
Abstract

Significance Statement
We discuss the case of a patient presenting with intractable vertigo and new maximal conductive hearing loss immediately on awakening from a temporomandibular joint arthroscopy. High-resolution computed tomography and a subsequent middle ear exploration confirmed a fractured stapedial footplate and perilymphatic fistula, presumably secondary to forceful external auditory canal packing, which is routinely done during temporomandibular joint (TMJ) arthroscopy. This case calls for heightened awareness of potential otologic complications during arthroscopic surgery.
An otherwise healthy 49-year-old woman with a history of congenital bilateral mild to moderate sensorineural hearing loss (SNHL) of unknown etiology was seen in our tertiary care otolaryngology clinic for severe vertigo, vomiting, and severe left-sided hearing loss immediately following left TMJ arthroscopy 1 week prior. Prior to her arrival, the patient’s symptoms failed to improve after an initial 7 day course of prednisone. She had no prior history of ear infections, otologic surgeries, noise exposure, or familial hearing loss. Otoscopy showed an intact tympanic membrane (TM), a well aerated middle ear, and a small amount of dry blood within the external auditory canal (EAC) along the posterior superior aspect, near the TM. Audiometry showed a severe to profound mixed hearing loss in the left ear with a mostly conductive component conductive hearing loss (CHL), with negative pressure on tympanometry (Figure 1A and B).
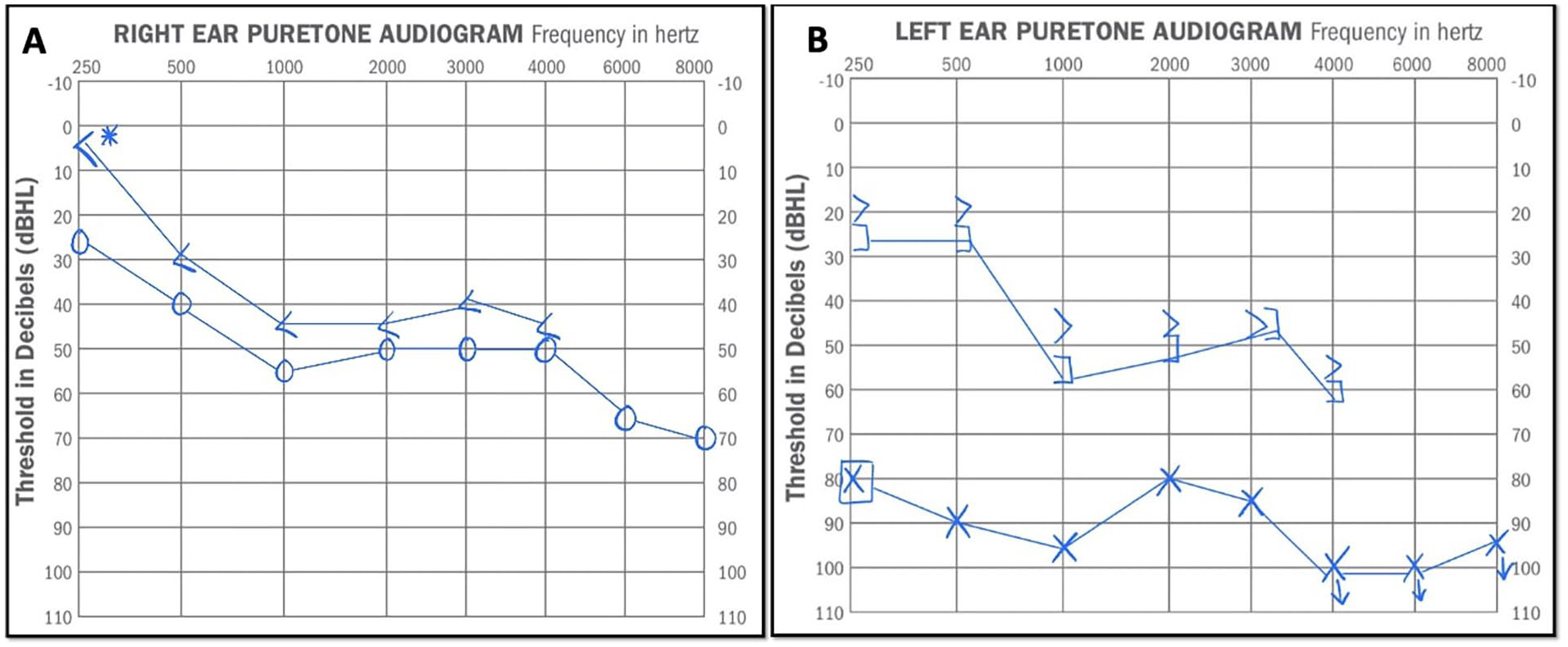
Audiometry test: (A) moderately to severe predominantly SNHL in right ear from 250-8k Hz; (B) severe to profound mixed hearing loss in left ear from 250-8k Hz. SNHL, sensorineural hearing loss.
