
Abstract
Keywords
Introduction
It is unusual for an adult patient to require the orthognathic surgeon to take into account the possibility of future jaw growth. Specific orthodontic techniques, such as fast palatal expansion, which are beneficial in children, are limited in adults. Both the surgeon and the orthodontist need to be familiar with alternative treatments. An adult patient’s social, economic, and psychological needs differ from a child’s needs. These may require switching the usual treatment order (orthodontics first, surgery later) on its head. Instead, it may be possible to address the bone issues via surgery and proceed with any additional orthodontics that may be required or wanted. Most patients with jaw abnormalities and malrelations also exhibit various Myofascial pain dysfunction (MPD) symptoms. 1
When patients have abnormalities in their dentofacial skeleton, orthognathic surgery can be used to realign the facial bones and improve their function.2-4
Careful investigation of the soft tissue via clinical examination and supporting pictures, evaluation of the skeleton via standardized radiographs, and evaluation of the dental via study dental casts are all necessary to successfully correct maxillofacial abnormalities. Therefore, the surgeon, the dentist, the orthodontist, and sometimes the restorative prosthodontist must collaborate to formulate a treatment plan. In contrast to the outcomes of many other surgical procedures, the success of this one depends on a wide range of factors that manifest long before surgery and continue to be under control for some time following. 2
Insurance companies may have differing opinions on whether or not they will cover orthognathic surgery to correct jaw discrepancy and malocclusion. The “medical necessity” concept is notoriously murky and hard to prove in court. The combined expense of orthodontic and orthognathic treatment can be too much for some individuals to pay out of pocket. When formulating their recommendations for patient care, treating providers should consider this consideration. 5
Most patients will seek surgical examination at their treating orthodontist’s suggestion. The patient may present to the surgeon with a predetermined treatment goal due to the orthodontist’s area of expertise. Orthodontic camouflage tactics to achieve a specific occlusal relationship should be encouraged, considering skeletal disparity, face aesthetics, and the degree of dental compensation. This is especially true for patients with a premium on face beauty. 5
In this article, we reviewed safer orthognathic surgery and preventive measures.
Methods
The literature survey was performed in PubMed, EBSCO, UpToDate, ProQuest Central databases of Kırıkkale University, and Google and Google Scholar databases. The search was conducted using the terms “orthognathic surgery” or “Le Fort I-type osteotomy” or “Le Fort II-type osteotomy” or “Le Fort III-type osteotomy” or “preventive measures” or “safety” or “indications” or “contraindications” or “support” from 1990 to 2024. Review articles, randomized controlled trials, prospective studies, and retrospective research are all part of the data set pulled in by the search.
Orthognathic Surgery
Standard orthognathic operations to repair jaw deformity and adjuvant procedures to improve hard and soft tissue shapes make up modern orthognathic surgical treatment for dentofacial deformity. These supplementary operations include a suction lipectomy of the neck, a septorhinoplasty, and an osseous or alloplastic genioplasty. 5
The orthodontist and maxillofacial surgeon must collaborate to create a thorough treatment plan with reliable results. 5
Orthognathic surgery can involve either the maxilla, the mandible, or both. Improving the dynamics of nasal airflow may necessitate simultaneous intranasal surgery consisting of septoplasty and reduction of the inferior turbinate. In some instances, genioplasty and neck liposuction may also be recommended to enhance the final appearance. 5
Etiology
