
Abstract
We report an extremely rare case with bilateral horizontal semicircular canal (HSC) dysplasia presenting as hearing loss with recurrent vertigo mimicking Meniere’s disease in a previously healthy 49-year-old male patient. HSC malformation is one of the common isolated developmental anomalies of the bony labyrinth usually associated with varying degree of hearing loss. He suffered from recurrent episodes of vertigo lasting more than 20 minutes accompanied by left hearing loss and tinnitus for 3 years. Pure-tone audiometry revealed a mild to moderate hearing loss at low frequencies in the left ear. Bithermal caloric testing revealed significant left-sided canal paralysis, but other vestibular testing was normal. Computerized tomography (CT) of the temporal bone showed the left HSC hypoplasia lacking a central bony island fused together with an enlarged vestibule, and right dysplasia, finally diagnosed with bilateral HSC dysplasia. Meniere’s disease-like recurrent vertigo attack and hearing loss were suspected to be caused by subsequent endolymphatic hydrops which could be due to HSC dysplasia.
Introduction
The dysplasia of the horizontal semicircular canal (HSC) is one of the most common inner ear malformations since it is the final vestibular structure to develop during inner ear embryogenesis. 1 As such, depending on the time point of the problems of a developmental process, HSC dysplasia may occur alone or in combination with other vestibular, cochlear, vestibular aqueduct, or middle ear malformations.2,3 With the development of imaging modalities, such inner ear malformation can be easily detected by temporal bone computerized tomography (CT) scan and/or magnetic resonance imaging (MRI). 4 HSC dysplasia is found in varying degrees, from the most severe form of aplasia to hypoplasia, which includes dilatation and shortened or narrowed HSC. 1 The hearing of patients with HSC dysplasia varies from normal to severe sensorineural hearing loss. 2 It is known that HSC dysplasia do not frequently induced vestibular symptoms such as vertigo or dizziness, and even when abnormal findings are identified in vestibular function test, they have been reported to be asymptomatic or mild.5,6 In the present report, we would like to present an extremely rare case with bilateral HSC dysplasia with recurrent vertigo attack with hearing loss mimicking definite Meniere’s disease.
Case Presentation
A 49-year-old man visited the outpatient clinic of the Department of Otorhinolaryngology, Chosun University Hospital, complaining of a recurrent vertigo attack that began 3 years ago. At the time of his first attack, the vertigo lasted more than 2 hours without no other cochlear symptoms. Three years later, he experienced 2 more vertigo attacks lasting more than 30 minutes, accompanied by hearing loss and tinnitus on the left side. At that time, almost all the vestibulocochlear symptoms disappeared completely within 2 days, so he did not visit the hospital. He visited our hospital 1 month after his last vertigo attack for further evaluation and did not complain of any other vestibulocochlear symptoms at the time of the visit. Pure-tone audiometry revealed mild to moderate left hearing loss at low frequency (Figure 1). The Bithermal caloric test showed left-sided canal weakness of about 42%, and other vestibular testing including the video head impulse test, and cervical/ocular vestibular myogenic potentials were within normal limits. The diagnosis of Meniere’s disease was made based on the patient’s clinical history and pure-tone audiometry, according to the Barany Society’s diagnostic criteria for Meniere’s disease. 7 A temporal CT revealed bilateral HSC dysplasia (Figure 2). The left side showed hypoplastic HSC lacking a central bony island, while the right showed mild dysplastic HSC (Figure 2).
