
Abstract
This is a case report on the treatment of tracheal glomus tumor, which is a rare tumor originating from the glomus bodies in the trachea and form spherical or nodular masses. These tumors can lead to obstruction and narrowing of the tracheal lumen, causing symptoms such as dyspnea. The standard treatment for tracheal glomus tumors is typically surgical resection. In this case, the patient underwent a procedure involving low tracheostomy with closure of the airway and mechanical ventilation through the stoma, followed by endoscopic-assisted subglottic tracheal glomus tumor resection using plasma-assisted radiofrequency.
Case Report
A 29-year-old male patient presented to our hospital with a 2 year history of recurrent irritative cough, which had worsened over the past 3 months and was occasionally accompanied by hemoptysis. Initially, he experienced an unexplained irritative cough without sputum or hemoptysis, occasionally dyspnea post-activity, but no fever or chest pain. However, his condition deteriorated over the past 3 months, with exacerbation of cough, production of thick white sputum, intermittent hemoptysis, and dyspnea post-activity. Evaluation in our respiratory department revealed a subglottic tracheal mass on pulmonary computed tomography (CT) scan and bronchoscopy, later confirmed histopathologically as a hemangioma, leading to surgical intervention. The patient denied any history of chemical or radiation exposure, tobacco or alcohol use, and had no family history of similar disorders.