When the upper facial skeleton develops at a different rate than the lower one, the usual link between the upper and lower jaws is disrupted, leading to a dentofacial skeletal anomaly. Inherited and environmental factors can affect the facial skeleton’s typical development. Regular development and growth are disrupted by congenital disabilities such as facial clefts and syndromic diseases like Apert and Crouzon syndromes. 2
If the typical skeletal elements are displaced after a traumatic incident in an adult, osteotomies may be necessary to realign them. Facial fractures and disfigurement are specific results of trauma to the growing face. Neoplastic growth, surgical resection, and iatrogenic radiation are potential causes of significant dentofacial abnormalities. However, the most prevalent cases needing orthognathic surgery are developmental anomalies representing extremes of population norms. 2
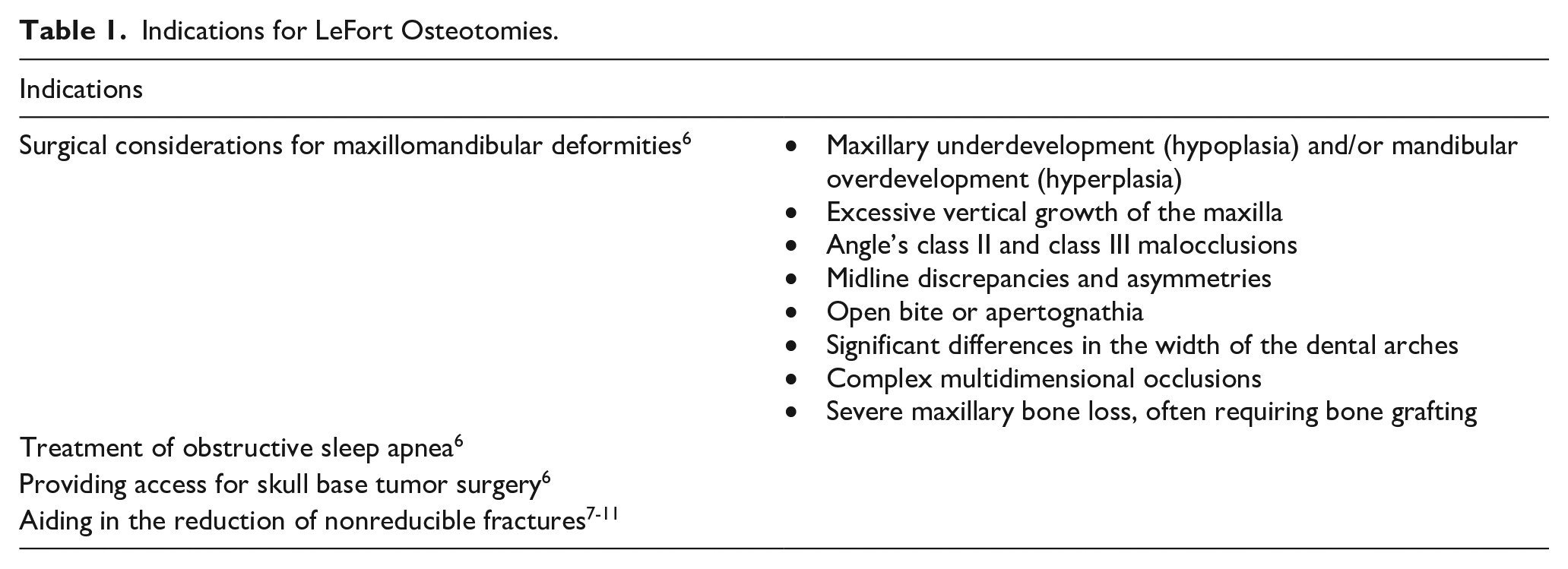
Indications for LeFort Osteotomies
LeFort osteotomy is indicated in the following conditions6-11 (Table 1).
Indications for LeFort Osteotomies.
Contraindications for LeFort Osteotomies
Contraindications for LeFort osteotomies6,12,13 are shown on Table 2.
Contraindications for LeFort Osteotomies.
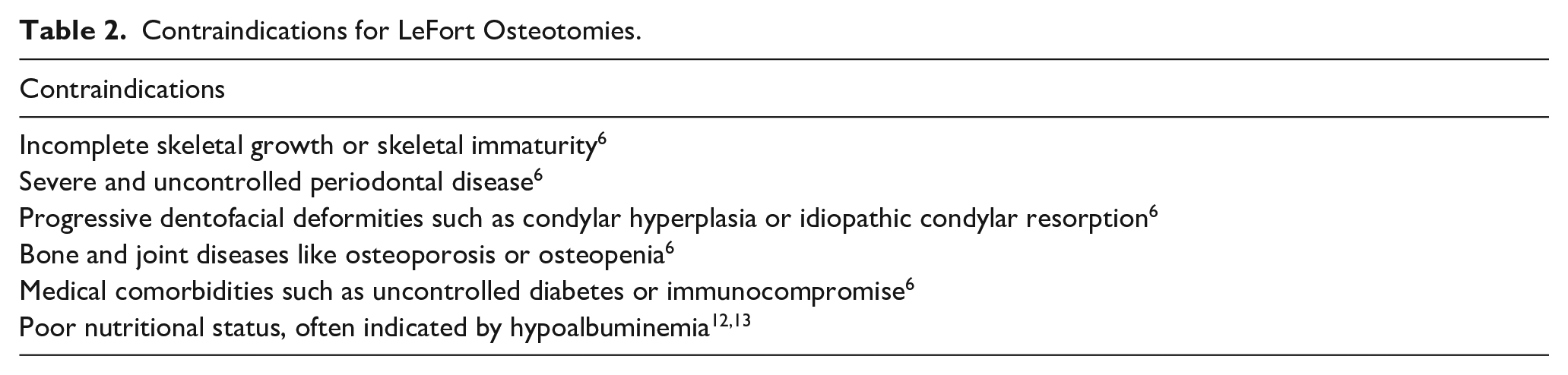
It is important to remember that contraindications are contextual, and there are situations in which they can be an indication to proceed with surgery. As a result, before surgery, the surgeon must do a comprehensive preoperative evaluation and secure informed permission from the patient, parent, or legal guardian explaining the risks, benefits, and probable problems. 6
The Surgical Approach
The elements of the facial skeleton can be “repositioned, redefining the face through a variety of well-established osteotomies, including Le Fort I-type osteotomy, Le Fort II-type osteotomy, Le Fort III-type osteotomy, maxillary segmental osteotomies, sagittal split osteotomy of the mandibular ramus, vertical Ramal osteotomy, inverted L and C osteotomies, mandibular body segmental osteotomies, and mandibular symphysis osteotomies.” 2
Three primary osteotomies are used to treat maxillofacial deformities: “the Le Fort I-type osteotomy in the midface, the sagittal split Ramal osteotomy of the mandible, and the horizontal osteotomy of the chin symphysis.” 2
Midface
The choice of osteotomy for the correction of midfacial abnormalities is condition-specific. The 3 typical lines of weakness in the facial bones give the Le Fort osteotomies their namesake. The Le Fort III osteotomy is a complete craniofacial disjunction that allows the surgeon to lengthen the nose and change the location of the maxilla, nasal root, frontonasal angle, and orbits. Surgeons can adjust naso-maxillary projection with the Le Fort II osteotomy without affecting orbital volume or zygomatic projection. Without affecting the orbito-zygomatic region, the Le Fort I osteotomy enables correction primarily at the occlusal level, including the position of the upper lip, the nasal tip and alar base, and the columella labial angle. 14
Lower Face
Different osteotomies address different mandibular (lower jaw) abnormalities. 15 Most mandibular retrognathism and prognathism occurrences are treated with the sagittal split ramal osteotomy. Some surgeons favor the intraoral vertical osteotomy or the inverted L osteotomy for severe cases of mandibular prognathism. Bone grafts are preferable over inverted L and C osteotomies for mandibular advancement when the mandibular rami are hypoplastic. Chin abnormalities, such as disproportionate chins, can occur without a mandibular malformation or occlusal dysfunction. 2
The horizontal osteotomy of the symphysis (osseous genioplasty) is a far more adaptable operation than alloplastic chin implants, typically used to correct mild sagittal chin deficits. Chin repositioning can cure substantial sagittal and vertical deformities of deficiency (microgenia) or excess (macrogenia), as well as asymmetric situations because the chin can be moved in more than one plane. 2
