
Abstract
Introduction
Percutaneous dilatational tracheostomy (PDT) is widely used in ICUs as a simple, fast, and minimally invasive technique that can be completed at the bedside. Notably, however, although overall complication rates are low, severe adverse events, such as posterior tracheal injury, premature decannulation, loss of airway, subcutaneous emphysema, and even death, are still reported.1,2 Therefore, bronchoscope-guided PDT is often used in the clinical setting because it can confirm the positions of the puncture needle, guidewire, and tracheostomy cannula under direct vision and is associated with less trauma and fewer complications.3,4 However, it has some drawbacks such as the requirement of additional staff, making the procedure more cumbersome and taking on an average more time. 5 When withdrawing the endotracheal tube (ETT), the view is unstable because of unsynchronized extubation. In addition, a bronchoscope is mainly used for airway inspection and cleaning of respiratory secretions, which requires a patent negative-pressure suction channel. Therefore, the diameter of the tube is relatively large so bronchoscopy during PDT can cause hypoventilation, hypercapnia, and respiratory acidosis.6,7 To overcome these issues, we have modified a bronchoscope to generate a novel imaging device for PDT under direct vision. We herein introduce the structure of this novel imaging device and report its successful use for guiding PDT.
Case Series
The new device includes a catheter with an external diameter of 4.2 mm, a camera that provides the operative perspective at the end of the catheter, fixation pieces, and electronic components. The catheter is inserted into the endotracheal tube (ETT) and then fixed to it using the fixation pieces; the catheter is also connected to a data cable through the electronic components, with the other end of the data cable being connected to a display. A schematic cross-sectional diagram of the device is shown in Figure 1. Before performing the PDT, the assistant connects the imaging device to the display, inserts the catheter of the imaging device along the ETT to ensure that the distal end of the catheter is flush with the distal end of the ETT, and finally fixes the catheter to the ETT through the fixation pieces. Then the whole procedure was performed under direct vision (Figure 2).
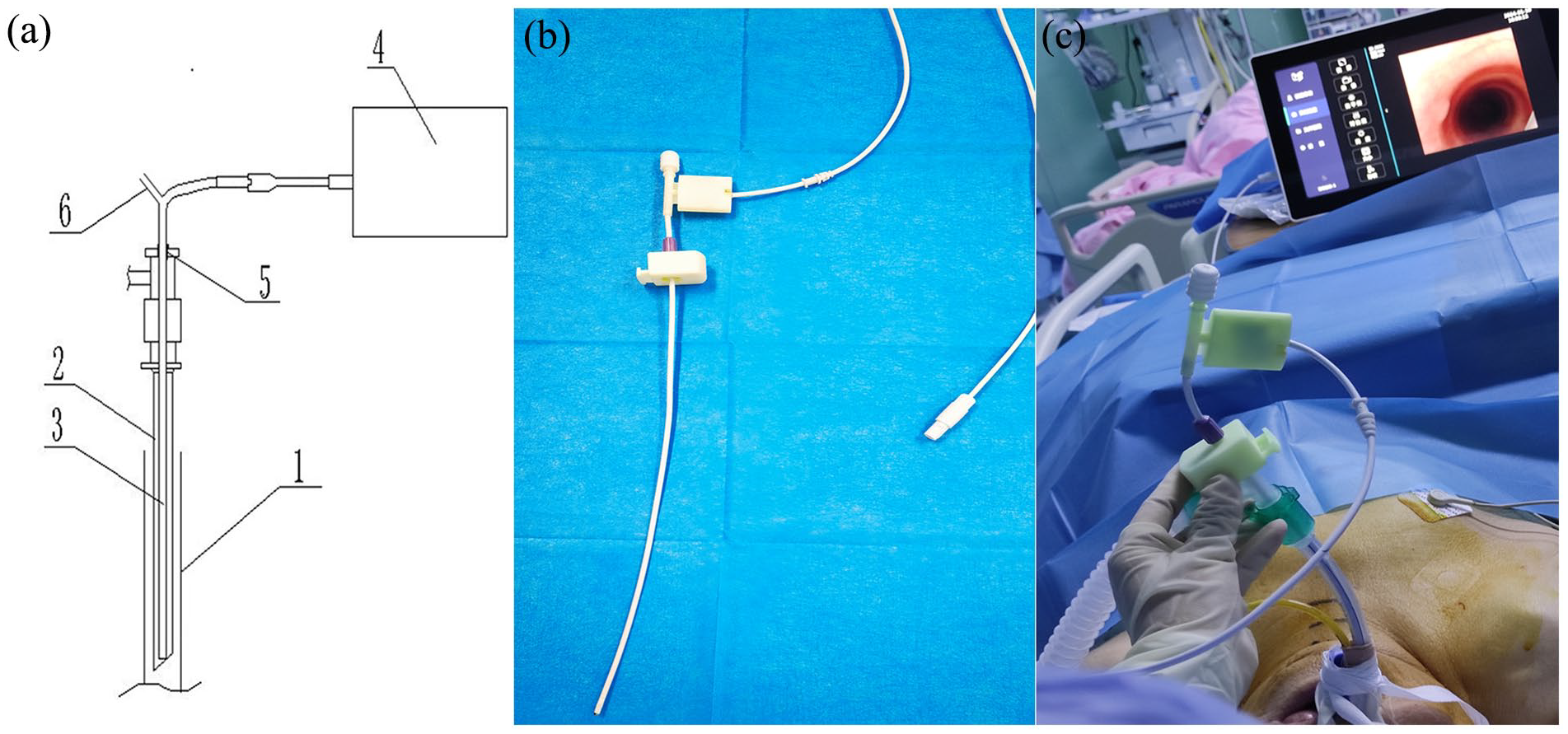
Schematic diagrams and photographs of new imaging device for percutaneous dilatational tracheostomy (PDT). (a) Schematic diagram of the new imaging device. (1) Trachea. (2) Endotracheal tube (ETT). (3) New imaging device. (4) Display. (5) Fixation pieces. (6) Negative-pressure suction channel connector. (b) Photograph of the new imaging device. (c) The new imaging device during PDT. The device is fixed to ETT firmly and no additional operator is required.
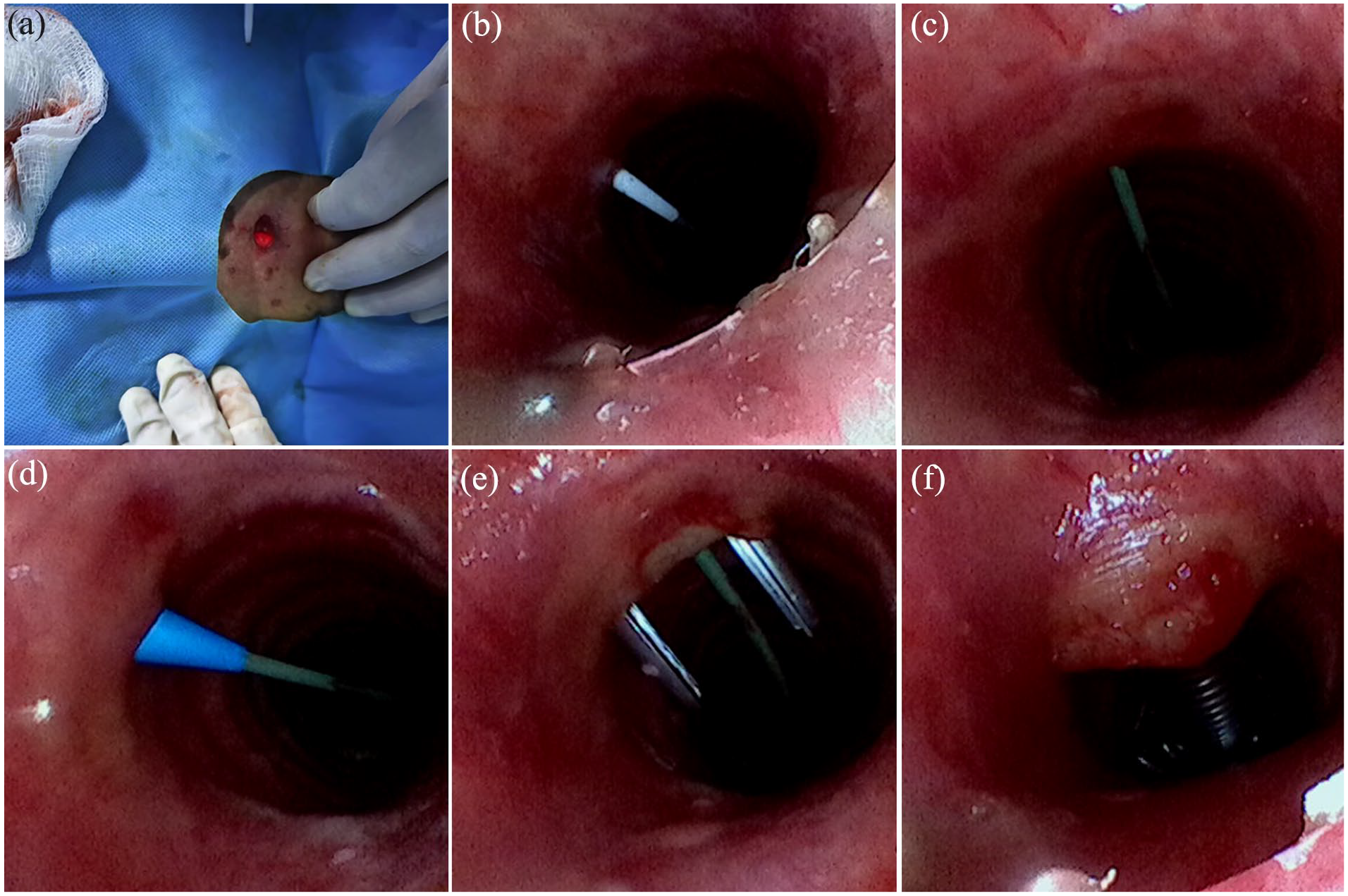