A high-resolution computed tomography (CT) scan of the temporal bone revealed abnormal density and slight opacification at the oval window, with mild inward displacement of the stapes of approximately 1 mm, suggesting potential stapes dislocation (Figure 2).
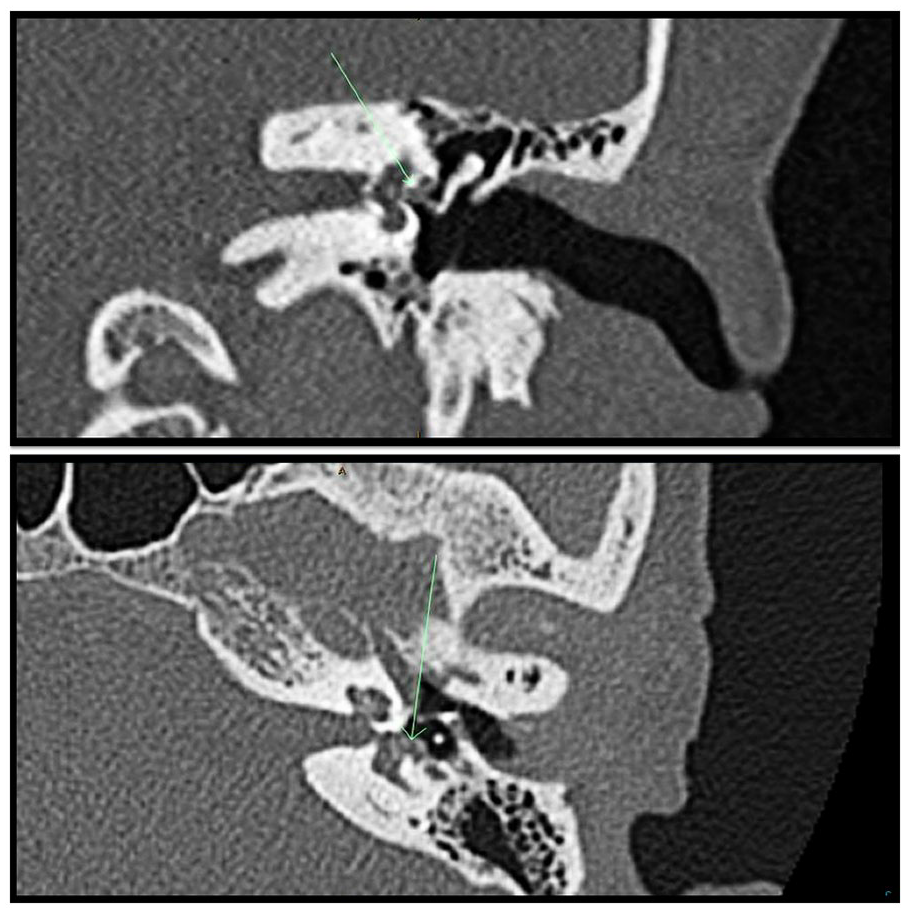
CT of temporal bone showing mild inward displacement of stapes. CT, computed tomography.
Despite a second course of oral steroids and numerous vestibular suppressant trials, the patient continued to have intractable vertigo leaving her incapacitated. Two weeks after her TMJ arthroscopy, the patient underwent an endoscopic middle ear exploration (MEE), revealing a fractured stapedial footplate and anterior crura (Figure 3). A Valsalva maneuver revealed a small amount of clear fluid leaking from the vestibule, confirming our suspicion of a perilymphatic fistula, which was repaired using perichondrium and fat. We hypothesize that stapedial injury and subsequent perilymphatic fistula in the absence of TM perforation most likely resulted from mechanical injury secondary to blind and forceful EAC packing. On discussing with the maxillofacial surgeon, it was reported that on each case the external ear is packed blindly with gauze using a foreceps.