Preventive Measures in Orthognathic Surgery
Although oral and maxillofacial surgeons and other head and neck surgeons often execute the LeFort I osteotomy, the crucial value of an interdisciplinary team before, during, and after surgery cannot be overstated. For optimal results, multidisciplinary treatment and support must be provided. The orthodontist’s involvement and experience with the surgical treatment plan and the anticipated need for postsurgical orthodontics are crucial in preparing the patient for orthognathic surgery.6,16
Patients with medical comorbidities cannot have a successful operation without preoperative adjustment. The preoperative optimization of a patient’s treatment may need the collaboration of specialists from several fields of medicine. When an anesthesiologist or other anesthesia practitioner is present during surgery, it increases the likelihood of a successful outcome and a speedy recovery after that—planning for potential airway issues posed by maxillo-mandibular fixation and postoperative edema, including discussing the surgeon’s preferred intubation technique, the risks and benefits of hypotensive anesthesia, and the optimal timing of hypotensive anesthesia. Reduced blood loss, improved surgical field visibility, and a shorter hospital stay are all benefits associated with hypotensive anesthesia.17,18
The nursing staff plays a crucial role in the initial postoperative period by educating patients, providing emotional support, and monitoring progress toward main postoperative goals. The pharmacist and pharmacy staff will be critical in selecting the best postoperative drugs for the patient, balancing adequate pain management and safe use. Patients with obstructive sleep apnea or morbid obesity, for example, are at increased risk for over-narcotization or respiratory depression. Therefore, the pharmacist must also develop safe and effective pain control regimes for them. Nutritionists and Registered Dietitians are essential in assessing adequate caloric demands, supporting and enabling a nutritional regimen, and ultimately minimizing postoperative problems and decreasing patient morbidity since proper nutrition is crucial for wound healing.6,19
Pitfalls for Safe Surgery
Soft tissue closure requires a sufficient cuff of gingival tissue, which can only be obtained through meticulous design of the surgical incision. The gum line should always be kept at least 5 mm above the mucogingival junction. Using a #15 blade or electrocautery, a perpendicular incision is created in the mucosa from the first molar to the first molar. The periosteum is scored to allow subperiosteal dissection, and the incision is taken to the bone. Careful dissection of the nasal mucosa surrounding the nasal aperture is then conducted after medial to the piriform rims subperiosteal dissection with a periosteal elevator. If you are having trouble dissecting the nasal mucosa, try using a curved, more accessible elevator or the blunt end of a Woodson elevator. Dissection of the nasal mucosa continues behind the palatine bone. When performing a subperiosteal dissection, locating and protecting the infraorbital nerves is essential as you move upward. The lateral maxillary buttress and the area around it are also dissected. Keeping a subperiosteal plane here is crucial since exposing the buccal fat pad severely limits surgical access elsewhere in the mouth. To finish this stage of the dissection, a curved, more accessible elevator may be helpful. At the pterygomaxillary joint, the lateral dissection stops. While the osteotomy is done on the other side, a ray-tec sponge or neuro-patties can be put in the lateral subperiosteal pocket to facilitate further blunt dissection and aid with hemostasis. 6
After the area of the bone to be cut is exposed, a Bovie electrocautery, a bur, or another tool might be used to make a mark. When done correctly, the osteotomy should begin at the apex of the jaw and end below the inferior turbinate. While finishing the osteotomy, you can preserve the previously dissected nasal mucosa by inserting an instrument like a Sayre elevator or freer on the medial aspect of the nasal aperture. 6
