
Abstract
Keywords
Introduction
Adenomas with neuroendocrine differentiation are classified as neuroendocrine neoplasms (NEN). NENs, a group of biologically and clinically heterogeneous neoplasms, originate from widely distributed primitive precursors or neural crest cells, with the lungs, gastrointestinal tract, and pancreas being the most common sites of origin.1-3 Neuroendocrine tumors in the middle ear, also known as middle ear adenomatous neuroendocrine tumors (MEANTs), are exceedingly rare and account for <2% of all middle and inner ear tumors. 4 Less than 150 cases have been reported in the English literature under various titles, including carcinoid tumors, middle ear adenomas, adenomatous tumors of the middle ear, adenocarcinoid tumors, and amphicrine tumors. 5 The first documented primary adenomatous tumor confined to the middle ear cleft was reported in 1976. 6 Murphy et al 7 reported middle ear tumors with histochemical and ultrastructural neuroendocrine characteristics consistent with carcinoids (unique argyrophilic and neuroendocrine granules in the cytoplasm). 8 MEANTs are believed to originate from the epithelium lining the middle ear mucosa, 9 an extension and modification of the respiratory epithelium. Ciliary activity, similar to that in other respiratory organs, has been found in the eustachian tube and middle ear, with stronger activity observed in cells distal to the eustachian tube. 10
Two decades ago, MEANTs exhibited indolent biological behavior characterized by a benign histological appearance and slow local growth.6,9 Patients with MEANTs often present with nonspecific symptoms, including progressive conductive or mixed hearing loss, aural fullness, tonal tinnitus, and otalgia. Consequently, MEANTs can mimic more common middle ear pathologies, such as temporal bone paraganglioma (TBPs), cholesteatoma, and chronic otitis media during the initial clinical evaluation. Classically, carcinoid syndrome is characterized by the presence of diarrhea, cutaneous flushing, wheezing/asthma-like symptoms, and pellagra-like skin lesions with hyperkeratosis and pigmentation at some point during the disease. 11 However, an increasing body of literature has shown that some patients with MEANT experience local recurrence, involvement of neck lymph nodes, liver and bone metastases, and mortality.12-14 In 2008, Gaafar reported a case of increased density in the middle ear, which was initially interpreted as a cholesteatoma. Tympanoplasty was performed, and the pathological diagnosis revealed middle ear adenoma/carcinoid with positive surgical margins. Subsequently, the patient underwent radiation therapy but ultimately succumbed to liver metastasis and tumor invasion of the middle cranial fossa. The period from initial diagnosis to death is 11 years. 12 To manage these patients more accurately, Marinelli proposed a tumor node metastasis (TNM) staging system for MEANTs. 5
In most localized cases, surgical excision is the primary recommended treatment. Suitable and complete surgical resection based on the tumor staging system is critical for the prognosis of MEANTs. 15 Given the nonspecific clinical manifestations in patients with MEANTs, preoperative imaging is necessary for accurate diagnosis and treatment planning. 5 Herein, we reviewed the clinical and imaging data of 10 patients with MEANT diagnosed by pathology and discussed the possible origin/predilection site, imaging manifestations, and intraoperative findings of the tumor to enhance clinicians’ understanding of the disease.
Patients and Methods
Basic Information
A retrospective analysis was conducted on the clinical data of 10 patients with pathologically confirmed middle ear adenomas who underwent surgical treatment at the Eye and ENT Hospital of Fudan University between March 2016 and March 2023. These data included information on patient age, sex, symptoms, preoperative diagnosis, results of electrical audiometry, otoscopy findings, imaging data [computed tomography (CT) and magnetic resonance imaging (MRI)], intraoperative findings, pathological features, surgical methods, and prognosis. Patients were classified based on preoperative imaging examinations combined with intraoperative findings according to the TNM staging system described by Marinelli et al. 5 Facial nerve dysfunction was graded according to the House–Brackmann grading system. 16
Statistical Methods
Statistical methods included summarizing continuous variables with medians and categorical variables with frequency counts and percentages. Statistical analyses were performed using Prism 8. All tests were two-sided, and P-values <0.05 were considered statistically significant.
Ethics
This study was approved by the Ethics Committee of the Eye, Ear, Nose, and Throat Hospital of Fudan University (Shanghai, China). All the examinations and treatments were performed in accordance with the Declaration of Helsinki.
Results
Clinical Characteristics
All patients presented with unilateral onset. Among the 10 patients, there were 5 males and 5 females, with ages ranging from 29 to 62 years and a median age of 39.3 years (Table 1). Based on the preoperative imaging examination and intraoperative findings, the distribution of cases was as follows: 1 case of T2aN0M0 and T2bN0M0, 6 cases of T2cN0M0, and 2 cases of T3N0M0 (Table 1). The most common clinical symptoms were mixed or conductive hearing loss (n = 8) and ear pain (n = 6). Other symptoms included tinnitus (n = 6), ear tightness, otorrhea, vertigo, and facial paralysis (Table 1). Among the 10 patients, 8 underwent pure-tone audiometry to evaluate the hearing status in the affected ear, and 4 patients presented with conductive hearing loss (air conduction ≤25 dB), with an average age of 32.75 ± 2.14 years old. The remaining 4 patients exhibited mixed hearing loss (bone conduction >25 dB), with an average age of 46.25 ± 7.98 years old (Table 1). The average air and bone conduction were 61.5 ± 22.81 dB and 29.25 ± 13.03 dB. The average air-bone gap is 32.25 ± 10.82 dB. No significant difference existed in bone conduction between the affected and contralateral ears. We assessed the patients’ postoperative hearing. Among the 10 patients, 2 underwent subtotal temporal bone resection without routine hearing review, 1 patient did not receive a postoperative hearing report due to loss to follow-up, and the remaining patients underwent hearing tests within 6 months after surgery. Postoperative hearing examination showed a reduction in air-bone conduction, with air-bone conduction fluctuating between 10 and 18 dB and an average air-bone conduction of 13.286 ± 1.554 (n = 7).
