
Abstract

Significance Statement
Despite their benign nature, the expansive growth of mucoceles can significantly remodel sinus structures and exert mass effects on adjacent anatomical structures. An isolated mucocele in the posterior ethmoid sinus has rarely been reported to cause oculomotor nerve palsy. This case underlines the need for considering mucoceles as an alternate diagnosis, particularly in patients presenting with unexplained neuro-ophthalmic symptoms. Early surgical intervention is efficacious and can offer a favorable outcome with minimal complications.
Rhinoscopic Clinic
A 69-year-old woman presented with sudden onset of diplopia and ptosis of the right eye that had persisted for 3 days; she did not report any medical history of hypertension, diabetes mellitus, or cerebral infarction. She initially visited an ophthalmologist and a neurologist at an outpatient department. Physical examination revealed normal results for muscle power in all 4 limbs, bilateral visual fields, and intraocular pressure. The only symptoms observed were ptosis, restricted motion when gazing to the left (Figure 1A), a decrease in best-corrected visual acuity to 6/12, and a prominent relative afferent pupillary defect in the right eye; therefore, diplopia associated with oculomotor nerve dysfunction was suspected.
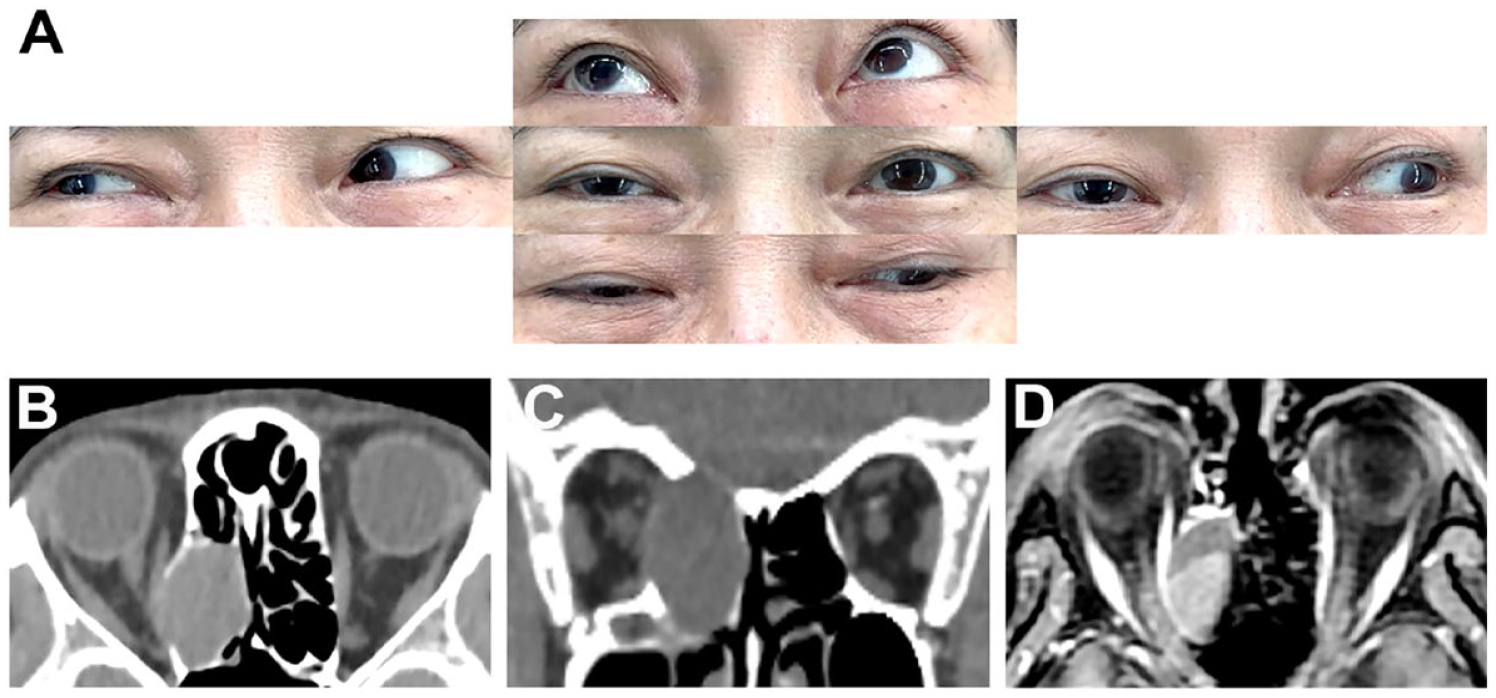
(A) Patient presented with ptosis and limited movement of the right eye during adduction and depression. (B and C) Preoperative axial and coronal view CT scan revealing a soft-tissue nonenhancing lesion over the right posterior ethmoid sinus, accompanied with deviation of the right medial rectus muscle and expansion with remodeling/defect of the bony plate at the cranial base and medial orbital wall. (D) Axial view magnetic resonance imaging scan indicating a cystic mass occupying the right posterior ethmoid sinus. Mild diffusion restriction and some T1-hyperintense area in the posterior half suggest protein-rich content. CT, computed tomography.