On Admission
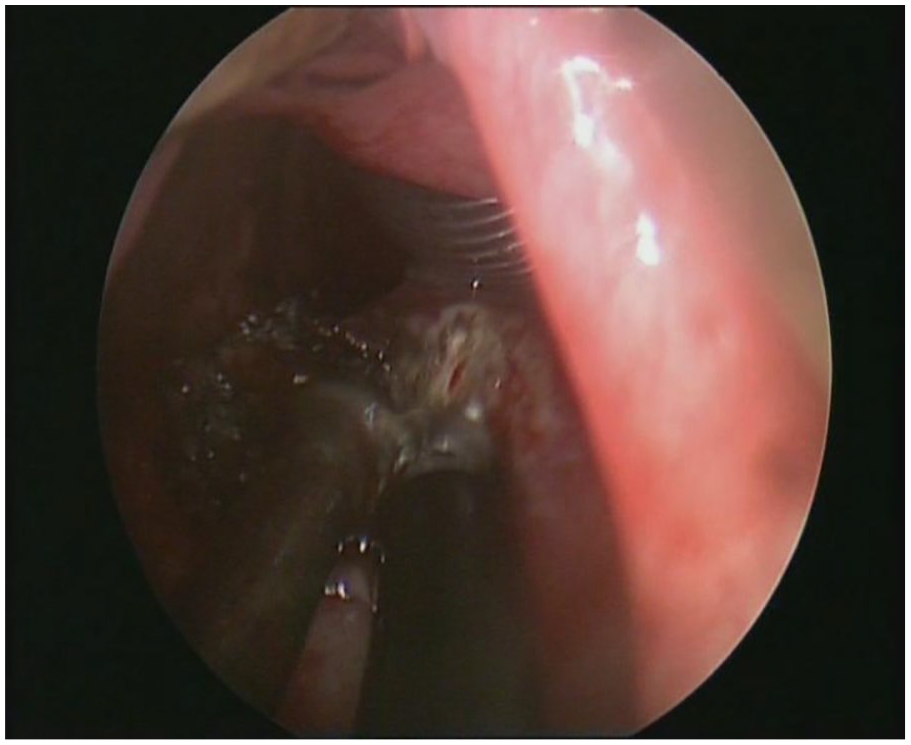
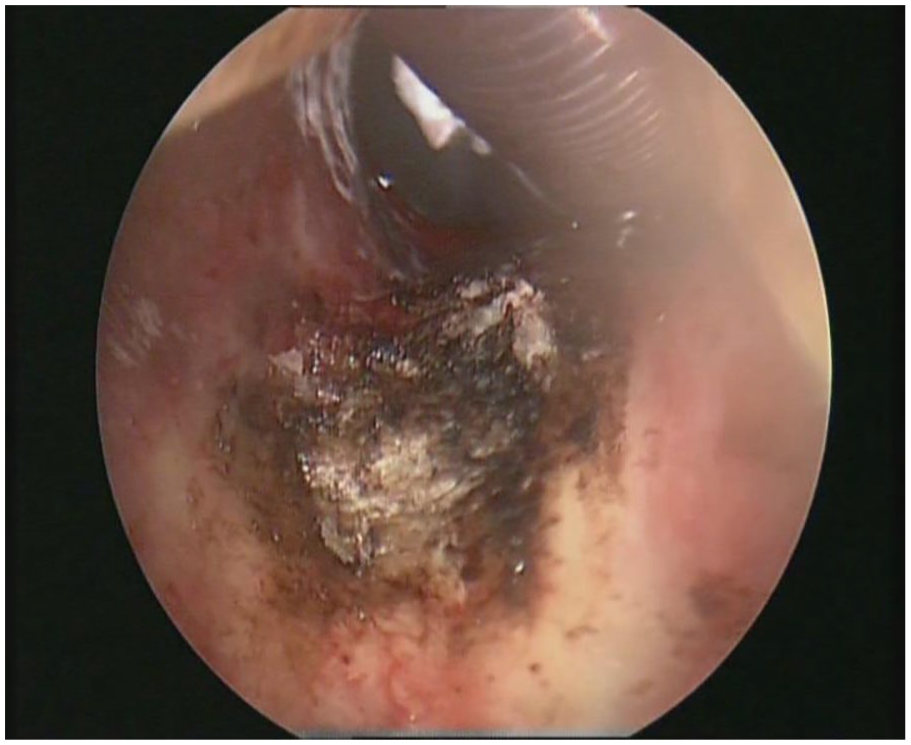
The patient demonstrated a sound mental state, fluent speech, and no physical signs of illness. Inspiratory stridor was noted during auscultation of the throat, while lung examination was unremarkable. Bronchoscopy revealed a cauliflower-like lesion protruding 1 cm below the vocal cords into the lumen, causing focal airway narrowing (Figure 1). A biopsy was performed at the prominent site of the mass, followed by hemostasis using a high-frequency electric knife. The pathology report indicated immunohistochemistry findings consistent with a diagnosis of glomus tumor (Figure 2). Chest and cervical CT scans showed a nodular soft tissue lesion measuring approximately 14 mm × 18 mm with a CT attenuation value of 30 HU on the trachea’s left posterior wall at the thoracic inlet’s level. The trachea demonstrated notable crescent-shaped narrowing at this level, with a diameter of 6 mm. Contrast-enhanced imaging revealed pronounced enhancement of the nodular lesion on the left posterior wall of the trachea, characterized by well-defined borders and homogeneous density (Figures 3 and 4).

The presence of a mass seen under bronchoscopy.
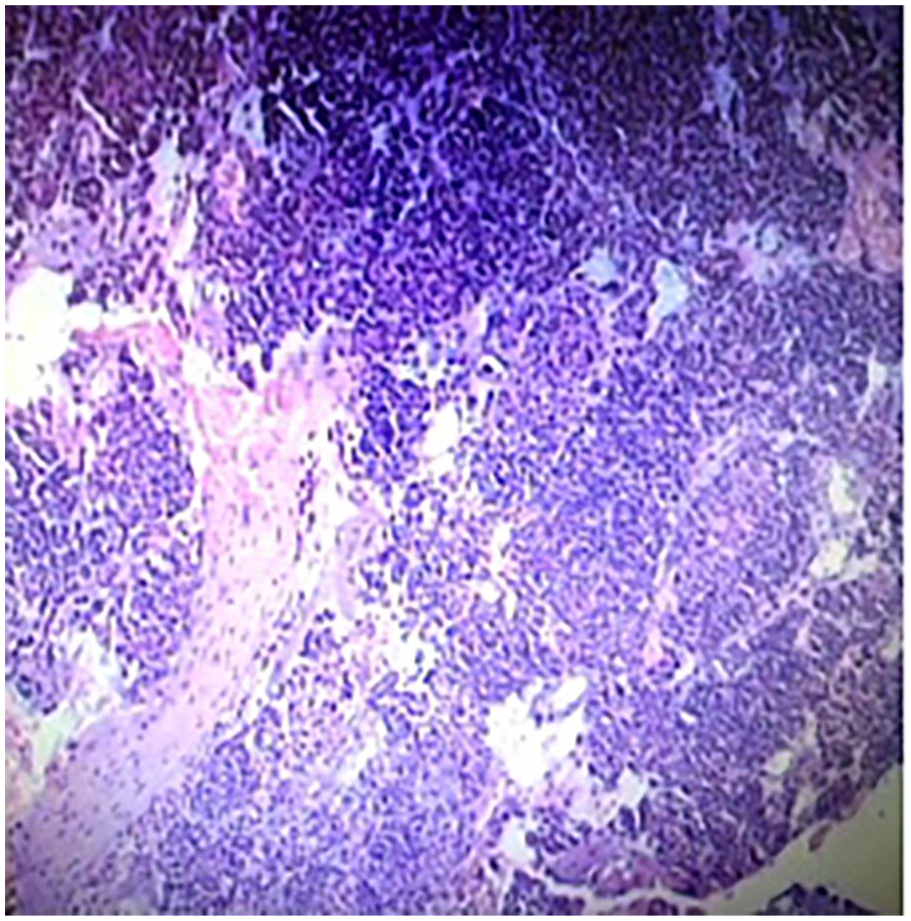
Pathological biopsy of the mass.
