
Abstract
Introduction
Local drug delivery is a popular therapeutic operation over the last few years, providing a reliable and predictable intracochlear delivery without negative side effects of systemic administration, with a high concentration of the therapeutic agent in the inner ear. 1 Intratympanic injection is the most available and general strategy used in the clinical practice of otological medicine. Large amounts of studies have shown that intratympanic steroid injection serves as an effective treatment in some common diseases, such as idiopathic sudden sensorineural hearing loss and Meniere’s disease.2-4 Intratympanic injection administration results in a higher concentration of therapeutic drugs in the middle ear, diffusion into the inner ear by contacting the round window (RW) membrane subsequently. 5 In clinical routine, although the therapy of intratympanic injection for inner ear disorders is widely accepted and practiced, however, intratympanic injection treatment effects vary occasionally. This almost may be due to the applied concentrations, releasing duration, and head position of post-operation.
Leakage of the injectate via the eustachian tube (ET) inevitably, as patients speaking, moving their heads, or swallowing saliva.6,7 As a consequence, a method of providing appropriate head position could benefit this therapy. However, up to now, there is no standardized definition for the optimal head placement following IT treatment. 8 In this study, we studied the position modifications of the ET orifice and RW with the head movement, and demonstrated the optimal head position (OHP) for the patients after IT injection, optimizing the drug diffusion by helping the drug retain in the middle ear in order to improve the therapy effect.
Methods
Subjects
The study received ethical approval from the Ethics Committee of the Eye & ENT Hospital of Fudan University (No. 2020118).
Twenty-two anonymized selected high-resolution computed tomography (HRCT) of 22 patients in our hospital from January 2022 to December 2022 were reviewed retrospectively. The selected patients had normal middle ear function and were investigated HRCT for sensorineural hearing loss, tinnitus, and other complaints, without history of otitis media, malformations of the middle and inner ear, and other organic diseases of the middle and inner ear. Patients aged from 5 to 70 years old with an average of 29 years old, 10 males included (45.5%). All subjects were standardized by age, divided into children (≤18 years, 11 subjects) and adult groups (>18 years, 11 subjects). 9
Scanning Method and Postprocessing
All the axial images were obtained with multidetector row computerized tomography (CT) (Sensation 16; Siemens Medical Systems, Forchheim, Germany) in the helical mode. Our scanning procedure followed the standard temporal bone imaging protocol. Scans were acquired with a tube voltage of 120 kV and a current of 180 mA. The images were reconstructed with 0.75-mm-thick sections, 0.5 mm increment, 512 × 512 matrix, 0.43 mm pixel size, and a display field of view of 22 × 22 cm. Images were displayed at a window center of 700 Hounsfield units (HU) and a window width of 4000 HU. Afterward, CT images were exported as Digital Imaging and Communications in Medicine (DICOM) files, and reconstructed the positioning data defined spatial coordinates in the directions of superior-inferior, anterior-posterior, and left-right. The DICOM data sets were imported into Mimics software (Materialise, Technologielaan Leuven, Belgium) for further image processing. This software allows users to view CT datasets simultaneously using a set of two-dimensional (2D) images and three-dimensional (3D) images for each dataset. The observation was performed with a contrast scale between 1024 HU (air) and 2000 HU (bone). All landmarks were defined on the boundaries or apexes of structures. The coordinates of landmarks were obtained from Mimics. Reference landmarks were highlighted as follows, the central point of RW, the central point of ET orifice, and the central point of foramen magnum. To investigate the changes in the position of the ET orifice with head movement, the coordinate values of the above landmarks were imported into a self-developed calculation program, EustachiantubeCalc, based on Matlab software (Matrix Laboratory, Natick, MA, USA).
Definition and Calculation of the Reference Plane
A spherical coordinate system was established with the center point of the foramen magnum as the origin. In this spherical coordinate system, the head could perform anteflexion and posterior extension in the midsagittal plane, as well as pronation and supination in the horizontal plane (the injected ear was turned to the front or back of the body, called pronation and supination, respectively).
The supine or standing position in the natural state of the patient was defined as the initial position. In these positions, the angles of anteflexion, posterior extension, pronation, and supination were all 0°. The position of supination and anteflexion was defined as positive angle, while the pronation and posterior extension were regarded as negative angle. As the patient kept in the supine position, a plane parallel to the coronal plane was drawn across the reference plane in the supine position. When the patient was in a standing position, a plane parallel to the horizontal plane was made 45 mm below the center point of foramen magnum as the reference plane of the standing position (Figure 1). The distances from the center point of ET orifice or the center point of RW to the reference plane were defined as distance of ET orifice (DET for short) and distance of RW (DRW), respectively (Figure 2). The DET and DRW at different angles of anteflexion, posterior extension, pronation, and supination were calculated and recorded. When the DET was higher than DRW in the direction of gravity and when the distance between the DET and DRW (or DET-RW) was the largest, it was the OHP for intratympanic injection.
