
Abstract

Significance Statement
Ectopic thyroid tissue is a rare condition resulting from impaired embryological migration of the thyroid gland. Lingual thyroid tissue is most commonly seen. Triple ectopic tissue is very rare. Ectopic thyroid may be the only functional tissue in the absence of normal thyroid tissue. In these cases, imaging and diagnosis is important to prevent removal of functional thyroid tissue.
A 35-year-old woman was admitted to our clinic with complaints of midline swelling in the anterior aspect of the neck and dyspnea and dysphagia, which had increased over the previous year. The patient had no known chronic disease or trauma and was diagnosed with bicornuate uterus. On physical examination, a hard, painless, mobile mass with tongue protrusion in the midline at the level of the thyroid cartilage was observed. In addition, a circumscribed rubbery lesion with a diameter of approximately 1.5 cm was observed in the midline at the base of the tongue. There was no normal thyroid gland and no lymphadenopathy on palpation. Thyroid function tests were normal, and no hypo- or hyperthyroidism was detected. On ultrasonography, a 2 cm × 1 cm lesion with heterogeneous echogenicity, located in the midline in the anterior-superior part of the thyroid cartilage and containing internal blood supply, was observed on Doppler imaging. There was no normal thyroid gland. Magnetic resonance imaging (MRI) was performed in the patient who was thought to have thyroglossal duct-ectopic thyroid tissue. The images demonstrated the presence of 3 distinct lesions. The first, measuring 27 mm × 18 mm × 16 mm, was observed to be