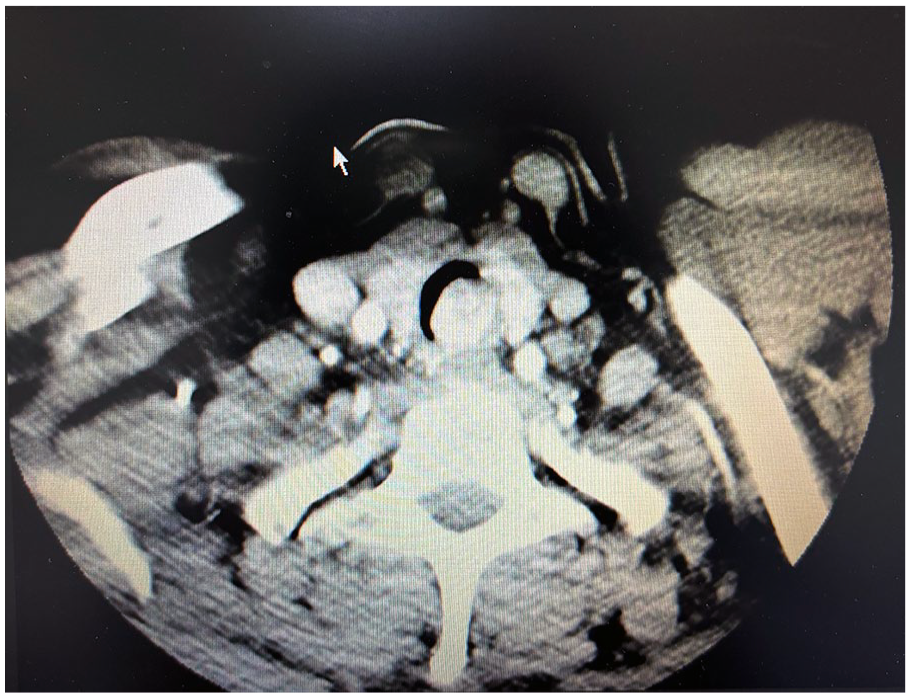
Cervical axial CT. CT, computed tomography.
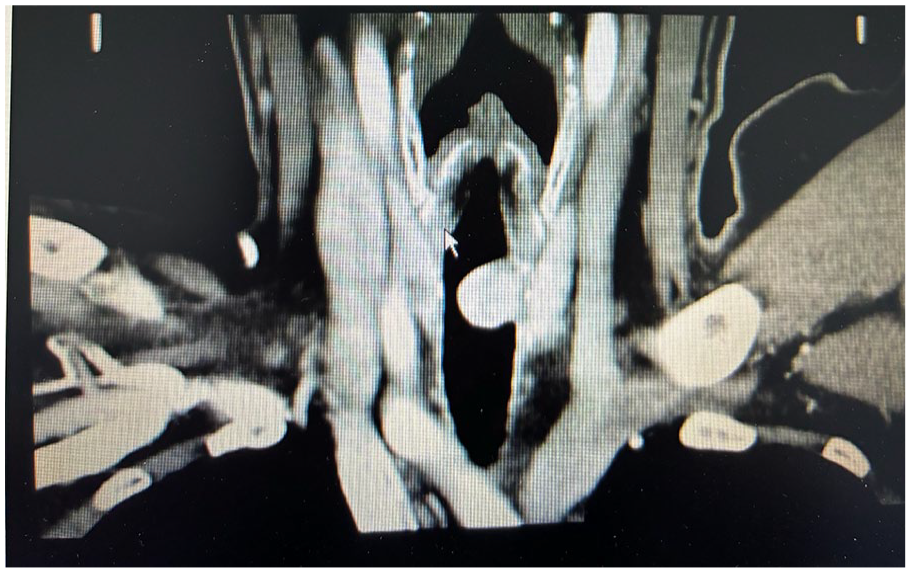
Cervical coronal CT. CT, computed tomography.