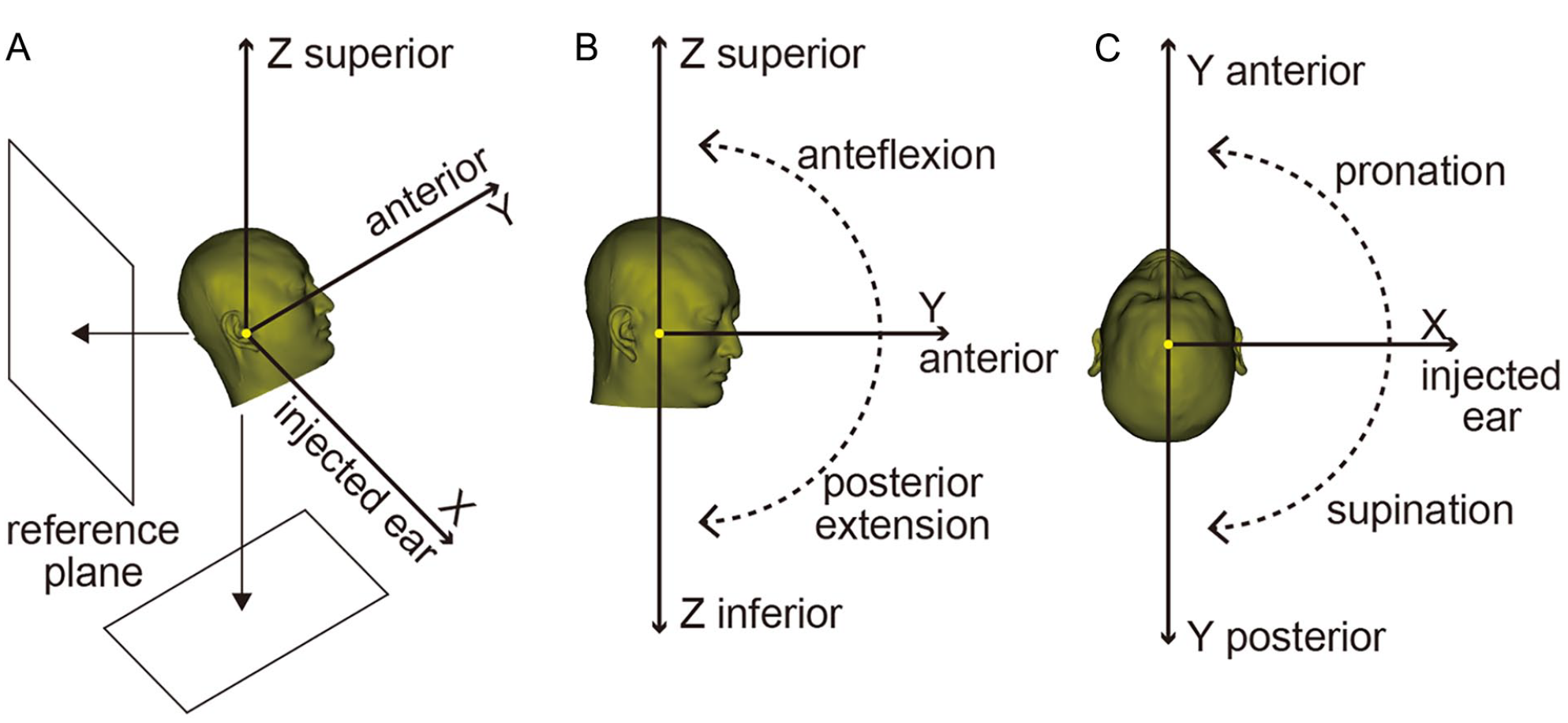
Schematic diagram of the method. (A) A spherical coordinate system was established with the center point of foramen magnum as the origin. (B) Side view. The head can perform anteflexion and posterior extension in the midsagittal plane. (C) Superior view. The head can perform pronation and supination in the horizontal plane. Yellow dots represented the center point of foramen magnum.
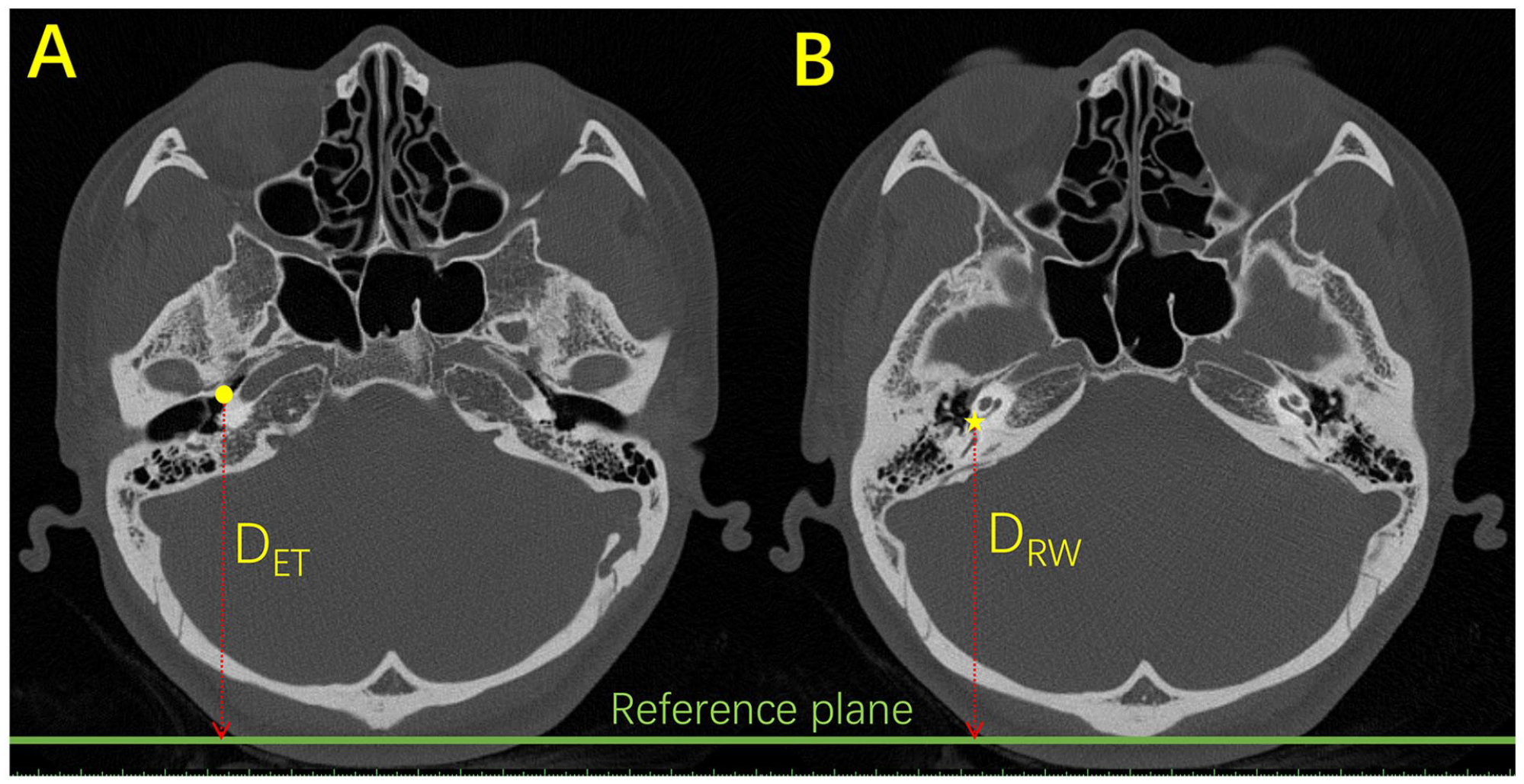
The CT axial images. (A) The yellow dot represented eustachian tube (ET) orifice, (B) The yellow pentagram represented round window (RW). The green line indicated the reference plane in the supine position. The distances from the center point of ET orifice or the center point of RW to the reference plane were defined as distance of ET orifice (DET for short) and distance of RW (DRW), respectively.
Statistical Analysis
The DET, DRW, and DET-RW were analyzed using SPSS® software (IBM, Armonk, NY, USA) version 20. Data were checked for normal distribution using the D’Agostino and Pearson normality test. An unpaired t-test was used to determine the effects on different analyzed distances under the various positions. The data were reported as mean ± standard deviation. Statistical significance was considered at P values less than .05.