A summary of Demographic Data, Clinical Features, Treatments, and Outcomes of the Patients.
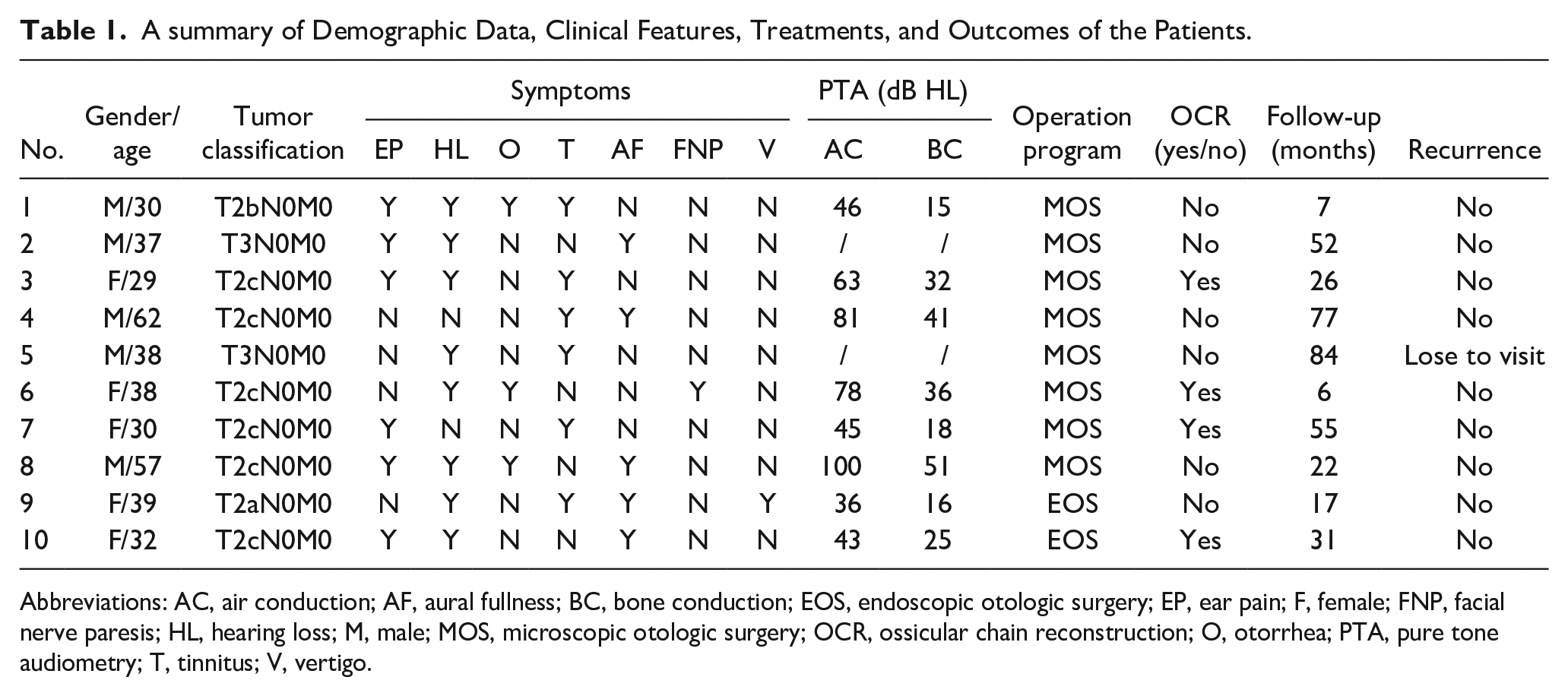
Abbreviations: AC, air conduction; AF, aural fullness; BC, bone conduction; EOS, endoscopic otologic surgery; EP, ear pain; F, female; FNP, facial nerve paresis; HL, hearing loss; M, male; MOS, microscopic otologic surgery; OCR, ossicular chain reconstruction; O, otorrhea; PTA, pure tone audiometry; T, tinnitus; V, vertigo.
The preoperative diagnosis of patients varied and included middle ear mass, external auditory canal mass, external auditory canal cancer, chronic suppurative otitis media, peripheral facial paralysis, tympanic membrane tumors, middle ear cholesteatoma, chronic otitis media, and external auditory canal cholesteatoma. However, all 10 patients were ultimately diagnosed with middle ear adenoma based on postoperative pathology and underwent tumor resection or tympanoplasty.
Smooth, Vascular, Non-pulsatile Mass in the External Auditory Canal Should Be Alerted to MEANTs
Ear endoscopy examination reports were available for 7 patients. The most frequent endoscopic appearance of the ear was a smooth, vascular-rich, non-pulsatile mass filling the external auditory canal, typically appearing quasi-circular (cases 3, 7, 8, and 10; Figure 1c). One patient exhibited an intact and bulging tympanic membrane (case 1, Figure 1a), while another exhibited secretory otitis media with complete invagination of the tympanic membrane and tympanic effusion (case 9, Figure 1d). Case 6, a patient presenting with ear discharge and facial paralysis, showed granulation and white secretions in the external auditory canal on ear endoscopy (Figure 1b). In summary, the endoscopic manifestations of middle ear adenomas are diverse, with the most prevalent presentation being a smooth, vascular, and non-pulsatile mass within the external auditory canal.
