
Abstract

Significance Statement
The presence of a branchial cleft cyst in the nasopharynx with petrous apex involvement and high T1 signal on magnetic resonance imaging can mimic a cholesterol granuloma and could be considered ectopic given the atypical location for a branchial cleft cyst.
Report
A 51-year-old male patient presented with a history of right-sided serous otitis. Computed tomography scan revealed an expansile lesion involving the right petrous apex with bony remodeling and fluid in the mastoid air cells (Figure 1).

Axial (A) and coronal (B) CT images of the head in bone windows without contrast demonstrate an expansile lesion involving the right petrous apex (red arrows) with bony remodeling and fluid in the right mastoid air cells (green arrow). CT, computed tomography.
Magnetic resonance imaging (MRI) demonstrated a T1 and T2 hyperintense cystic lesion involving the right petrous apex with no post-contrast enhancement. Right tympanomastoid fluid infiltration was also present (Figure 2).
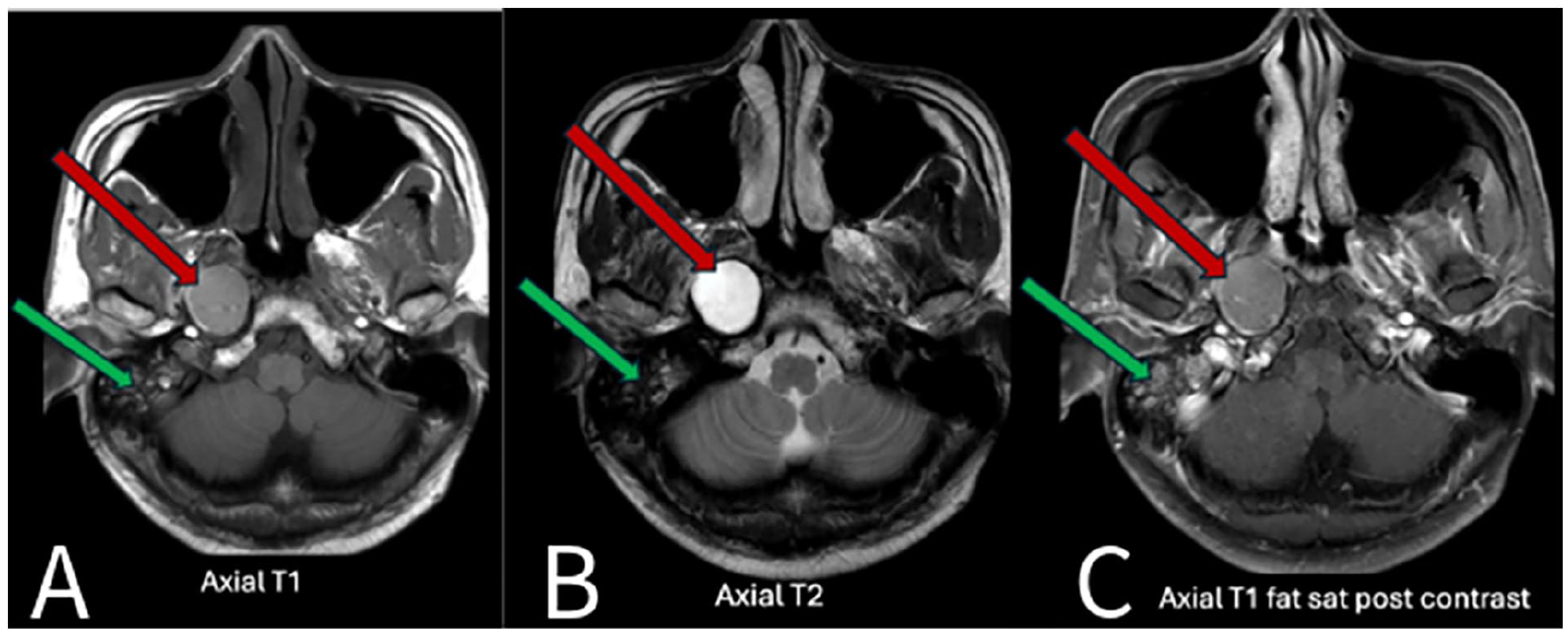
Axial T1-weighted (A), T2-weighted (B), and post-contrast T1-weighted fat-suppressed (C) MR images of the head demonstrate a hyperintense expansile cystic lesion involving the right petrous apex (red arrows). There is right tympanomastoid fluid (green arrows). MR, magnetic resonance.
The patient underwent a biopsy via the transnasal approach and initial pathology suggested an inflammatory lesion. The lesion was then excised with a combined approach by ENT and neurosurgery. Marsupialization of the cyst cavity was performed with removal of crystalloid debris and motor oil consistency fluid. Near total resection of the cyst wall was completed and a Propel mini stent was placed. Pathology showed cyst contents with scant refractile debris. The excised cyst wall showed respiratory mucosa and chronic inflammation consistent with a nasopharyngeal branchial cleft cyst.
The branchial apparatus consists of 6 arches with associated clefts and pouches. These structures eventually give rise to many structures of the head and neck in the developing fetus. However, congenital anomalies may occur, which may manifest as a cyst, sinus tract, or fistula. These defects are present at birth but are often asymptomatic and go unnoticed for years. During respiratory tract infections, they may become inflamed and symptomatic. The most common origin of cleft cysts is the second branchial cleft and are commonly located at the anterior border of the sternocleidomastoid muscle with possible sinus tracts to the skin or the tonsillar fossa of the pharynx. 1 However, they may very rarely involve the nasopharynx, posing a challenge since imaging findings may initially cause concern for other lesions typical for that location. This article reviews the clinicoradiologic features of a branchial cleft cyst in an atypical location with involvement of the temporal bone.
Branchial cleft cysts can rarely involve the nasopharynx and can become symptomatic in a respiratory tract infection. 2 However, this case is particularly atypical in that there was remodeling of the petrous apex of the temporal bone, which mimicked a cholesterol granuloma, particularly with the high T1 signal on MRI. The location of the lesion is atypical for first or second branchial cleft cysts and thus could be considered to be ectopic. Nevertheless, the lesion displayed benign features on imaging, but treatment was warranted due to associated symptoms of otomastoiditis related to Eustachian tube obstruction. The main treatment for such lesions consists of excision and marsupialization, which can relieve symptoms. A steroid-eluting stent can be used to maintain the patency of the marsupialized cyst, reducing the amount of postoperative care. 3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.