Surgery and Postoperative Details
The procedure began with local anesthesia and involved a low cervical tracheostomy, later transitioning to general anesthesia. A cervical fistula was created to aid mechanical ventilation support. During laryngoscopy, smooth vocal cord surfaces were observed bilaterally, and a pinkish mass approximately 1.5 cm in diameter was identified just below the glottis. The mass had distinct margins and firm consistency, which tended to bleed on palpation. The mass was carefully excised using an 8870-plasma radiofrequency knife, starting from its upper margin, while bipolar electrocautery was used for simultaneous coagulation to control bleeding.
Furthermore, bipolar electrocoagulation was used to cauterize the tumor base repeatedly for comprehensive treatment (Figures 5 and 6). The surgery went smoothly, and the subsequent examination showed no residual mass or active bleeding. No incidental structural damage occurred during the procedure. Subsequently, the cervical tracheostomy tube was replaced with a size 8 plastic tube, and the patient was transferred back to the ward. Standard post-tracheostomy care was provided to prevent infections. The patient had occasional irritative coughing after the surgery, without any episodes of coughing up blood. On the first day after surgery, a physical examination revealed secure fixation of the tracheostomy tube with the cuff deflated and no signs of redness, swelling, or abnormal discharge around the incision site. Subcutaneous emphysema was observed on the right side of the neck, extending from the submandibular region to the clavicle. Electronic laryngoscopy showed smooth vocal cord surfaces and regular movement, with the previously identified mass below the glottis now absent. Only a tiny amount of blood crust and fibrinous exudate remained at the base of the original mass (Figure 7). Oral antitussive medication was given to relieve coughing, and the patient’s subcutaneous emphysema did not worsen. On the fifth day after surgery, it was decided to remove the tracheostomy tube and seal the tracheostomy fistula with butterfly adhesive tape. However, 2 days later, there was no evidence of closure at the tracheostomy fistula, and phlegm and air leakage were still present.
Intraoperative excision using a plasma knife.
Only blood crust seen after complete excision of the mass.

Two weeks postoperatively, only fibrinous exudate was observed at the base of the original lesion.
Consequently, on the seventh day after surgery, under local anesthesia, the tracheostomy fistula was debrided and sutured. Over the next 2 days, there were no signs of infection at the sutured site, and no gas leakage was observed. The patient reported no coughing, expectoration, or blood-tinged sputum and had unobstructed breathing with the disappearance of stridor. In the second week after surgery, electronic laryngoscopy showed satisfactory recovery in the surgical area (Figure 7), with complete resolution of subcutaneous emphysema. Postoperative follow-up was performed as scheduled, and no recurrence was observed during the 8 year postoperative period, demonstrating excellent recovery (Figure 8).
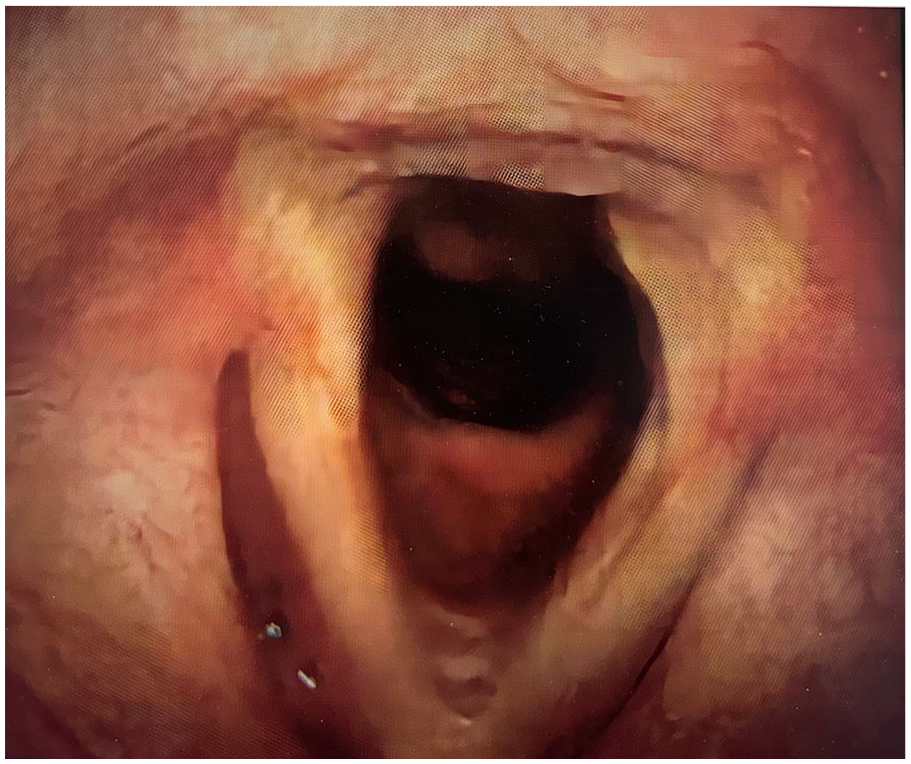
No recurrence for 8 years postoperatively, with normal morphology.