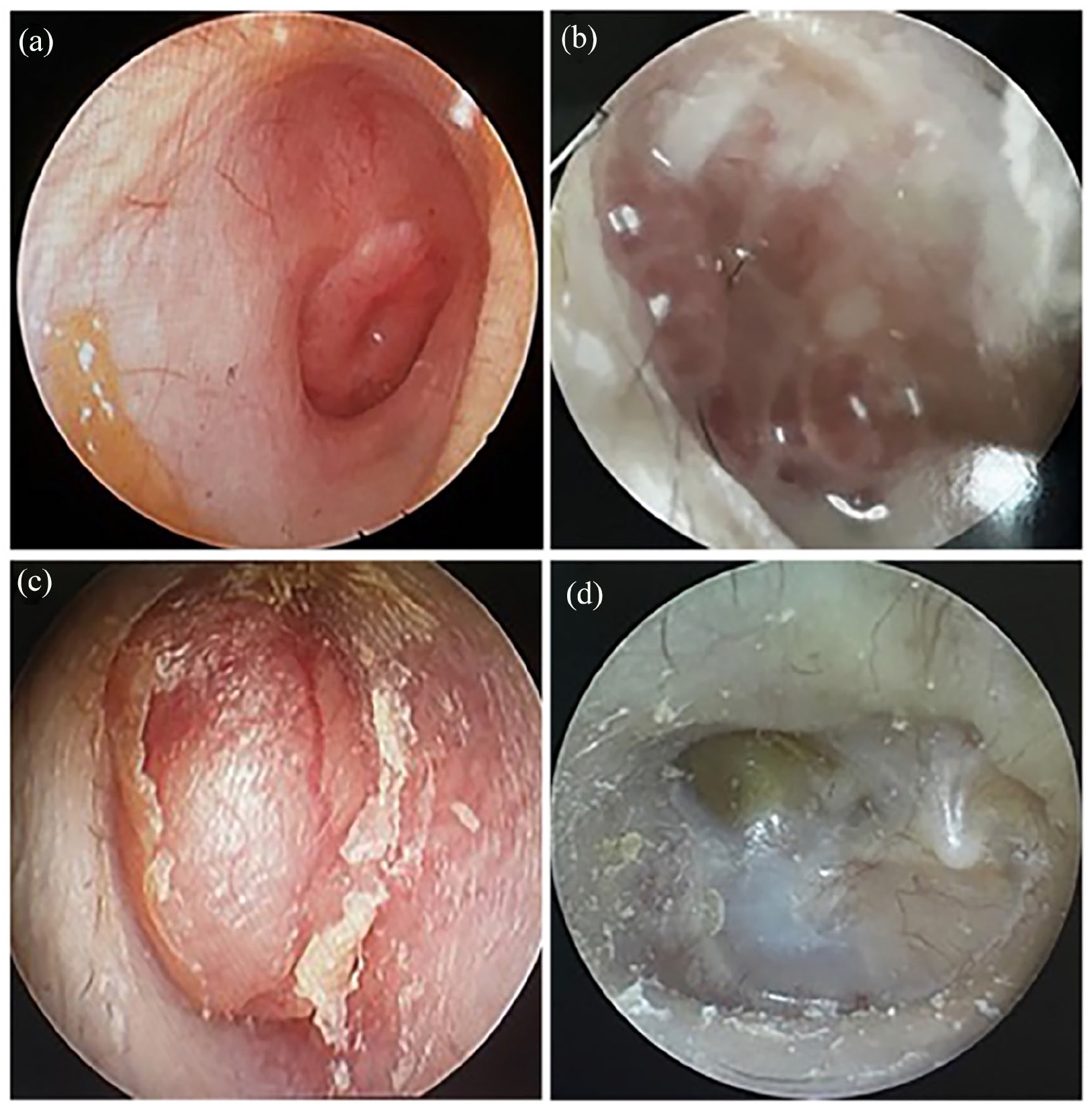
Patients with MEANTs have diverse endoscopic manifestations. (a) The eardrum is intact and bulging (case 1). (b) Granulation of external auditory meatus with secretion (case 6). (c) Smooth tumors in the external auditory canal (case 3). (d) Complete invagination of the tympanic membrane, with tympanic effusion (case 9). MEANT, middle ear adenomatous neuroendocrine tumor.
Imaging Features of MEANTs
CT was available for all 10 cases, revealing consistent findings of middle ear and mastoiditis characterized by soft tissue lesions within the tympanic cavity and sinuses. Furthermore, certain tumors showed invasion of the ossicles (Figure 2c and d), whereas several cases displayed sclerotic lesions within the tympanic cavity and eustachian tube (Figure 2a, b and c; blue arrow). A few cases also exhibited bone resorption and destruction (Figure 2a and d, orange arrow). Nine patients underwent MRI, which did not reveal specific manifestations but revealed soft tissue lesions in the middle ear (Table 2). On T1-weighted imaging, iso-intensity was observed in 6 cases, with a slightly high signal in 2 cases and an equal or slightly low signal intensity in 1 case. T2-weighted imaging showed a high signal in 5 cases and an equal or slightly high signal in 4 cases. Enhancement was observed in 5 cases, while 3 cases exhibited uneven enhancement. Notably, 3 cases showed tumor involvement in the eustachian tube (cases 1, 3, and 9). Diffusion-weighted imaging (DWI) did not demonstrate specificity or diagnostic value; 6 cases showed diffusion limitation, while 3 cases showed diffusion restriction (Figure 3).