After that, an osteotomy is performed under constant irrigation with a reciprocating saw, straight tapered fissure bur, or bone scalpel, beginning at the lateral maxillary buttress and continuing through the piriform rim. The opposite side has a mirror image osteotomy. Although the initial bone in the buttress is dense, the anterior maxillary sinus wall is fragile once through the buttress, so care must be taken not to apply force to the cutting implement or risk losing control and causing iatrogenic damage to the sinus wall or potentially compromised areas for fixation. The lateral maxillary buttress can be “back cut” once the bilateral osteotomies are finished by placing the cutting instrument again from the medial to lateral side into the osteotomy. The cut at the lateral buttresses can be replicated with small straight osteotomes. 6
Small straight chisels or Neivert-Anderson single-guarded osteotomes are used to finish the lateral nasal osteotomies, with the curved end of the osteotome resting on the floor. It is important to remember that the osteotome needs to be orientated similarly to how the lateral nasal wall diverges from anterior to posterior. When the osteotome hits the pyramidal process of the palatine bone, it will come to a sudden, unyielding halt. A narrow u-shaped osteotome or a double-guarded v-shaped osteotome, with a curved end against the nasal floor, is then used to remove the septum from the maxilla. It is recommended that this osteotomy do not exceed 30 mm in females and 35 mm in males to prevent injury to the descending palatine arteries. 20
At last, an anterior, inferior, and medial big curved osteotome or Tessier cruciform osteotome separates the pterygomaxillary junction. A finger is put intraorally against the pterygoid hamulus to ensure the osteotomy is done correctly. It is wise to inform the anesthesia staff that the maxilla will be downfractured before the pterygomaxillary osteotomy. If a hypotensive anesthetic is preferred, the risk of severe bleeding can be reduced by keeping the mean arterial pressure at around 60. If the osteotome is not positioned correctly, severe bleeding can occur from the maxillary artery and its branches, the descending palatine, and sphenopalatine arteries. For this reason, some writers recommend avoiding using an osteotome at the pterygomaxillary junction and instead separating the maxilla at the tuberosity or by accomplishing downfracture with digital pressure alone. 21
Protecting the Blood Supply
Preserving blood flow to mobilized bone segments, soft tissue, and teeth (dental pulp and periodontal ligament) through maintenance of a connected soft tissue pedicle was first demonstrated by Bell’s groundbreaking work in experimental animal models. 22 More than 4 dentoalveolar segments should not be created in a single arch, and a single tooth should not be placed in a mobilized skeletal segment. The blood supply to the new bone segments created by ramus osteotomies is protected by arteries penetrating the bone from the mandibular elevator muscles. Subperiosteal peeling of the posterior mandible should be kept to a minimum. 5
Protection of Teeth, Bone, and Neurovascular Structures
When working on the jaw, the lingual, inferior alveolar, and face nerves should be shielded from the surgical approach and osteotomy. 5
Osteotomized and mobilized skeletal segments put the teeth in those areas in danger of losing blood supply. There is a heightened danger to teeth near osteotomy sites. Ankylosis of the teeth is avoidable after an interdental osteotomy if the periodontal ligament space is preserved. In cases where an interdental osteotomy will be performed, 3 to 4 mm of bone should be left between the tooth roots during presurgical orthodontic preparation. Transverse osteotomy cuts should be made at least 3 to 5 mm from the root apices to protect the tooth pulp’s blood flow. To reduce the likelihood of postoperative periodontal pocketing and associated bone loss, it is essential to arrange alveolar segments so that components have uniform vertical height. 5