Results
The relative positions of the ET and the RW in the direction of gravity were observed on four head movements, pronation, supination, anteflexion, and posterior extension. As the patient lay in a supine position, DET-RW was becoming greater at the range from 75° at pronation position to 38° in supination position (Figure 3A, P < .05). The OHP was achieved at a pronation of 16°, with a maximum DET-RW distance of 8.55 ± 1.82 mm. Whereas, as patients were instructed in the standing position, there was no significant difference in the aspect of DET and DRW, as the head exchange from pronation to supination (Figure 3C, P > .05). But in fact, the vertical height of the RW was higher than ET orifice in the position of standing.
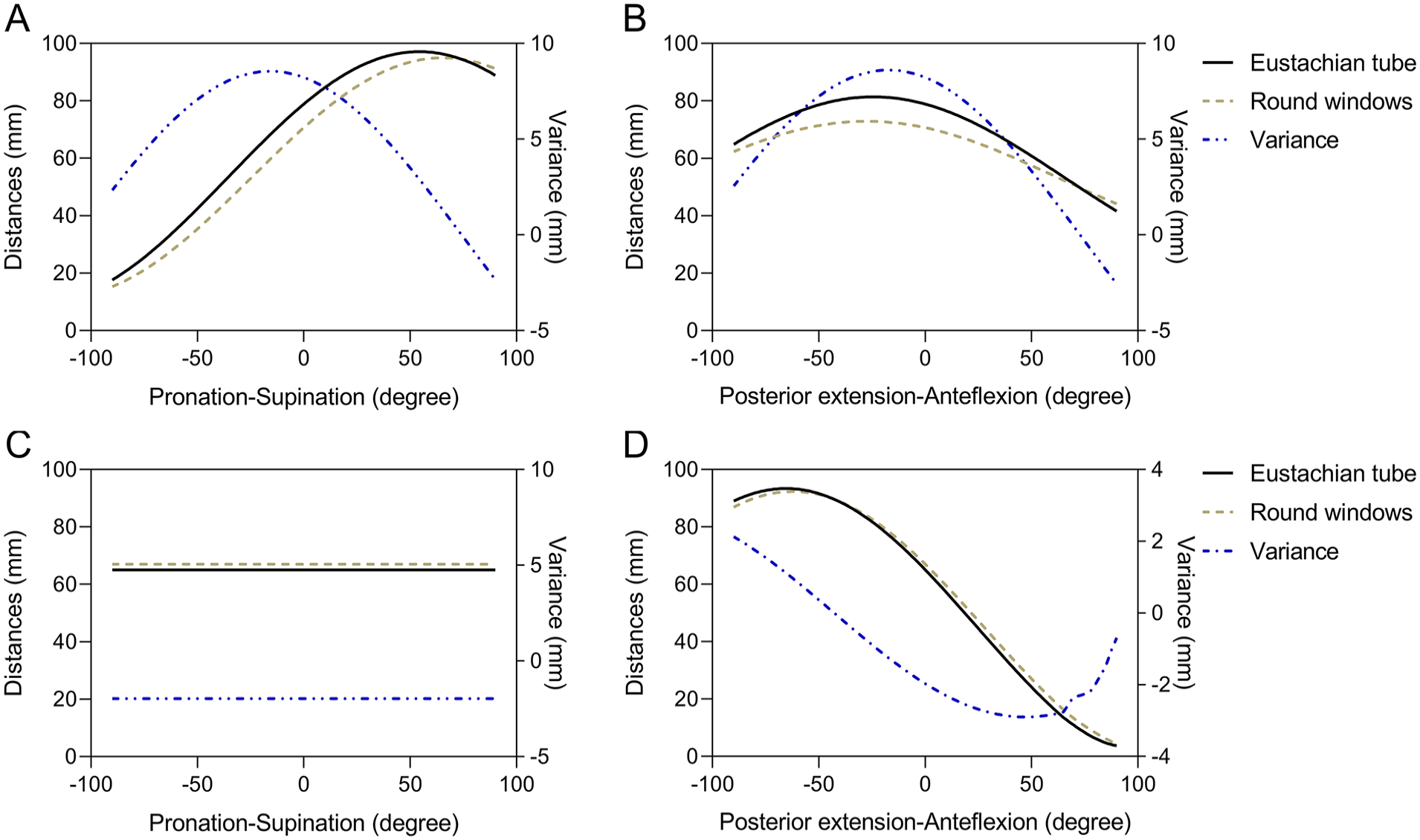
If the head only performed pronation and supination. In the supine position, (A) the DET was greater than DRW from pronation at 75° to supination at 38° (P < .05). The OHP (DET-RW = 8.55 ± 1.82 mm) was when the head was supination at 16°. (C) In