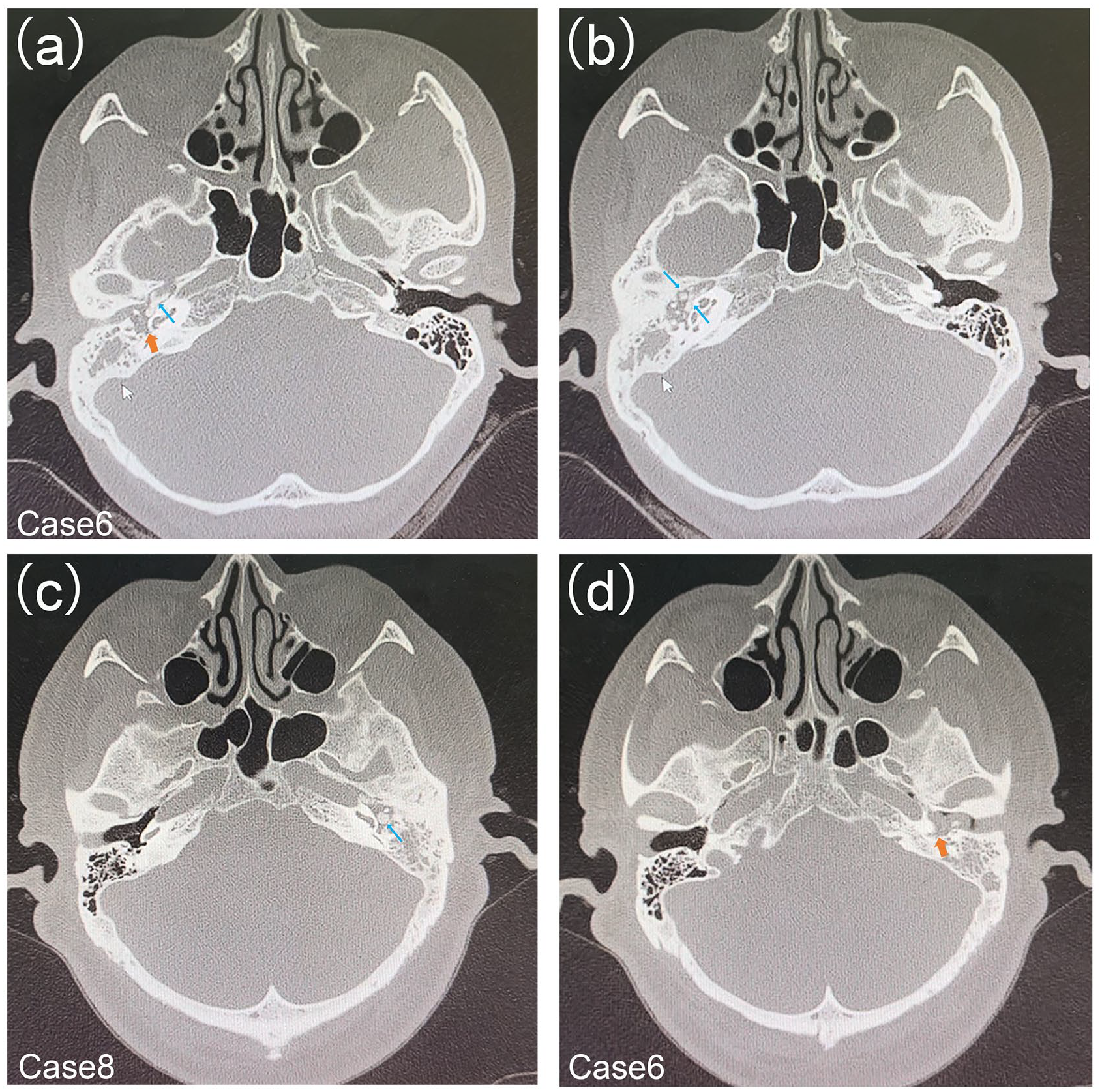
Computed tomography imaging of MEANTs. Soft tissue lesions (a, orange arrow) can be seen in the tympanic chamber, and sclerotic lesions (b, blue arrow; c, red arrow) can be seen in the tympanic chamber and eustachian tube. The ossicular chain is surrounded by a mass with partial bone resorption and destruction (c, d).
Magnetic Resonance Imaging Findings of 9 Patients with MEANT.

Abbreviations: AE, apparent enhancement; E, enhancement; ET, eustachian tubes; H, hyperintensity; I, iso-intensity; IE, inhomogeneous enhancement; ME, mild enhancement; MEANT, middle ear adenomatous neuroendocrine tumor; RD, restricted diffusion; SH, slightly high signal intensity; SL, slightly low signal intensity; UD, unrestricted dispersion.