Discussion
The glomus tumor originates from aberrant smooth muscle cells within arteriovenous anastomoses, constituting approximately 2% of soft tissue tumors. 1 It is associated with peripheral blood vessel constriction, blood flow regulation, and temperature control. The disease commonly affects these areas due to the prevalence of arteriovenous anastomoses in the extremities, particularly at the distal ends, such as the nail beds. 2 In addition, occurrences have been reported in other locations, including the stomach, kidneys, nasal cavities and sinuses, thoracic vertebrae, abdominal rectus muscles, and vascular pericyte tissues within cardiac organs. Airway glomus tumors are sporadic and can occur in the pulmonary parenchyma, tracheobronchial tree, and sinuses, with tracheal glomus tumors being predominant. Tracheal glomus tumors mainly occur in adults, with a higher prevalence in males than in females. They are predominantly benign, with fewer than 1% malignant glomus tumors. The main clinical manifestations of this condition include paroxysmal coughing and coughing up blood-tinged sputum. Stridor may occur after vigorous activity, while respiratory distress is less common, likely due to the benign nature of most tumors, which tend to grow slowly. Chest X-ray examination has poor sensitivity, while lung CT can show intratracheal masses, with uniform mass enhancement after contrast administration. The diagnosis of glomus tumors mainly relies on pathological examination and immunohistochemical analysis. In histopathology, tumor tissue exhibits blood vessels of various sizes surrounded by medium-sized, clear-bordered, round, or polygonal cells. The tumor cells have slightly more prominent, round, and regular nuclei with slightly acidophilic or transparent cytoplasm. Immunohistochemical staining shows positive expression of smooth muscle actin and vimentin, with negative expression of neuroendocrine and epithelial markers. Malignant glomus tumors are also sporadic. Folpe et al proposed diagnostic criteria for them 3 : (1) Tumor diameter >2 cm, located within the fascia or parenchymal organs; (2) atypical mitotic figures are visible; and (3) nuclei exhibit marked pleomorphism, with >5 mitotic figures per 50 high-power fields. Since the depth of tumor invasion into the trachea is an essential indicator for distinguishing between benign and malignant tumors, complete and thorough resection of tracheal glomus tumors is theoretically necessary. 4 Therefore, tracheal sleeve resection is currently considered the optimal treatment for this condition. However, in this case, the tumor’s location is rather unusual. Enhanced neck CT imaging reveals that the tumor is situated 1.0 cm below the glottis, between the cricoid cartilage and the second tracheal ring. In this scenario, performing a tracheal sleeve resection would pose challenges in anastomosing the distal trachea with the cricoid cartilage. 5 In this case, our department adopted a procedure involving low tracheostomy for fistula creation, followed by mechanical ventilation after airway closure. Under endoscopic support, plasma radiofrequency was used to assist in the excision of the tracheal glomus tumor below the vocal cords. This surgical approach not only ensures the patency of the lower respiratory tract and prevents blood aspiration during surgery but also utilizes the coagulation function of plasma to reduce intraoperative bleeding effectively. Furthermore, plasma has a certain depth of action in the submucosal layer, reducing the risk of recurrence by removing visible tumors and targeting deeper tissues.
Conclusion
In summary, endoscopic-assisted excision of tracheal glomus tumors using plasma radiofrequency below the vocal cords provides a novel treatment approach for tumors in specific locations. However, since this procedure does not entirely remove the tracheal rings to which the tumor base is attached, there is a theoretical risk of recurrence. Close postoperative follow-up is essential, and the patient is currently under careful surveillance. This case underscores the efficacy of endoscopic-guided plasma radiofrequency-assisted therapy in managing tracheal hemangioma, highlighting its potential as a minimally invasive therapeutic modality. Further studies are warranted to explore its long-term outcomes and applicability in broader clinical settings.
Footnotes
Acknowledgements
We appreciate the teachers at Dalian Central Hospital’s medical records department who offered retrieval services at the beginning of the work.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is an observational study. The Research Ethics Committee of Dalian Municipal Central Hospital has confirmed that ethical approval is unnecessary.
Statement of Human and Animal Rights
Not applicable.
Informed Consent
Written informed consent was obtained from the patient for the study, and his anonymized information and clinic data will be published in this article.