the standing position, there was no head position where DET was greater than DRW. If the head only performed anteflexion and posterior extension. In the supine position, (B) the DET was greater than DRW from posterior extension at 63° to anteflexion at 6° (P < .05). When the head was posterior extension at 17°, it was the OHP (DET-RW = 8.61 ± 1.56 mm). In the standing position, (D) If the head only performed anteflexion and posterior extension: in the supine position, the head was posterior extension more than 43°, the DET was greater than DRW. When the head was posterior extension at 90°, it was the OHP (DET-RW = 2.13 ± 1.60 mm).
Further investigation was explored as the head position at anteflexion and posterior extension. As the patient was kept in the supine position, DET was found greater than DRW from a posterior extension at 63° to anteflexion at 6° (Figure 3B, P < .05). The OHP was observed in the posterior extension at 17°, and the DET-RW was 8.61 ± 1.56 mm. In the standing position, the DET exceeded DRW when the head underwent posterior extension beyond 43° (Figure 3D, P < .05), with the OHP at a full posterior extension of 90°, yielding DET-RW was 2.13 ± 1.60 mm.
Combining anteflexion and posterior extension along with pronation and supination, the OHP was noticed when the head pronation at 23° and posterior extension at 24° in the supine position, corresponding DET-RW was 9.29 ± 2.13 mm. Additionally, it was found that DET was greater than DRW (Figure 4D, P < .05), and DET-RW exceeded 8.61 mm (Figure 4D). In the standing position, DET was observed to be greater than DRW when the head underwent posterior extension of more than 43° (Figure 5D).
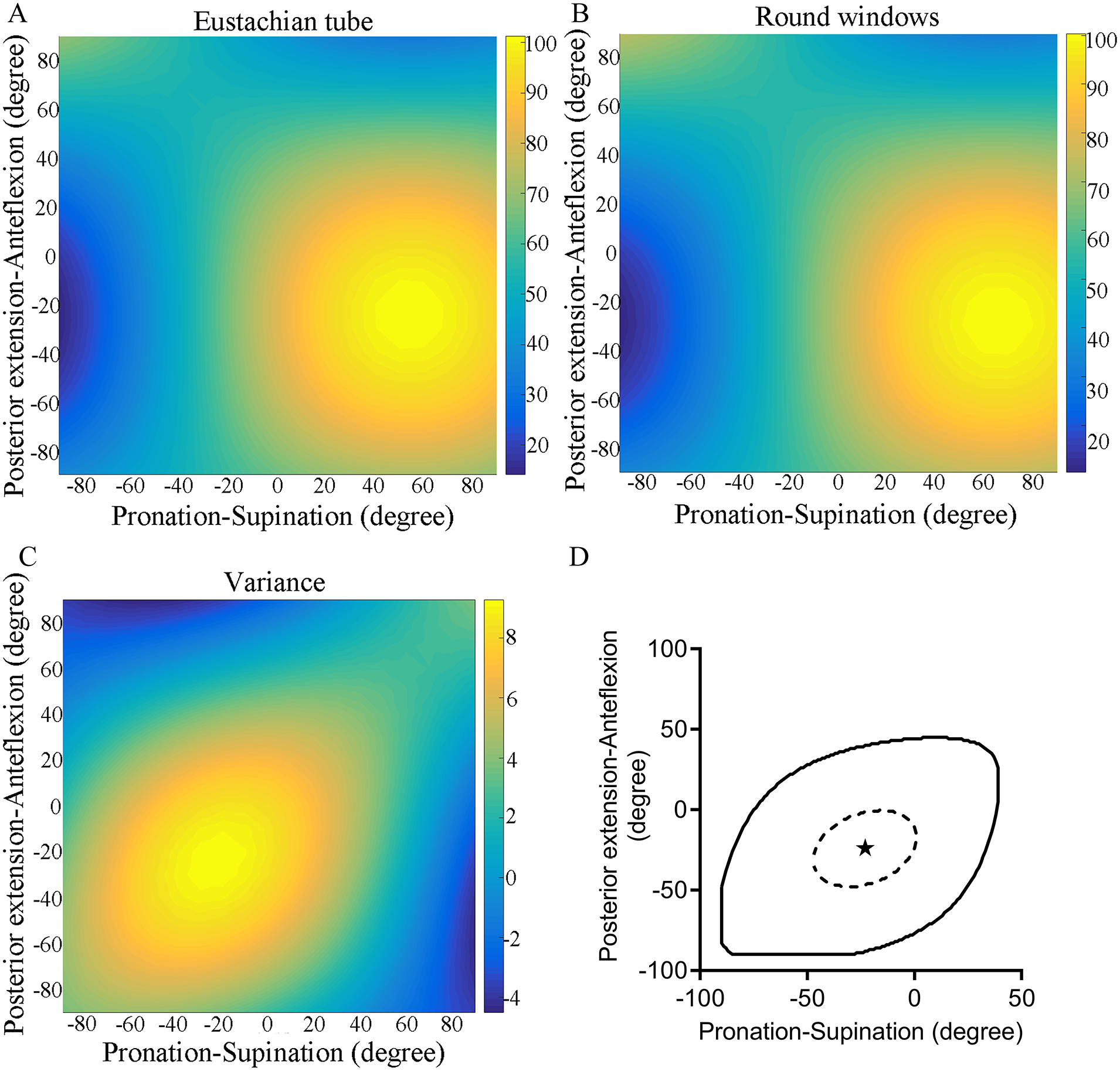
In the supine position. (A-C) The DET, DRW, and DET-RW were changed with head movement. (D) In the solid line range, DET was greater than DRW (P < .05). Within the range of the dotted circle, DET-RW was greater than 8.61 ± 1.56 mm. The OHP was at the asterisk (when the head was pronation at 23° and posterior extension at 24° in the supine position. DET-RW = 9.29 ± 2.13 mm).
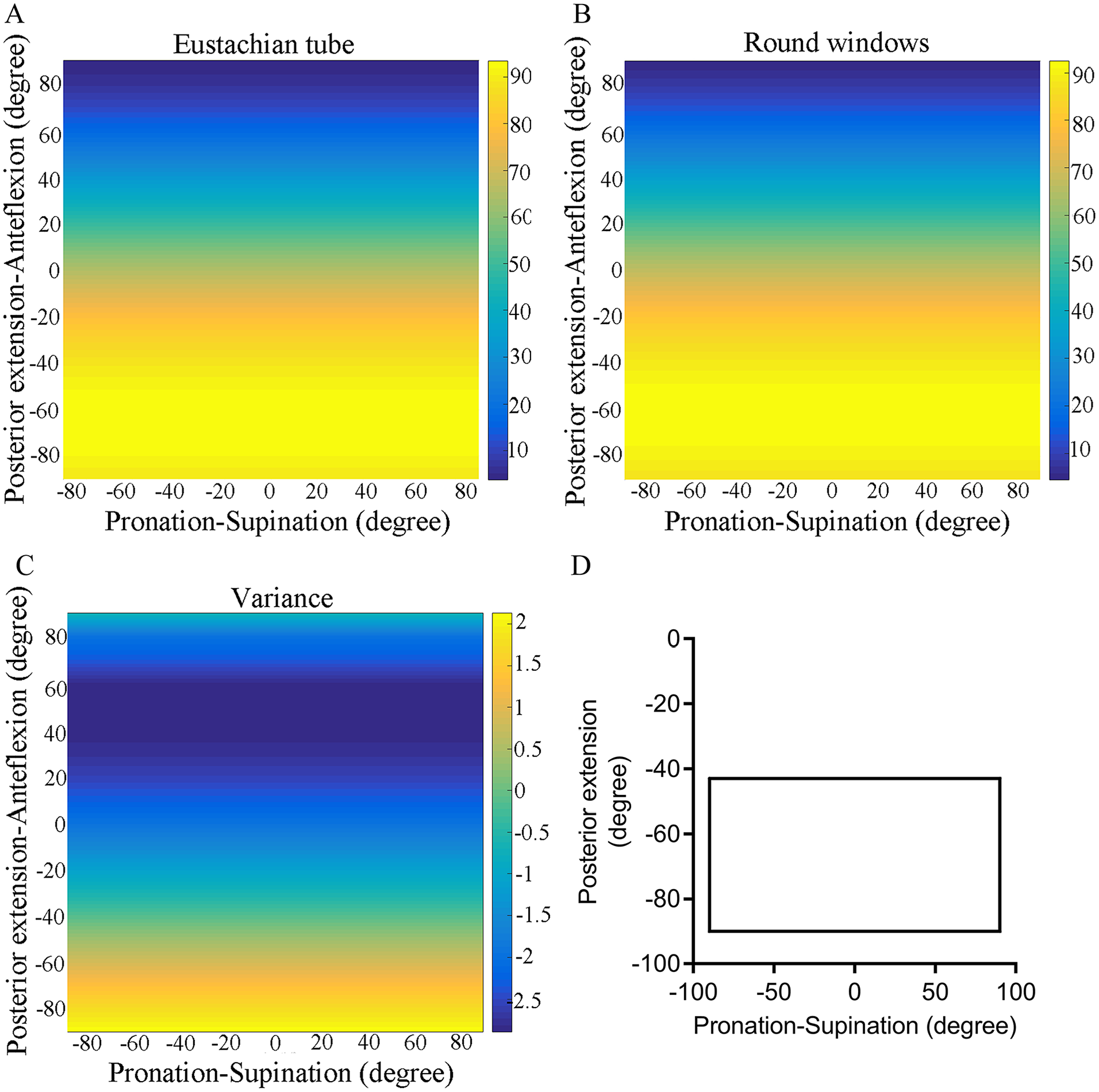
In the standing position. (A-C) The DET, DRW, and DET-RW were changed with head movement. (D) The DET was greater than DRW as long as the head was posterior extension more than 43°.