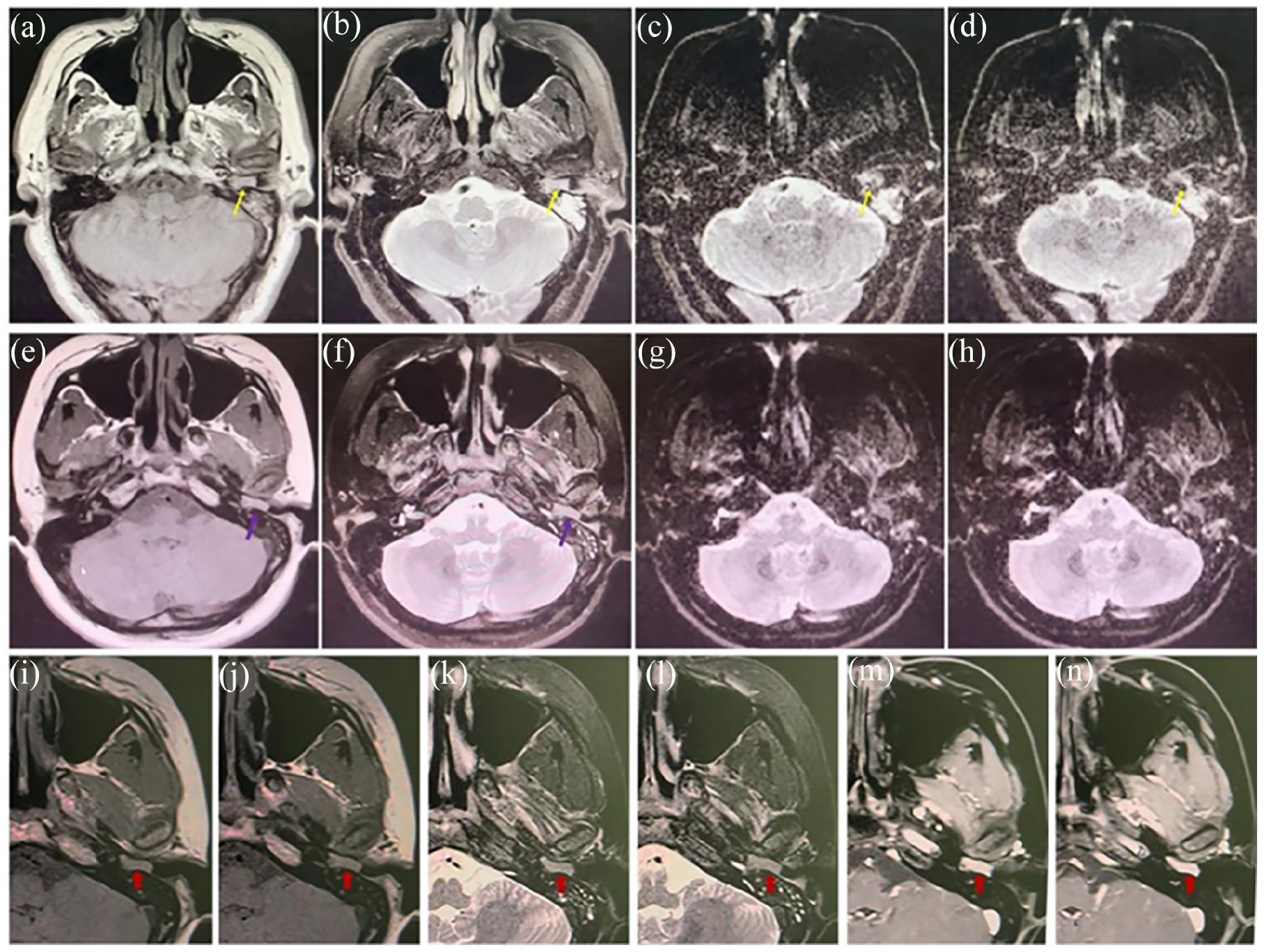
The manifestation of middle ear adenoma on magnetic resonance imaging (case 8 and case 3). (a) T1 shows moderate signal, (b) T2 shows high signal, (c, d) DWI diffusion is limited, involving deep external auditory meatus (yellow arrow). (e) TI shows a moderate signal and (f) T2 shows a slightly high signal (purple arrow). (g, h) DWI shows no significant diffusion limitation. (i-n) Soft tissue lesions in the tympanic cavity, presenting as iso-intensity with T1 and slightly high signal with T2, enhanced markedly after enhancement in case 3. DWI, diffusion-weighted imaging.
Pathological Features of MEANTs
The primary pathological features include CD56 positivity or weak positivity, CKpan positivity, Syn positivity or partial positivity, and S100 negativity, with Ki67 expression ≤3%. Other pertinent indicators encompass CK8, Vimentin, CHG, P63, CK7, etc. (Table 3).
Summary of Immunohistochemistry Data of the Patients in This Series.