Nutritional Support
Consuming enough protein and calories after surgery is crucial for reversing the catabolic metabolism that occurs due to the stress of surgery. Because the patient’s jaws cannot work correctly for a while, their dietary needs rise simultaneously. Prolonged maxillomandibular fixation after surgery makes matters worse. Goals of 2500 to 3000 calories per day and 1 to 1.5 g protein per kilogram of body weight per day are reasonable. Protein shakes or other nutritionally balanced drinks may be necessary as a supplement. Body weight is commonly used as a guideline to ensure adequate food and drink intake. It may be required to consult with a dietician while hospitalized. It is helpful to have a dedicated caregiver who keeps tabs on the patient’s food and drink consumption. 5
Patient Satisfaction in Orthognathic Surgery
Numerous studies have examined the effects of orthognathic surgery on various aspects of patients’ quality of life, including “psychological, social, physical, functional, and aesthetic factors,” both before and after the procedure.23,24 The “World Health Organization (WHO)” defines quality of life as an individual’s perception of their position in life within the context of their culture and value systems, considering their goals, expectations, standards, and concerns. 25 Although research on the relationship between quality of life and oral surgery has significantly increased, there is still no consensus on the most effective tool for evaluating the outcomes of orthognathic surgery. 26
Health measurement tools, such as the “Short Form Health Survey (SF-36),” evaluate the impact on overall health status beyond the orofacial region. 27 Instruments designed for assessing global oral health, like the “Oral Health Impact Profile’s short form (OHIP-14),” focus on the impact of oral health on quality of life. Some tools are tailored to specific contexts, such as the “Orthognathic Quality of Life Questionnaire (OQLQ),” which is commonly used to assess the impact of orthognathic surgery during the postoperative period. 28
Analyzing the variable “type of facial deformity” is crucial. No significant differences in “OHIP-14” scores were observed based on the type of malocclusion. 29 Nonetheless, Baherimoghaddam et al 30 “(MINORS 18)” identified significant differences in “OHIP-14 scores” between patients with “Class II and Class III malocclusions.” In addition, no significant differences were found in the late perioperative period between patients who underwent the surgery-first approach and those who received conventional treatment.
Conclusion
Orthognathic surgery can involve either the maxilla, the mandible, or both. Improving the dynamics of nasal airflow may necessitate simultaneous intranasal surgery consisting of septoplasty and reduction of the inferior turbinate. In some patients, a genioplasty and neck liposuction may be recommended to enhance the final result. Le Fort I osteotomy, Le Fort II osteotomy, Le Fort III osteotomy, maxillary segmental osteotomies, sagittal split osteotomy of the mandibular ramus, vertical Ramal osteotomy, inverted L and C osteotomies, and mandibular body segmental osteotomies are all examples of well-established osteotomies that can be used to reposition facial skeletal elements and redefine the face. Preventative strategies for risk-free orthognathic surgery include maintaining blood flow, shielding teeth, bone, and neurovascular systems, and bolstering the patient’s diet.
Footnotes
Acknowledgements
None.
Author Contributions
Authors contributed equally to the planning, literature survey, and manuscript writing.
Availability of Data and Materials
All data for this article are presented in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Committee Approval
There is no need for ethics committee approval because this is a review article.
Informed Consent
There is no need to take informed consent because this is a review article.