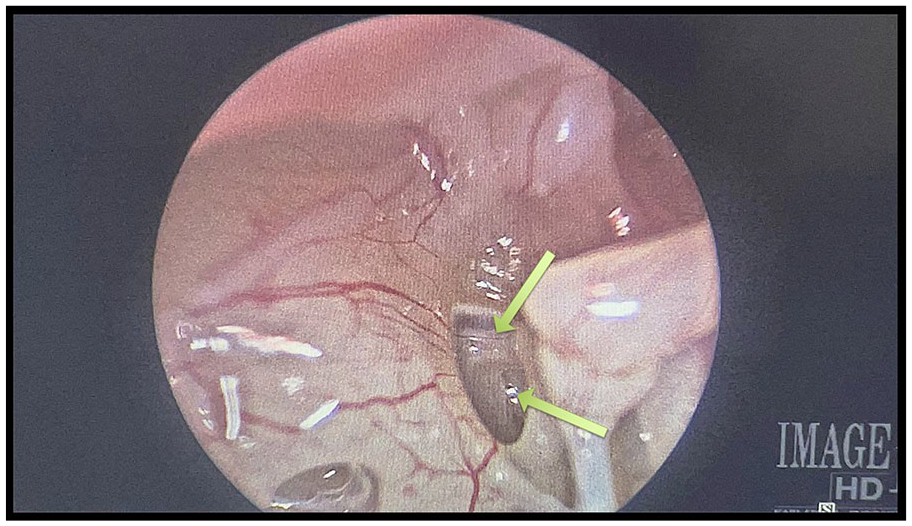
Fracture of stapedial footplate and anterior crura of stapes.
At last follow-up 3 months postoperatively, she noted improvement in vertigo. She was sent to vestibular rehabilitation for a remnant disequilibrium. No attempt was made to improve hearing, although this may be considered after repeat audiometry in 6 months time.
TMJ arthroscopy is a minimally invasive procedure which has established itself as a safe and reliable surgical modality for the diagnosis and treatment of various temporomandibular disorders.1-3 Very few otologic complications have been reported in the literature. 4
EAC lacerations are among the more common otologic adverse events, while middle and inner ear injury are seldom reported. 5 Chowdhury et al analyzed complications in 50 patients who underwent unilateral TMJ arthroscopy, reporting on 4 patients (8%) having experienced otologic adverse events. 6 This included 3 EAC lacerations, and 1 case of transient CHL after surgery due to a middle ear effusion. 2 Tsuyama et al similarly reported 24 otologic complications in 301 patients having undergone a TMJ arthroscopy (8%): 16 blood clots or lacerations to the EAC noted intraoperatively, 5 cases of postoperative hearing loss, 2 cases of ear fullness, and 1 patient developed severe vertigo. 7 In contrast to the high rates of otologic complications observed in the aforementioned studies, González-García et al reported an otologic complication rate of <1%. 4
Few cases in the literature draw similarities to our case, with ossicular chain and inner ear injury. Applebaum et al reported 3 cases of severe otologic injury in open and arthroscopic TMJ procedures, including 2 cases of severe to profound SNHL and vestibular injury due to suspected penetrating injury to the inner ear, and a case of incus dislocation with resulting CHL and complete facial nerve injury. 5 Similar to our case, Khandalavala et al described severe mixed unilateral hearing loss in a 35-year-old woman due to a fractured stapes and a perilymphatic fistula following arthroscopy, suspected to be caused by a defect of the coblation device. 8 In reviewing the literature, a membranous stapes footplate has been proposed as a novel diagnosis that could potentially predispose patients to such injuries.9,10
Various mechanisms of EAC injury and associated mitigation strategies have been proposed, including inadvertent mispositioning of the trocar, which can be avoided by directing the arthroscope away from the EAC wall and cautious packing to prevent lacerations or TM perforations. 6
We report a case of severe injury followed by TMJ arthroscopy. This case brings awareness of the possible effects of the packing used to protect the ear, which needs to be placed with great caution.
Footnotes
Author Contributions
Conceptualization, E.K.R.; methodology, S.K., K.S.K., C.F.R., and E.K.-R.; resources, S.K.; writing—original draft preparation, S.K.; writing—review and editing, S.K., K.S.K., C.F.R., and E.K.R.; visualization, E.K.R.; supervision, E.K.R.; project administration, E.K.R.; all authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent Statement
We confirm that we have obtained written informed consent from the patient for the publication of this case report, including any individual details, images, or videos contained within.