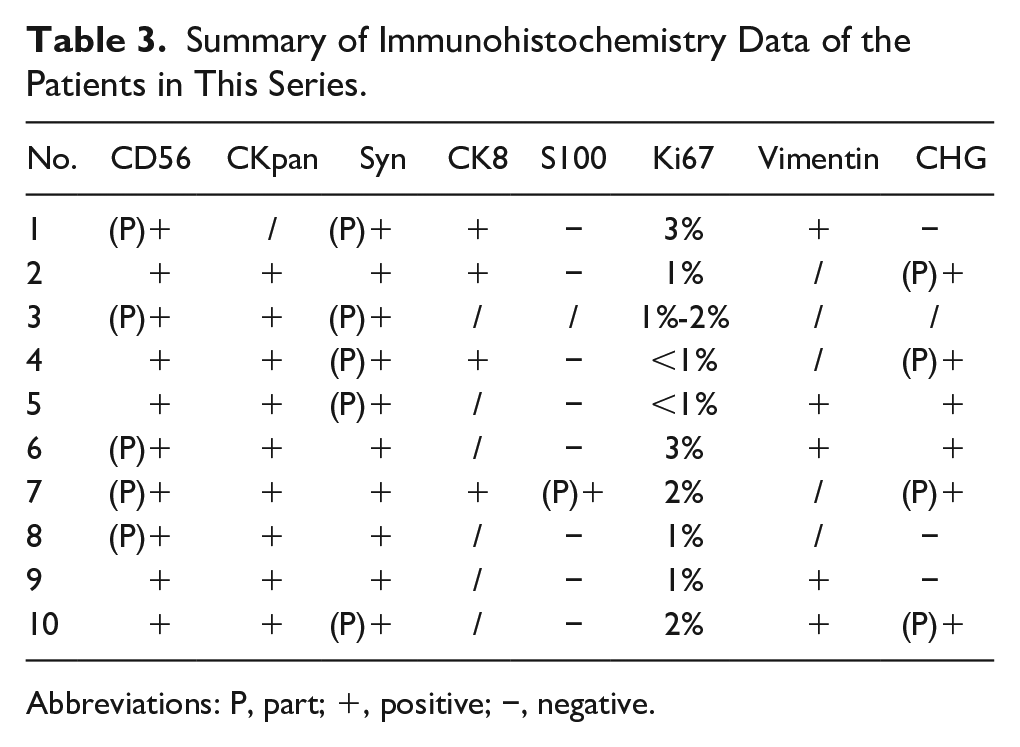
Abbreviations: P, part; +, positive; −, negative.
Treatment and Prognosis of MEANTs
All the patients underwent surgical resection. Among the 10 patients, 2 underwent lateral temporal bone resection, and postoperative imaging examinations revealed no significant recurrence. Two patients underwent endoscopic tumor resection, and postoperative imaging showed no significant tumor progression (cases 9 and 10). Six patients underwent an open tympanoplasty and ossicular chain reconstruction. None of the patients underwent radiation therapy, chemotherapy, or adjuvant systemic therapy with a somatostatin analog. The follow-up period for all the patients ranged from 6 to 84 months. With the exception of 1 patient lost to follow-up, 9 patients showed no significant tumor progression during the postoperative follow-up (7 patients did not experience tumor recurrence after surgery; 2 patients were found to have residual tumors on postoperative imaging, but no tumor progression or enlargement was detected in the subsequent follow-up). The surgeries and prognoses are detailed in Table 1. Intraoperative descriptions of the tumors revealed new bone formation or organisms in the middle and lower tympanic chambers and pharyngeal tube openings during surgery, corresponding to the imaging findings. Five patients had tumors involving the tympanic opening of the eustachian tube during surgery, with new bone obstruction observed in 2 cases and new organisms present around the tympanic opening of the eustachian tube in 3 cases. Four patients had tumors in the middle and lower tympanic cavities. Other intraoperative descriptions of the tumors included being yellow and bright in appearance in 2 cases, the presence of cholesterol crystals or granulation in 2 cases, and being easily prone to bleeding in 2 cases.
A Special Case Predicts the Development Process of MEANTs
A 39-year-old woman presented with hypoacusis in the right ear, accompanied by tinnitus and stuffiness. The endoscopic appearance of the ear resembled that of secretory otitis media, characterized by complete invagination of the tympanic membrane and tympanic effusion (Figure 4M). CT revealed increased density in the middle and lower tympanic chambers of the middle ear, which was initially interpreted as a cholesterol granuloma (Figure 4A-F). During this period, the patient underwent grommet insertion at another institution due to symptoms. However, after a few months, the patient’s symptoms did not improve after removal of the ventilation tube.
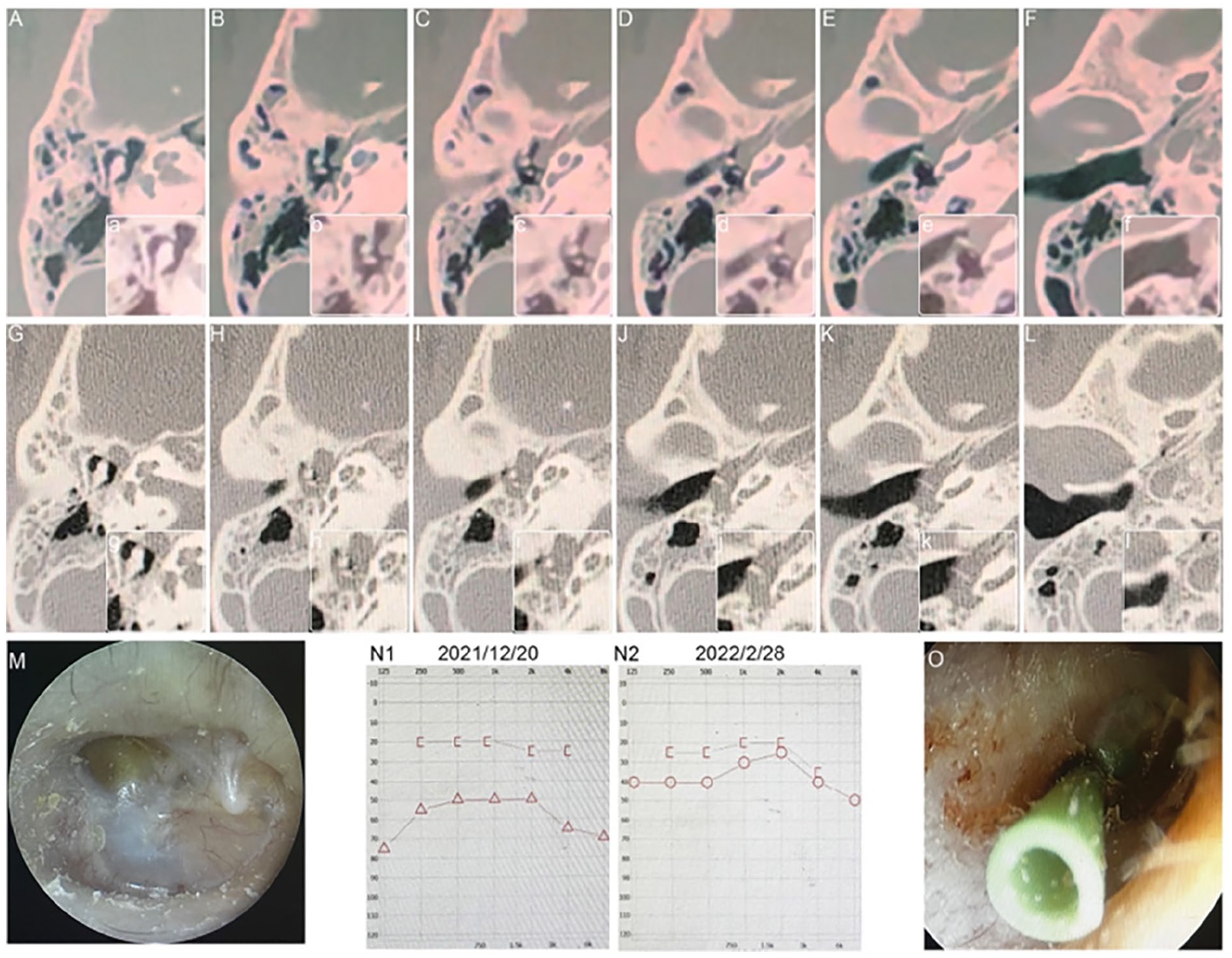
A special case (case 9) predicts the development process of MEANTs. (A-F; a-f) CT scans showed an increased density in the middle and lower tympanic chambers of the middle ear and did not invade the ossicular chain in December 2018. (G-L; g-l) The CT scan showed that the tumor filled the middle ear cleft and encased the ossicles with ossicular bone erosion 2 years later. (M) Before surgery, the tympanic membrane shows a sign of middle ear effusion. (N) Preoperative and postoperative hearing test results of the patient. (O) Tympanum exploration and tympanic membrane catheterization were performed. CT, computed tomography; MEANT, middle ear adenomatous neuroendocrine tumor.