The subjects were comparable in age, under 18 and over 18 years old. As shown in Figures 6 and 7, the trend of the DET-RW presented consistently in the children and the adult group as the head engaged in pronation, supination, anteflexion, and posterior extension. In the supine position at pronation and supination, the OHP in the children group was the pronation of 15°, and in the adult group, was at the pronation of 16°, the DET-RW showed 8.05 ± 1.69 mm and 9.04 ± 1.87 mm respectively (Figure 6A). In the standing position, the vertical height of the RW was higher than ET orifice for both groups (Figure 6C). In the period of anteflexion and posterior extension at supine position, the OHP was the posterior extension of 17° in the children group (DET-RW = 8.10 ± 1.47 mm) and the posterior extension of 18° in the adult group (DET-RW = 9.13 ± 1.53 mm) (Figure 6B). In the standing position, the DET surpassed the DRW at a posterior extension beyond 51° for the children group and beyond 36° for the adult group (Figure 6D, P < .05). The OHP in both groups was a full posterior extension of 90°, resulting in a DET-RW of 1.77 ± 1.38 mm in the children group and 2.48 ± 1.57 mm in the adult group.
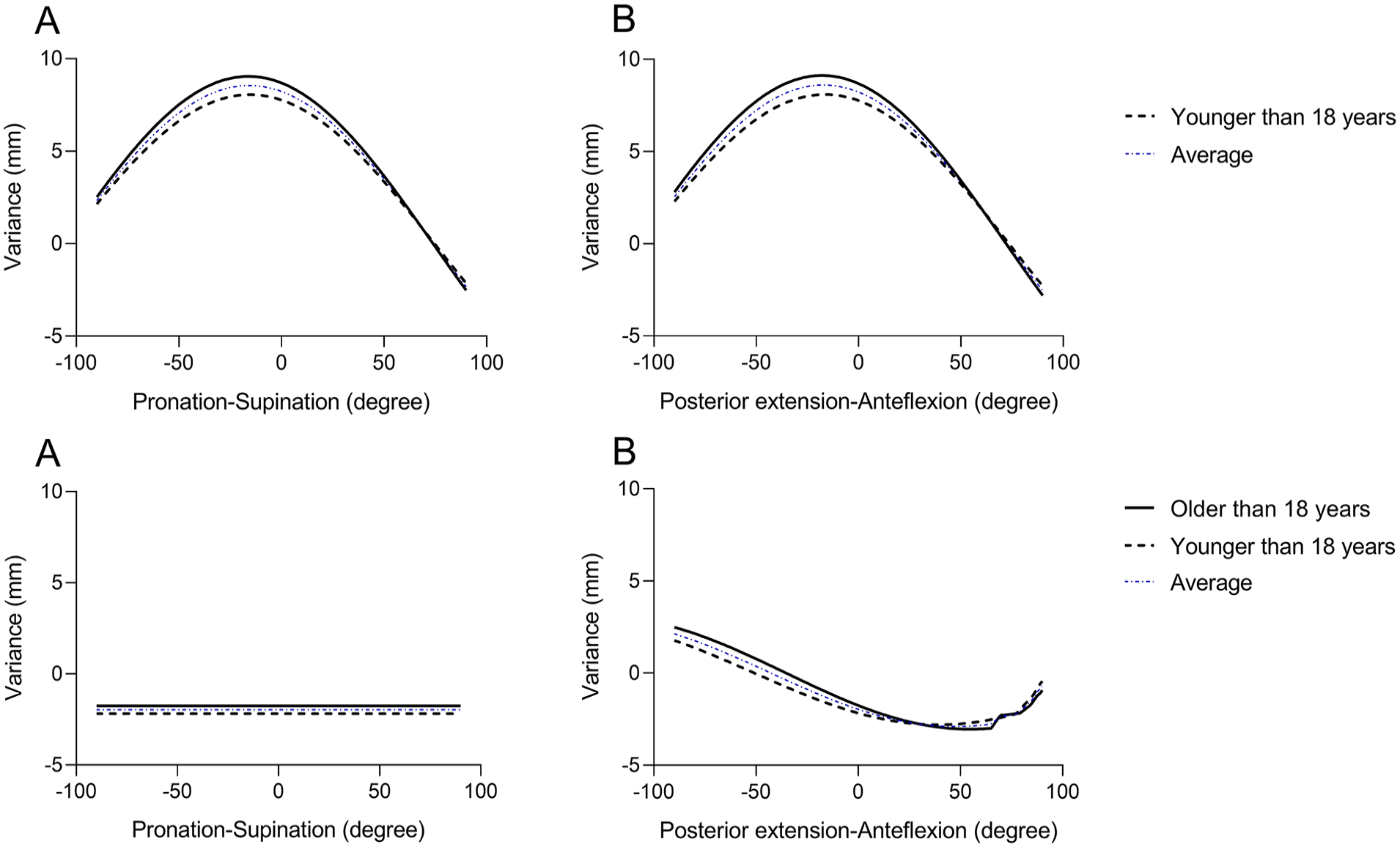
When the head performed pronation and supination. In the supine position, (A) the OHP was achieved at a pronation of 15°, with the DET-RW of 8.05 ± 1.69 mm in the children group and at a pronation of 16°, with the DET-RW of 9.04 ± 1.87 mm in the adult group. In the standing position, (C) no head position resulted in DET being greater than DRW in both groups. When the head performed anteflexion and posterior extension. In the supine position, (B) the OHP was observed when the head was posterior extension at 17°, with the DET-RW of 8.10 ± 1.47 mm in the children group and at a posterior extension of 18°, with the DET-RW of 9.13 ± 1.53 mm in the adult group. In the standing position, (D) When the head performed anteflexion and posterior extension, the DET exceeded DRW when the head underwent posterior extension beyond 51° in the children group and posterior extension beyond 36° in the adult group, with the OHP observed at a full posterior extension of 90°, yielding the DET-RW of 1.77 ± 1.38 mm in the children group and 2.48 ± 1.57 mm in the adult group.