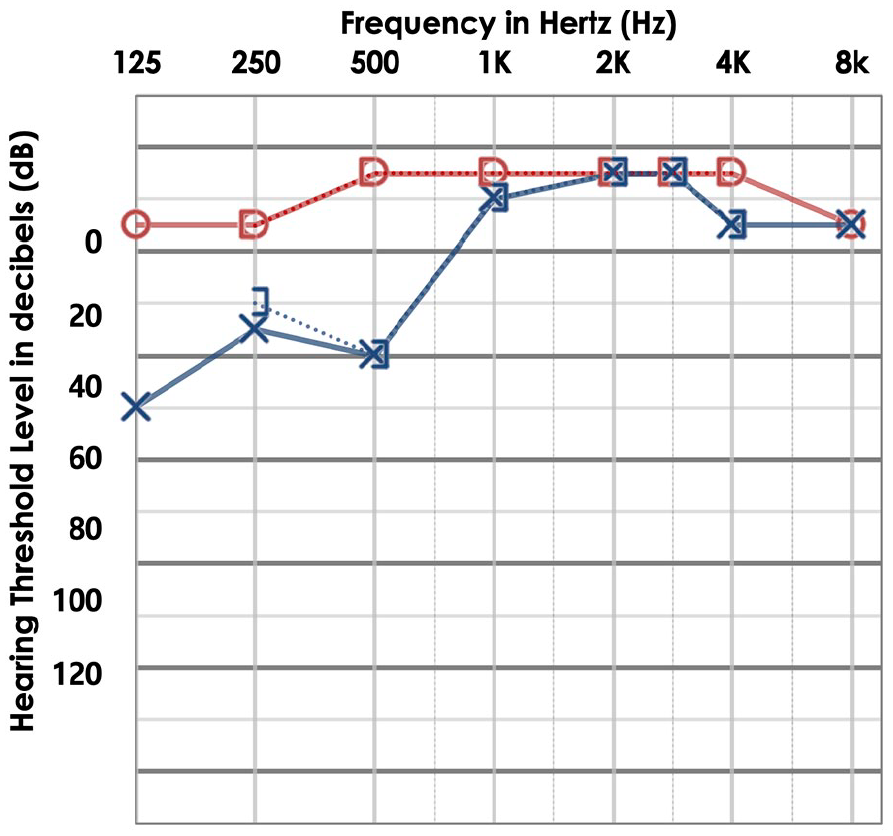
The pure-tone audiometry showed mild to moderate left low-tone hearing loss in a 49-year-old patient with bilateral horizontal canal dysplasia presenting with recurrent vertigo mimicking Meniere’s disease.
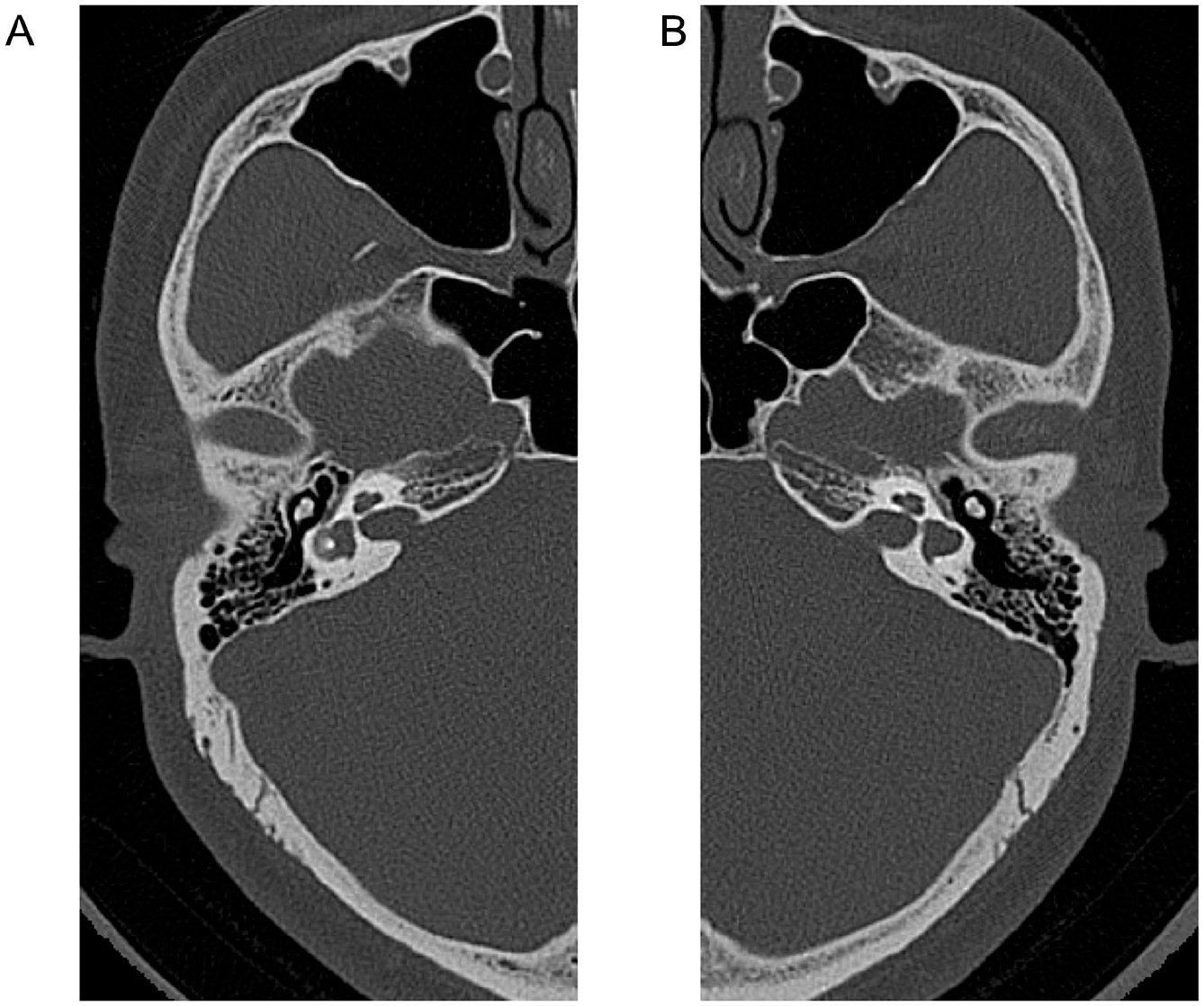
Temporal bone computed tomography image of bilateral HSC dysplasia in a patient who suffering recurrent vertigo attack and left hearing loss. The right side (A) showed HSC dysplasia and the left side (B) showed HSC hypoplasia fused together with an enlarged vestibule. HSC, horizontal semicircular canal.
Discussion
This case firstly showed spontaneous acute vestibular syndrome like vestibular neuritis and later Meniere’s disease-like episodic vertigo with aural symptoms such as hearing loss and tinnitus. In spite of such a complicated history, this case was finally identified as bilateral HSC dysplasia without other inner ear deformity by means of temporal bone CT scan. This case report suggests that even in patients with definite Meniere’s disease, 7 efforts should be made to confirm the presence of inner ear anomalies by CT or MRI. The HSC is the most frequently affected canal of inner ear anomalies because it is the final vestibular structure to be formed during inner ear embryogenesis.1,2,6 Previous literature showed various degrees of hearing loss in patients with HSC dysplasia, even in some cases displaying normal hearing.8,9 On the other hand, it has been reported that vestibular symptoms are not common in HSC dysplasia, and there is a lack of correlation between the degree of dizziness and the severity of the deformities.5,6 It is understood that deformities of the bony labyrinth do not necessarily indicate abnormalities in vestibular function. 6 To date, there are no definitive statements on the treatment of HSC dysplasia, and if vestibular symptoms are present, it is reasonable to select modalities that selectively target the vestibular system.