She was thus referred to the emergency department for further assessment. Computed tomography (CT; Figure 1B and C) and magnetic resonance imaging scans of her brain (Figure 1D) demonstrated the presence of a posterior ethmoid mucocele. Therefore, we were consulted for managing this likely case of an isolated sinus lesion complicated with ptosis and limited eye movement. Surgery was conducted on her right posterior ethmoid sinus by using a 3-dimensional CT-guided navigation system to achieve decompression. A cystic structure containing milky secretions was discovered (Figure 2A-D), and its pathology was compatible with that of a mucocele. She was subjected to regular postoperative follow-up assessments involving endoscopic examinations, ocular motility assessments, and visual acuity assessments every month. The patient recovered uneventfully, displaying free motion toward the left side of the right eye and a best-corrected visual acuity of 12/12 in the right eye until 6 months after surgery (Figure 3A). Sinoscopy and CT scans of the right paranasal sinuses revealed patent openings without any evidence of residual mucoceles or polyps (Figure 3B-D).
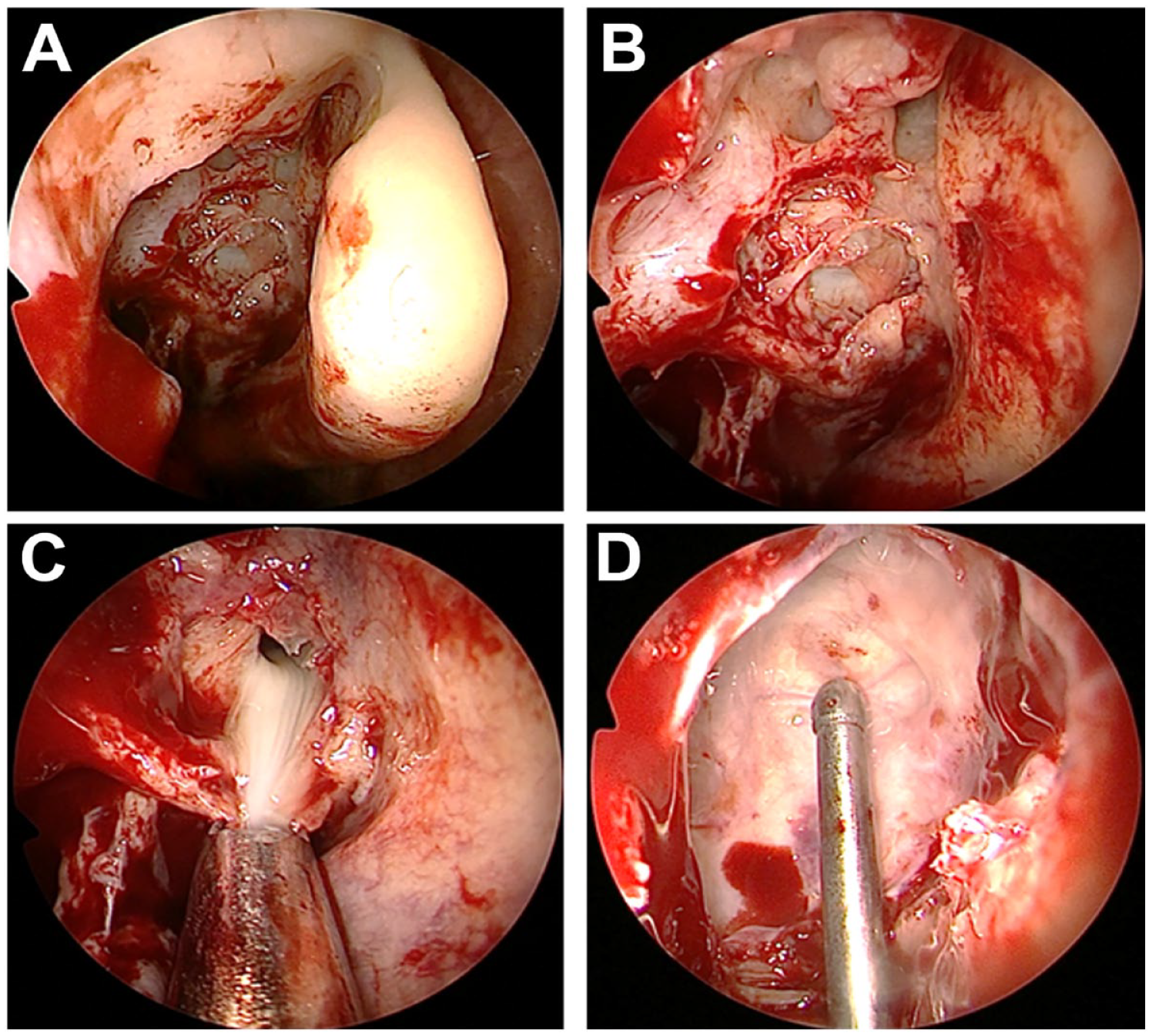
(A and B) Endoscopic operative views showed the approach to the posterior ethmoid sinus after removing the uncinate process and enlarging the ostium of the right maxillary sinus and anterior ethmoid sinus bullae. (C) A cystic structure containing a large amount of mucopus was observed when the mucocele wall was broken down. (D) After removing fragments of bone plates and mucopus, bony defect at the skull base was identified (suction tip).