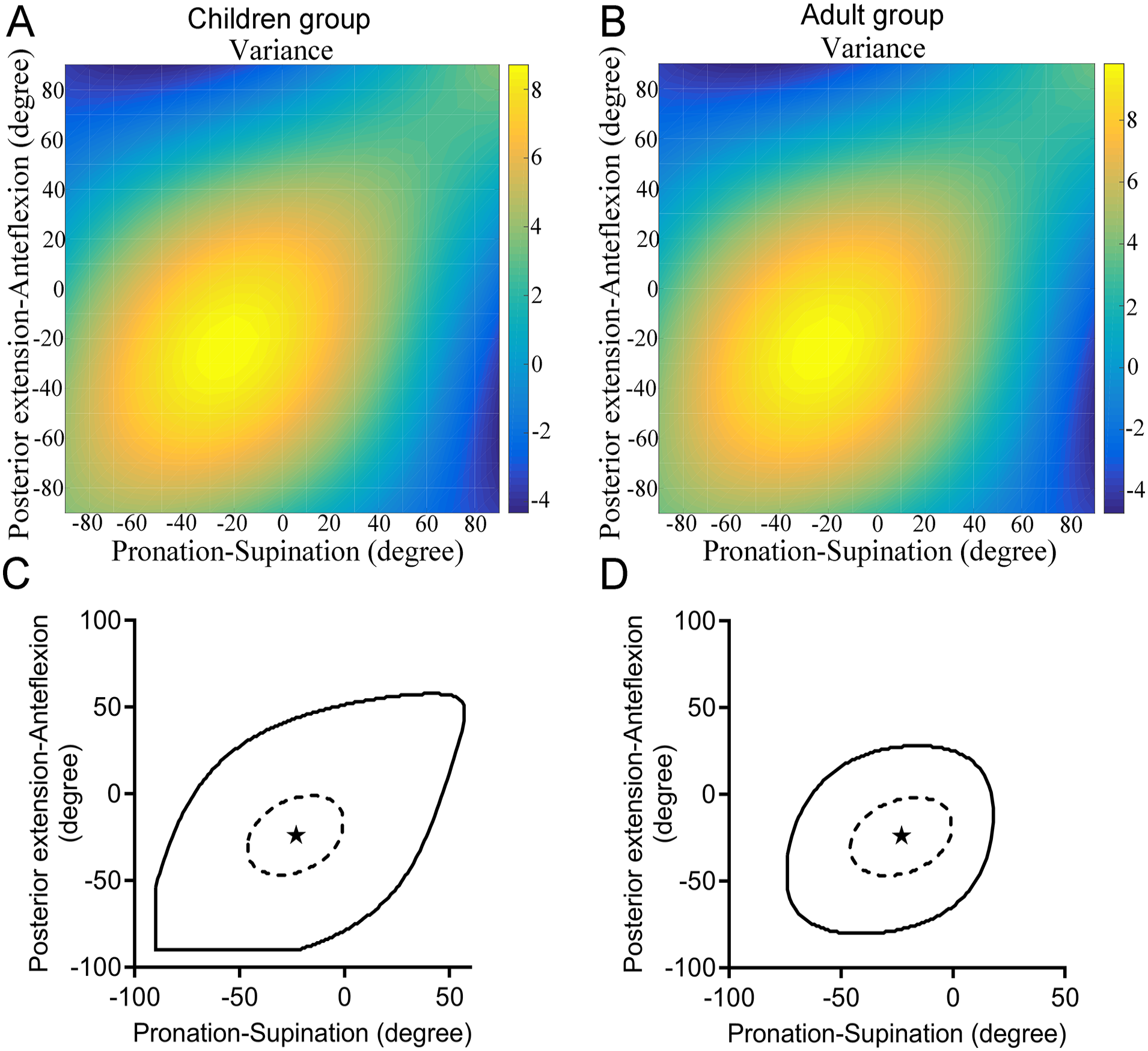
In the supine position. The DET-RW was changed with head movement in the children group (A) and in the adult group (B). In the solid line range, DET was greater than DRW in the children group (C) and in the adult group (D) (P < .05). Within the range of the dotted line, DET-RW was greater than 8.10 mm in the children group (C) and greater than 9.13 mm in the adult group (D). The OHP was at the asterisk when the head was pronation at 23° and posterior extension at 24° in the supine position. DET-RW = 8.74 ± 1.97 mm in the children group (C) and DET-RW = 9.86 ± 2.24 mm in the adult group (D).