obstructing the air column posteriorly at the level of the lingual tonsil. The second, measuring 23 mm × 21 mm × 15 mm, was identified at the floor of the mouth. The third, measuring 21 mm × 12 mm × 10 mm, was observed at the midline of the neck. All 3 lesions demonstrated heterogeneous hypointensity on T1-weighted images, iso-hypointense signal with T2-weighted muscle tissue, and contained internal cystic areas (Figure 1). Heterogeneous dense contrast enhancement was observed in postcontrast series (Figure 2). A 3mCi technetium scan demonstrated activity in all the foci observed on MRI. There was no activity uptake in the anatomic distribution of both thyroid lobes. The patient was diagnosed with a thyroid ectopia in lingual, sublingual, and thyroglossal duct regions without normal thyroid tissue in the anatomic thyroid bed. The patient was diagnosed as euthyroid but was recommended for surgery because of dysphagia and dyspnea. However, the patient refused surgery and was followed up.
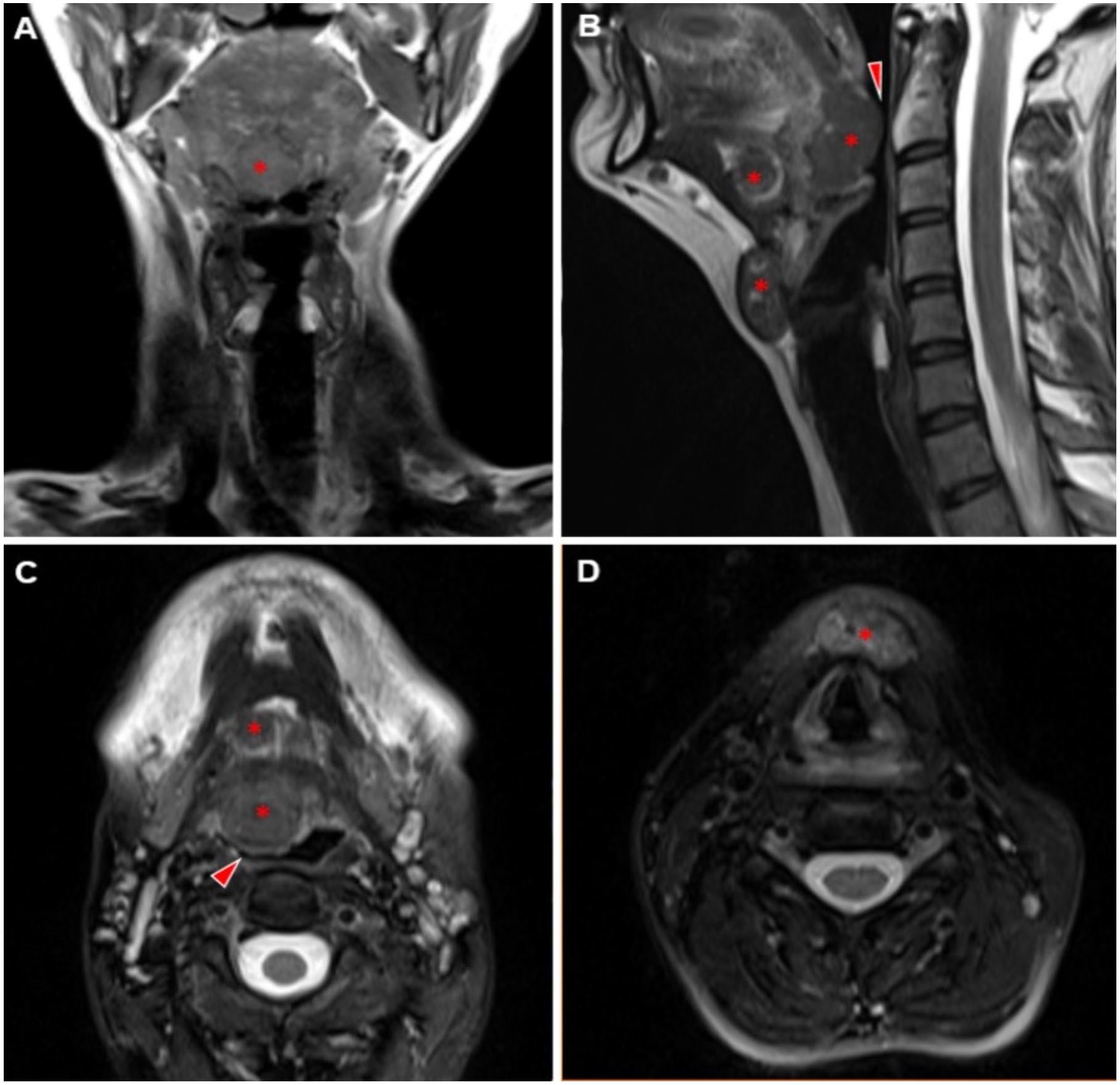
T1-weighted coronal section MR image (A) shows sublingual hypo-isointense ectopic thyroid tissue (asterisk) and normal thyroid tissue is not observed. T2-weighted sagittal (B) and axial sections (C, D) show heterogeneous intensity triple ectopic thyroid tissue (asterisks) and compression of the lingual tissue to the air column (red arrowheads). MR, magnetic resonance.
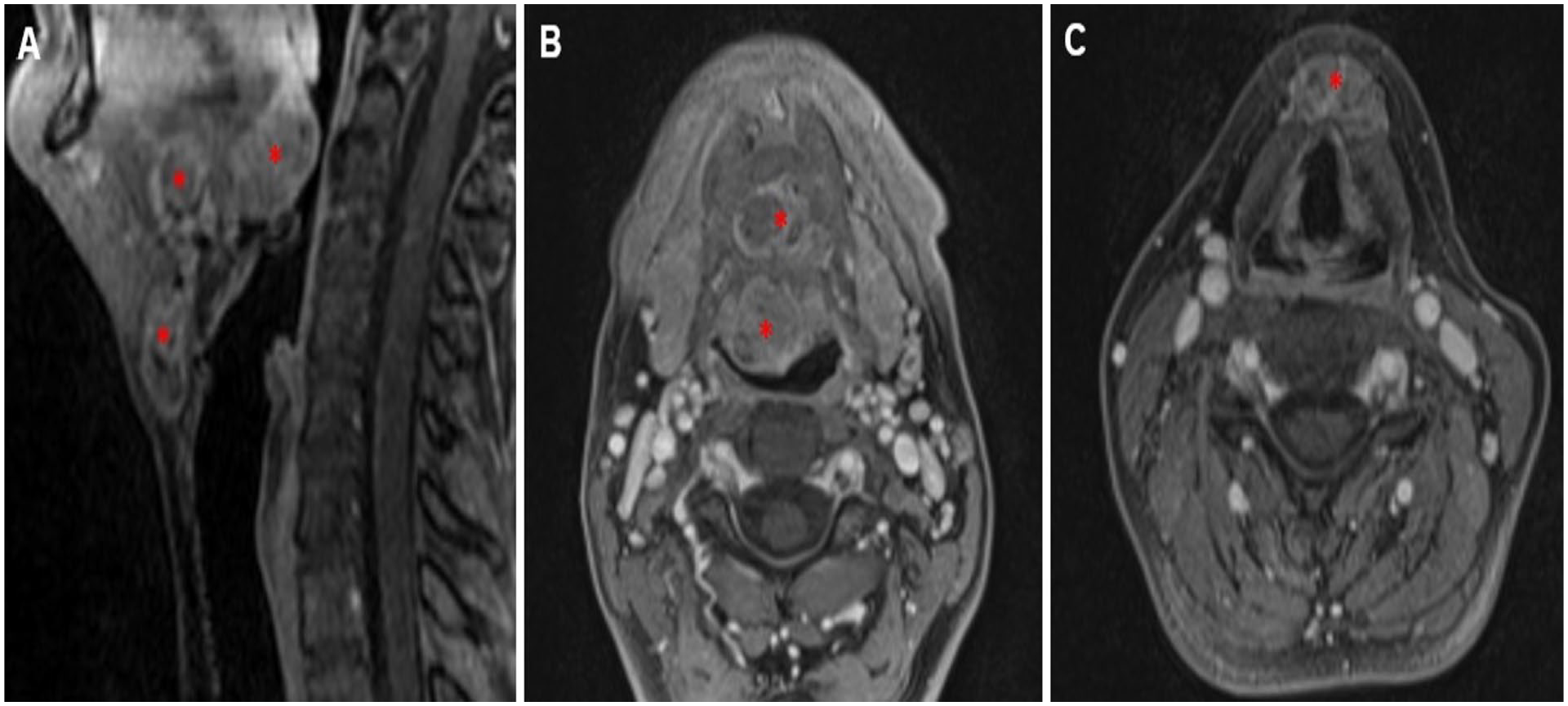
Post-contrast fat-suppressed T1-weighted sagittal (A) and axial (B, C) sections show intense heterogeneous contrast enhancement of ectopic thyroid tissues (asterisks).