View of the operating field with a new imaging device. (a) Bright light at the puncture site. (b) The puncture needle enters the trachea. (c) Guidewire enters the trachea. (d) The dilator expands the anterior wall of the trachea along the guidewire. (e) Dilator forceps expand the anterior wall of the trachea. (f) The tracheostomy cannula enters the trachea.
We enrolled 9 mechanically ventilated patients who underwent PDT between July 2023 and January 2024. The study was approved by the ethics committee of Shandong Public Health Clinical Center (approval number: GWLCZXEC2023-57-1). Before the procedures, written informed consent was obtained from the patient’s family members. Gender distribution was 67% male and 33% female, with a mean Acute Physiologic Assessment and Chronic Health Evaluation II (APACHE II) score of 22.22 ± 5.54. Tracheostomy was performed for the following medical conditions: cerebrovascular disease (n = 5), severe pneumonia (n = 1), motor neuron disease (n = 1), meningitis (n = 1), and thoracic spinal tuberculosis (n = 1). The average pre-tracheostomy tracheal intubation time was 10.78 ± 5.02 days. Three medical staff were involved in the procedure: an operator, an assistant, and a nurse. Puncture was successful after a single attempt in all patients and no ETT cuffs ruptured. The procedure did not result in major bleeding, pneumothorax, mediastinal emphysema, accidental extubation, desaturation, hypercarbia, respiratory acidosis, hemodynamic abnormality, or posterior tracheal puncture. The average time was 11.63 ± 1.56 minutes from skin incision to needle insertion and 4.43 ± 1.99 minutes from needle insertion to tracheal placement (Table 1).
Characteristics of the Cases.