Two years later, the patient consulted our institution again for the symptoms. Examination revealed signs of middle ear effusion in the tympanic membrane (Figure 4G-L). CT (Figure 4G-L) and enhanced MRI scans indicated that the lesion was larger than before, with imaging still suggesting inflammatory lesions, possibly cholesterol granulomas. Subsequently, tympanic exploration and catheterization were performed (Figure 4O), and the observed material was diagnosed as a middle ear adenoma/carcinoid tumor.
Six months later, the ventilation tube of the tympanic membrane fell off spontaneously, and the patient remained symptomatic, prompting another consultation. Soft tissue lesions in the lower tympanic cavity and pharyngeal tube openings were detected using a CT scan and contrast-enhanced MRI. Subsequently, the tumor was resected. Hearing has recovered well (Figure 4N1-2). After 6 months, a CT scan revealed no significant recurrence.
From the imaging findings of the patient, it is evident that the tumor originated from the middle and lower tympanic chambers and the pharyngeal tube opening area. In the early CT scan, the tumor was observed in the inferior tympanic chamber without invading the ossicular chain (Figure 4a-f). However, over 2 years, the tumor grew slowly and completely enveloped the ossicles (Figure 4g-l). In similar cases, tumors commonly occur in the middle and lower tympanic chambers, often leading to obstruction of the eustachian tube by the tumors and new bone formation. Therefore, we speculate that the tumor may have originated from the middle ear mucosa in the middle and lower tympanic chambers, and the oropharyngeal region.
Discussion
Neuroendocrine adenoma is an extremely rare pathology, accounting for less than 2% of all ear tumors. This study aimed to improve physicians’ understanding of the disease and increase the diagnostic rate by summarizing the imaging characteristics and intraoperative findings of 10 patients with pathologically diagnosed middle ear adenomas. The incidence of MEANTs was comparable in females and males. Previous studies reported a high incidence in both women 17 and men. 5 The most common symptoms were hearing loss and earache, which is consistent with previous reports.5,15,17 Patients with mixed hearing loss had an average age of 46.25 years old, which is higher than that of patients with conductive hearing loss (32.75 years old), suggesting that MEANTs manifest as conductive deafness. Some studies have reported that facial nerve palsy can be caused by MEANT. 18 Acute-onset facial palsy induced by MEANTs is rare. For a patient who has already developed facial paralysis, early complete excision of the tumor is recommended, not only as a curative treatment but also for restoration of facial function. Preserving the facial nerve as much as possible during surgery is recommended, as these tumors are low-grade malignancies, and recurrence is rare after complete excision of the tumor during primary surgery. In reported cases, facial nerve function fully recovered within 3 weeks to 3 months after surgery.18,19 In our study, we also found a case of a 36-year-old woman who presented to our emergency department with acute-onset facial nerve paralysis and otitis media. During the 6 months follow-up after tumor resection, the patient showed significant recovery from facial paralysis, indicating that the tympanic part of the nerve was compressed rather than directly invaded.
The clinical manifestations of MEANTs are nonspecific and often overlap with those of other middle ear diseases, such as temporal paraganglioma, cholesteatoma, chronic otitis media, and masses in the external auditory canal.