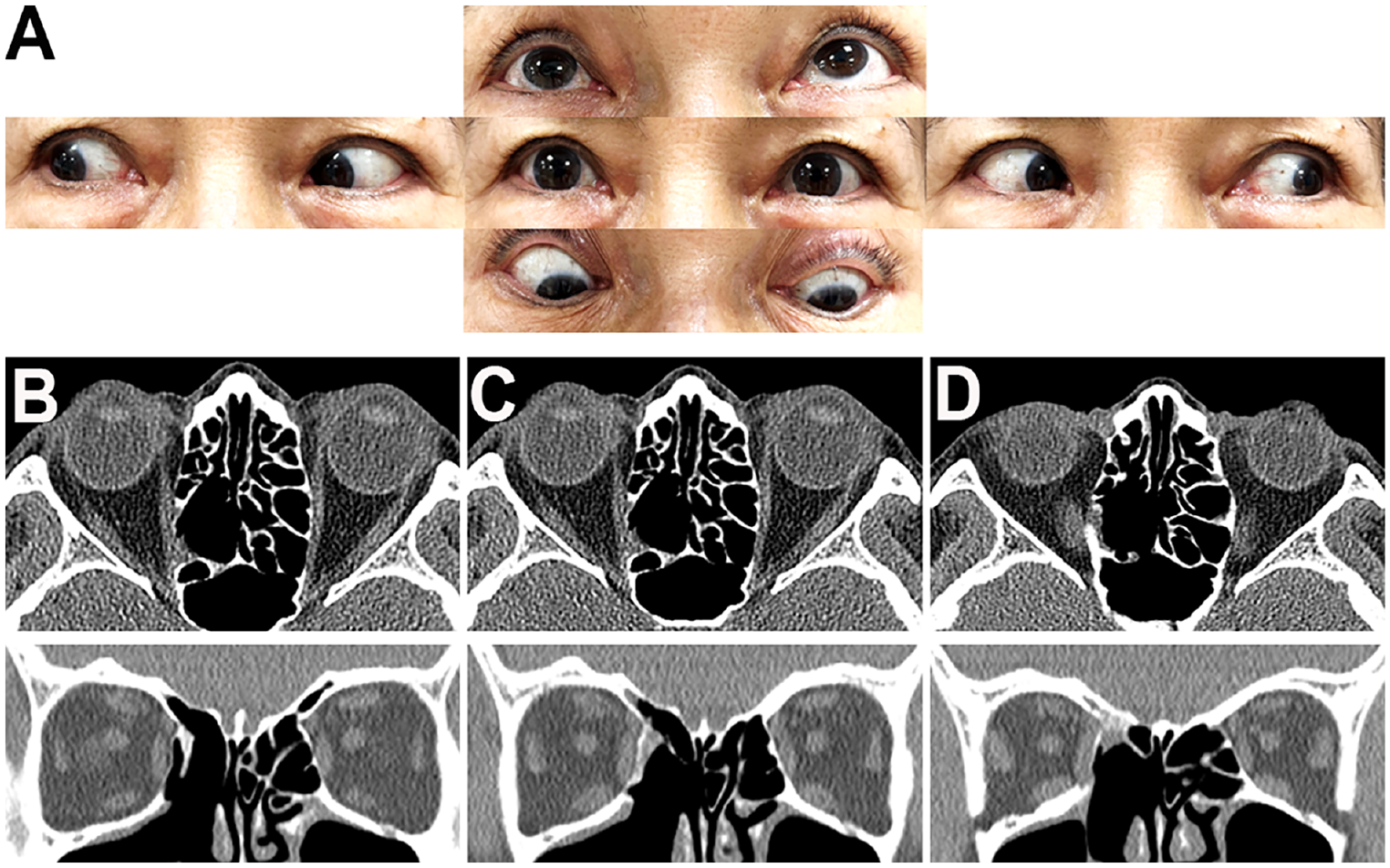
(A) Patient displayed normal movement of the right eye and symmetric upper lid level after 6 months of follow up. (B-D) Postoperative axial and coronal view CT scan of the paranasal sinus showing normal structure of the medial rectus muscle and the orbit without recurrence of mucocele. CT, computed tomography.