We would like to discuss how the case of bilateral HSC dysplasia can share clinical manifestations with definite Meniere’s disease. Maekawa et al reported a case of HSC dysplasia fused together with an enlarged vestibule on the left side which was accompanied by recurrent vertigo attacks like Meniere’s disease with normal hearing. 10 They described the mechanism of Meniere’s like vertigo attack in HSC dysplasia by indirectly demonstrating endolymphatic hydrops by performing bithermal caloric test before and after the furosemide injection. 11 The other previous studies report recurrent episodes of short-duration vertigo-like benign paroxysmal positional vertigo in patients with HSC dysplasia which suggest that the otolith in the deformed utricle might be transferred into the fused space of HSC, resulting in cupula deviation.10,12 Although endolymphatic hydrops was not demonstrated in our case, it is meaningful to note that ipsilesional hearing loss with recurrent vertigo was identified, providing a more definitive case of Meniere’s disease in bilateral HSC dysplasia.
Footnotes
Acknowledgements
The present study was supported by grants from the Clinical Medicine Research Institute at Chosun University Hospital (2021).
Author Contributions
Conceptualization: W.B. Data curation: Y.J.L. Formal analysis: W.B. Funding acquisition: G.S.N. Investigation: G.S.N. Methodology: W.B. Supervision: G.S.N. Validation: G.S.N. Visualization: G.S.N. Writing—original draft: W.B. Writing—review and editing: G.S.N.
Data Availability Statement
The data that support the findings of this article are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Our institution does not require ethical approval for reporting individual cases or case series.
Patient Consent
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.