Ectopic thyroid is defined as the localization of thyroid tissue other than in the anterior-lateral thyroid cartilages,2-4 which is the normal thyroid region. As a consequence of aberrant embryogenesis, ectopic thyroid tissue can be observed at any point along the descent pathway from the base of the primitive foregut to the paratracheal position. The incidence rate is between 1 in 100,000 and 1 in 300,000, with the most common observed at the base of the tongue. It may present as asymptomatic or may result in dysphagia and dyspnea in the lingual location, while a palpable mass may be observed in the thyroglossal duct location. Ectopic thyroid tissue may be nonfunctioning and may be accompanied by an orthotopic thyroid gland or monofunctioning thyroid tissue.1,2 Triple ectopic thyroid is a very rare phenomenon that has been documented in a limited number of cases in the literature.3,4 Ultrasonography is sufficient to visualize normal thyroid tissue and the thyroglossal duct. Computed tomography (CT) scan and MRI are valuable tools in identifying ectopia, especially when distant from the descending tract of the thyroid. On CT scan, thyroid tissue is hyperdense due to iodine accumulation. On MRI, it is iso-hypointense with muscle on T1-weighted images, variable on T2-weighted images and shows intense contrast uptake in postcontrast series. Technetium imaging is of significant value in demonstrating the localization of activated thyroid tissue. In cases of severe compression symptoms, surgical excision is performed. Hormone replacement therapy can be applied, contingent on the patient’s condition.2-5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.