For the comparison of anteflexion and posterior extension with pronation and supination, the OHP was the pronation of 23° and posterior extension of 24°, which corresponded to the DET-RW of 8.74 ± 1.97 mm in the children group and 9.86 ± 2.24 mm in the adult group at supine position (Figure 7). It was demonstrated from the solid line in Figure 7C and D shown the DET was greater than DRW significantly. The dotted line in Figure 7C and D represents DET-RW exceeded 8.74 mm in the children group (Figure 7C) and 9.86 mm in the adult group (Figure 7D).
Discussion
Local steroid application to the inner ear has been established as an essential intervention for certain otologic conditions.1,2 Whereas, with the head moving, it cannot achieve the therapeutic drug concentrations in the inner ear, 10 cause the rapid clearance of the medication from the middle ear could significantly influence the bioavailability of the steroids in the cochlea. Ungar et al used virtual and in vitro models of intratympanic anatomy to identify OHP for drug delivery. 8 Thus, head position is a controlled factor that can be optimized with relative ease compared to physiological and pharmacological variables. Large amounts of studies generally focused on the pharmacological aspects of the steroids used, 7 while the physical retention of these drugs within the inner ear, specifically, has not been extensively studied. In Ungar’s study, virtual model was used for a series of specific measurements, 53° vertical axis rotation away from the injected ear, 27° longitudinal axis rotation toward the non-injected ear, and 10° neck extension in the transverse axis were performed. 8 This finding was comparable with our study. While Ungar et al. focused on a singular anatomical model, our study accounts for a broader range of anatomical diversity, providing a more comprehensive understanding of the impact of head positioning.
Our study investigated potential disparities between children and adults as well. Regardless of the chosen position (supine or standing), and the head movements (pronation, supination, anteflexion, and posterior extension) executed, the trends of the DET-RW were consistent across the two groups (Figures 6 and 7). Hong et al demonstrated that the bony part of ET slightly changes with its relative position with age. 9 The angle of ET was observed to constantly increase with age, and the values were found to be within the range of the adult size in children older than 7.7 years. As well as the angle, the length of ET was observed to constantly increase with age, and the values were found to be within the range of the adult size in children older than 7.7 years. 11 Since there were only two subjects younger than 8 years old in this study, age seemed to have a negligible effect on the optimal position for intratympanic injection. This discrepancy could be attributed to the individual anatomical variations among patients, which were accounted for in this study’s methodology. It was also possible that previous studies may have overlooked or underestimated the significance of these particular angles due to a focus on a single anatomical model or a lack of multi-dimensional imaging analysis. The practical applications of these findings are significant.
Steroids access the cochlea via the RW membrane. According to diffusion principles, the amount of diffused substance correlates directly with diffusion duration before reaching a steady state, underscoring the importance of retaining the injected steroids within the RW. This highlights the necessity to maintain the injected steroids within the RW. Three major mechanisms control the final amount of therapeutic drug that will be in contact with the RW membrane: loss in the ET, loss in the mastoidal air cells, and transmucosal loss. 12 The OHP identified through this study could be recommended post-intratympanic injection to reduce steroid loss in the ET and maximize the duration of the drug’s presence within the middle ear, potentially enhancing therapeutic outcomes. In clinical settings, incorporating these head positions into post-injection care protocols could be an effective, non-invasive strategy to improve the efficacy of intratympanic injection steroid treatments. It is important to emphasize that while the OHP is beneficial, it may not be necessary or practical for all patients. For example, patients with specific anatomical variations or those who have difficulty maintaining the position due to physical limitations may require tailored recommendations.
Additionally, this study suggested that the OHP was not a “one-size-fits-all” situation; instead, personalized adjustments based on individual anatomical landmarks could provide the best outcomes. The findings from this investigation highlighted the intricate relationship between head positioning and the diffusion of steroids within the ear. A pronounced variation in the relative positions of the ET and RW with different head movements, particularly in the supine position, underscored the necessity of a head position protocol post-intratympanic injection. However, this study overlooked aspects such as the properties of middle ear fluid, the characteristics of the round window niche, and the physiological impacts of swallowing on middle ear fluid, necessitating further investigation via finite element analysis.
To sum it up, the observed head positions conducive to maximizing steroid retention within the middle ear offer a promising adjunct to the current intratympanic injection steroid administration protocols. The non-uniformity in anatomical structures among individuals suggested that a degree of personalization in post-injection care could be beneficial. Further research involving larger, more diverse populations and clinical trials was warranted to validate these findings and develop standardized guidelines that could be easily implemented in otologic practice.
Footnotes
Availability of Data and Materials
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Natural Science Foundation of China (No. 82301306 and 82101216) and the Shanghai Committee of Science and Technology, China (No. 23Y11909700).
Ethics Approval
The study received ethical approval from the Ethics Committee of the Eye & ENT Hospital of Fudan University (No. 2020118).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.