Mucoceles are benign, cystic lesions filled with mucus or mucopus and are commonly found within the paranasal sinuses. Mucoceles are often the reason underlying the obstruction of natural sinus drainage pathways and subsequent chronic inflammation. Most are asymptomatic and manageable with regular observation. However, because of their characteristics of growing slowly and tending to expand, they might easily cause a mass effect with localized aggressive behavior, affecting nearby anatomical structures such as the orbital wall, cranial nerves, and skull base. 1 Typical manifestations include headache, orbital pain, and unilateral nasal obstruction.1,2 In severe cases involving the orbital apex, mucoceles may impair the functions of the optic and cranial nerves, leading to vision loss, visual field defects, afferent pupillary defects, optic disc swelling, restricted eyeball motion, and diplopia.
Mucoceles are predominantly diagnosed using imaging studies, with CT and magnetic resonance imaging providing crucial details regarding their location, size, and effects on surrounding structures. Some likely similar diagnoses include neoplasms, abscesses, and other cystic formations of the sinuses. Therefore, relevant imaging findings must be carefully interpreted and matched with clinical presentations.
Oculomotor nerve dysfunction, manifesting as diplopia and ptosis, could have various etiologies, including third cranial nerve palsy and other neuromuscular disorders. 2 Oculomotor nerve dysfunction not accompanied by inflammation or trauma may be related to mechanical compression exerted by expanding mucoceles. The proximity of the posterior ethmoid sinus to the orbit makes orbital structures particularly vulnerable to the effects of compression. The consequent bone erosion can result in the compression or stretching of the oculomotor nerve, and this might cause temporary or permanent damage, which manifests as the symptoms presented by our patient.
According to the literature and previous case series, no significant gender disparity exists in mucocele occurrence, with typical presentations occurring between the ages of 40 and 60 years. 1 The frontal sinus is the most commonly affected by mucoceles; however, the prevalence of mucoceles in the other sinuses is inconsistent among case series. For example, Lee et al reported that the ethmoid was the most commonly affected by mucoceles, followed by the maxillary and sphenoid sinuses, 1 whereas Plantier et al reported that the maxillary sinus was the most commonly affected by mucoceles, followed by the ethmoid and sphenoid sinuses. 3
Regarding ophthalmologic manifestations and postoperative outcomes, Lee et al reported that 67 of the 82 mucoceles (81.7%) detected in their study showed orbital involvement, primarily manifesting as ptosis and periorbital swelling. 1 The postoperative recurrence rate was relatively low. Kim et al revealed that 18 cases (18.8%) in their study involved optic neuropathy, characterized by visual acuity deterioration and unilateral relative afferent papillary defects; surgical intervention resulted in improvements in vision. 2 Plantier et al observed ocular symptoms in 43.5% (20/46) of the cases they reviewed, highlighting the high frequency of ocular involvement in patients with sinus mucoceles. 3 Previous case studies involving mucoceles limited to the ethmoid sinus have reported inconsistent prognostic outcomes regarding the functional recovery of the optic and cranial nerves after surgery.4,5
The case presented herein provides a compelling narrative on the complexity of diagnosing and managing paranasal sinus mucoceles. The diversity of symptoms reflects the potential of mucoceles for expansion, and subsequent compression or displacement of proximal critical structures, such as the orbit or cranial cavity, can have significant clinical implications.1,2 This case highlights several aspects of otolaryngology and ophthalmology, demonstrating the necessity of an interdisciplinary approach for effective treatment.
Footnotes
Author Contributions
The specific role and contribution of each author is as following: Chia-Ho Chen: first author and preparation of draft. Hsin-Chien Chen: corresponding author and editing of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-113006 to Hsin-Chien Chen).
Patient’s Consent
The patient consent statement was informed and approved by Tri-Service General Hospital Institutional Review Board.