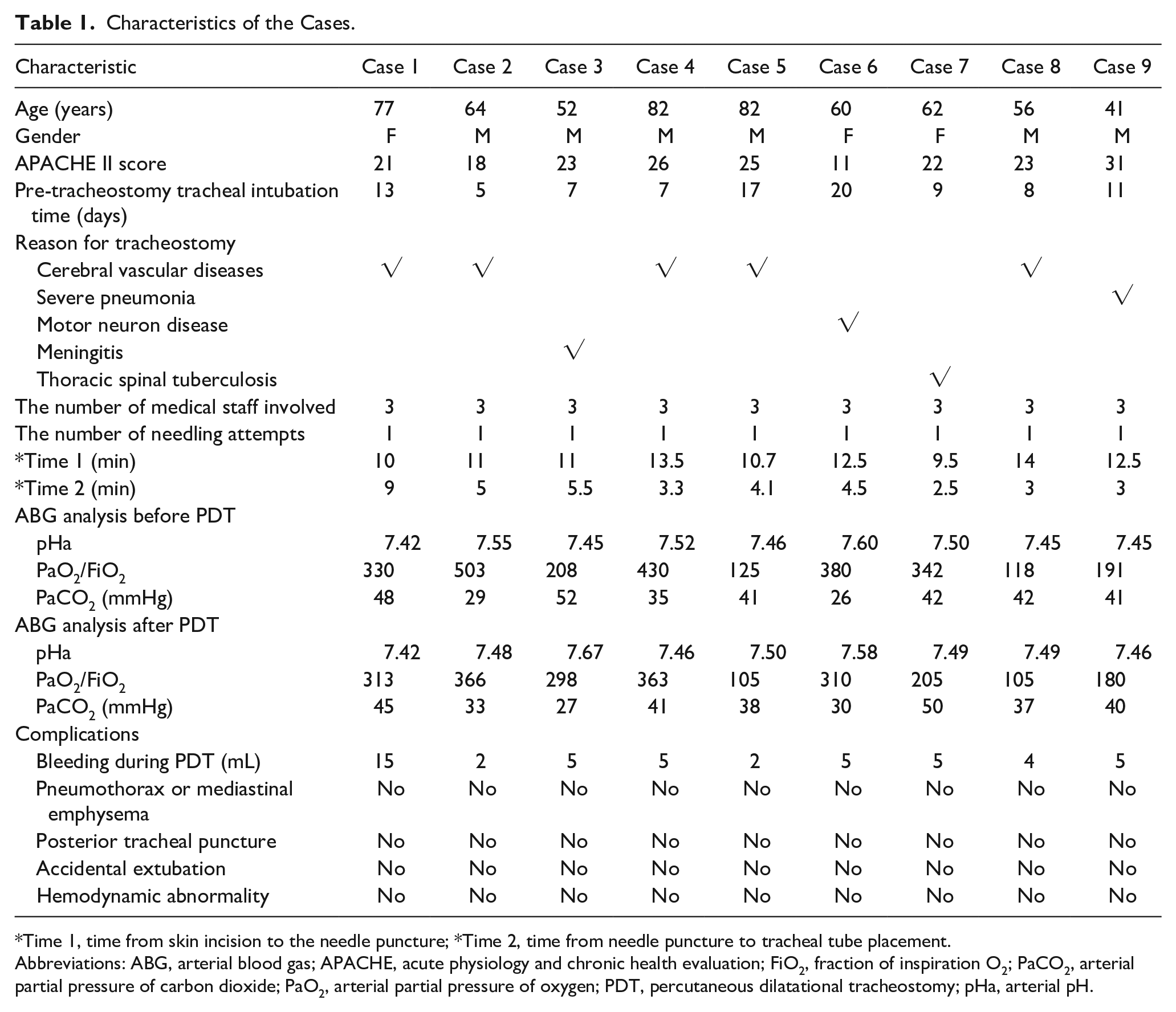
Time 1, time from skin incision to the needle puncture; *Time 2, time from needle puncture to tracheal tube placement.
Abbreviations: ABG, arterial blood gas; APACHE, acute physiology and chronic health evaluation; FiO2, fraction of inspiration O2; PaCO2, arterial partial pressure of carbon dioxide; PaO2, arterial partial pressure of oxygen; PDT, percutaneous dilatational tracheostomy; pHa, arterial pH.
Discussion
PDT has since been frequently employed for critically ill patients in ICUs because of its ease of application and brief procedural time. 8 However, because the puncture needle is inserted blindly, puncture can result in complications such as posterior tracheal wall injury, bleeding, pneumothorax, and mediastinal emphysema.9,10 Evidence suggests that bronchoscopy guidance can dramatically reduce complications in association with the following 3 advantages.11-13 First, most patients undergoing PDT have an ETT in place, and the ETT needs to be moved back to a proper position during the procedure. Excessive withdrawal may cause the ETT to move outside the vocal folds and thus affect ventilation, whereas insufficient withdrawal allows the puncture needle to pierce the ETT. Bronchoscopy facilitates direct visualization of the anterior tracheal wall approaching the posterior wall and the narrowing of the tracheal lumen when the operator presses on the trachea, and a bright light can be seen at the site of skin puncture; both of these signs can assist in confirming the position of the tip of the ETT. The second advantage is that bronchoscopy guidance allows the operator to directly observe whether the puncture needle, guidewire, dilator, dilator forceps, and tracheal cannula are properly placed into the trachea, which helps to reduce complications such as injury to the posterior wall of the trachea, mediastinal emphysema, and pneumothorax. Third, the airway can be observed during the procedure, allowing blood or secretions inside the airway to be cleared in a timely manner.
Despite these strengths, bronchoscopy guidance has some obvious shortcomings that limit its clinical application. First, an additional operator is required to operate the bronchoscope, which takes up human resources and operating space. 14 In fact, human resource shortages are common in ICUs, and the space for the procedure is limited because of the use of monitoring equipment and advanced life-support devices at the bedside. As a result, many ICU doctors choose not to use a bronchoscope when performing PDT. Second, the operator and the bronchoscope operator need to closely cooperate with each other when withdrawing the ETT. Unsynchronized extubation may affect the view and even irritate the airway wall, leading to choking and coughing, which can interfere with the operation. 14 Third, the cumbersome operation and the requirement for mutual cooperation lead to a longer duration of the procedure. Fourth, it has been reported that the application of bronchoscopy can lead to complications such as acidosis and carbon dioxide retention and affect intracranial pressure.6,7
In view of the above shortcomings of bronchoscope-guided PDT, we modified the bronchoscope and created a novel imaging device for PDT. To accomplish this, we removed the handle of the bronchoscope and added fixation pieces to secure the catheter to the ETT. Compared with bronchoscopy, our new technique allows the performance of the operation under direct vision with acceptable safety. The device is equipped with a negative-pressure suctioning channel to remove airway secretions. It also has the following 4 notable advantages. First, the catheter of the device can be fixed to the ETT before the operation. Therefore, no additional operator is required during the procedure, which saves both human resources and operating space. Second, the catheter is withdrawn synchronously with the ETT, eliminating the need for cooperation between 2 operators and ensuring the stability of the view without irritating the airway. This enables the operation to be carried out more smoothly. Third, a bronchoscope is mainly used for airway inspection and cleaning of respiratory secretions, which requires a patent negative-pressure suction channel. Therefore, the diameter of the tube is relatively large. By contrast, our new imaging device is designed to guide the tracheostomy procedure, and its main function is to use a video system to guide the operation rather than to remove secretions. Therefore, the outer diameter of the device is smaller. Accordingly, its impacts on ventilation and arterial blood gas are also smaller. Fourth, patients should not be ventilated via an endotracheal tube for longer than 3 weeks unless they are either unstable or unlikely to benefit from tracheostomy.15,16 However, the blind nature of conventional PDT and the complexity of bronchoscope-guided PDT may lead to hesitancy in performing the tracheostomy, causing the operator to miss the optimal treatment window. Our novel imaging technique offers a simple and easy option for PDT that may encourage the timely implementation of tracheostomy and thus benefit more patients. As shown in our study, the procedure guided by the novel device required only 3 medical staff and was easy to perform. All punctures were successful after a single attempt, and no complications such as mediastinal emphysema, pneumothorax, accidental extubation, or injury to the posterior wall of the trachea occurred. All operators who utilized the novel technique offered positive feedback on the device.
However, this new technique has 3 main limitations. First, endoscopy guidance should be used together with ultrasonography to improve safety for percutaneous. Current data suggest that only endoscopy guidance does not seem to be effective enough to prevent complications related to local alterations of anatomical structures of the neck. 17 Preoperative ultrasound is essential to assess the at-risk structure of the neck to reduce the risk of bleeding. Second, it may also lead to hypoventilation, hypoxia, and hypercapnia. The third limitation is that the device must be inserted into the ETT and is therefore only suitable for patients receiving PDT under endotracheal intubation.
In conclusion, our new imaging device is appropriate for patients undergoing tracheostomy with endotracheal intubation. In addition to the benefits of bronchoscope-guided PDT (i.e., video assistance, safety, and fewer complications), it also has other advantages such as the requirement for fewer personnel, being easier to operate, keeping the view more stable, and smaller impact on ventilation and arterial blood gas. These benefits may facilitate the adoption of early tracheostomy and therefore benefit more patients. Our new imaging device has the potential to be an ideal PDT technique, and this potential requires further exploration.
Footnotes
Acknowledgements
We express the greatest appreciation to the ICU members who are as follows: Xiaoyi Yu, Ran Zhang, Hongbo Liu, and Lili Ju for their support in recording data. We also thank Jialiang Gao for help with device modification and technique support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of Shandong Public Health Clinical Center (approval number: GWLCZXEC2023-57-1). Before the procedures, written informed consent was obtained from the patient’s family members.