Middle ear cholesteatomas, middle ear malignant tumors, and middle ear adenomas can manifest as middle ear soft tissue masses with ossicular involvement, sclerotic lesions of the tympanum, bone resorption, and destruction. TBPs are highly vascular, typically benign neoplasms that occur within the temporal bone. They are relatively common among temporal bone tumors, comprising approximately 0.6% of all head and neck tumors, and are the most prevalent tumors affecting the middle ear. They often present with pulsatile tinnitus and a red/hypervascular mass located medial to the tympanic membrane, typically originating in the hypotympanum or mid-promontory. These masses commonly exhibit deep red hues when endoscopically visualized. 20 By contrast, MEANTs may originate from the mucosal epithelium of the middle ear, including the eustachian tube. The most common MEANTs are typically smooth, vascular, and non-pulsatile masses within the external auditory canal (Figure 1c). Our observation of a case resembling secretory otitis media, with complete invagination of the tympanic membrane and tympanic effusion (Figure 1d), underscores the diversity of MEANTs. Furthermore, this study displayed a 1:1 male-to-female ratio, indicating a significant female predilection for TBPs. 21 The age of onset of TBPs typically falls between 40 and 60 years, 21 whereas MEANTs affect a relatively younger demographic with an average age of only 39.2 years. CT with thin cuts of the temporal bone has proven very useful for diagnosing middle ear lesions and assessing bone involvement. However, its ability to distinguish and evaluate soft tissue changes is limited. The combination of CT and MRI has remarkably improved the diagnostic accuracy for middle ear lesions. A cholesteatoma is a middle ear lesion composed of squamous cell debris, and surgical resection is required owing to its local invasiveness. 22 Conventional cholesteatoma MRI images display only nonspecific intermediate signal intensities on T1-weighted images and hyperintense signal intensities on T2-weighted images without significant enhancement. DWI has been developed as an important tool for the detection of cholesteatoma, with a sensitivity and specificity of 94%.23,24 Nonetheless, factors such as the presence of external auditory meatus, dental braces, abscess cavities, or silastic sheets identified during previous surgeries may cause false negatives with regard to the DW-MRI signal.5,25-27 In most cases, MEANTs showed iso-intensity on T1-weighted imaging, hyper-intensity on T2-weighted imaging, and enhancement or heterogeneous enhancement after enhancement (Table 2). Previous studies have shown that MEANTs do not exhibit restricted diffusion. 5 However, some cases in our study showed restricted diffusion on DWI (Figure 3c and d; Table 2). Therefore, we believe that restricted diffusion is not the only criterion for distinguishing between MEANTs and cholesteatomas. Cholesterol granuloma in the middle ear can manifest as bone erosion, passivation of the tympanic shield, and ossicle involvement. However, the disease has no history of tympanic membrane perforation and is characterized by a typical blue eardrum, often accompanied by clinical manifestations of tinnitus. The T1 high signal on MRI is a specific sign. 28 Tympanic choroidal paraganglioma shows focal soft tissue masses covering the lateral wall of the inferior tympanic chamber cochlear promontory, without obvious bone erosion. Characteristically, they exhibit a light pink coloration and are non-pulsatile. Larger lesions can fill the middle ear cavity and erode the ossicles, eustachian tube, and mastoid process. It is isointense on T1-weighted imaging, hyperintense on T2-weighted imaging, and significantly homogeneous after enhancement.
Ki67 is a proliferating cell-related antigen that plays a crucial role in cell division and tumor cell proliferation. A high Ki67 index indicates active cell proliferation, potentially signaling malignant tumor risk. Conversely, a low Ki67 value generally indicates less active cell proliferation, suggesting the presence of benign tumors. In our study, the pathological results showed a Ki67 index below 3%, indicating low cell proliferation, which is consistent with the presence of benign tumors.
The tympanic cavity mucosa was pale white, thin, and devoid of blood vessels. It was connected to the pharyngeal mucosa through an eustachian tube. The middle ear mucosa surface is a ciliated respiratory mucosal scaffold secreting mucus. Various mucociliary distribution pathways merge at the tympanic opening of the eustachian tube, forming an important component of mucosal excretion in the middle ear cavity. However, ciliated cell distribution varies in different parts of the middle ear cavity, decreasing from the opening of the pharyngeal canal to the tympanic promontory. Imaging of the patients, particularly in typical cases (Figure 4), revealed tumors in the middle and lower tympanic chambers and the pharyngeal tube opening area. In the early stages, tumors did not invade the ossicular chain but often obstructed the eustachian tube and led to new bone formation. Therefore, we speculate that the tumor originated from the middle ear mucosa in the middle and lower tympanic chambers and the oropharyngeal region.
Complete surgical removal is the primary treatment for MEANTs. 15 Neither local resection nor tympanotomy is recommended for the management of MEANTs. The local recurrence rate after tympanoplasty was significantly higher than after radical mastoidectomy. Due to limited anatomical space, complete tumor resection is difficult to achieve, and most MEANTs are performed in a fragmented manner. Ossicular chain involvement is common, making its management crucial in primary and recurrent diseases. In a previous study, only 1 patient who developed recurrent disease had an intact ossicular chain retained during initial treatment 15 ; therefore, it was necessary to remove the ossicular chain. In this study, all patients underwent surgical treatment, with 2 patients undergoing endoscopic ear tumor resection (cases 9 and 10). Postoperative imaging revealed no significant recurrence or enlargement of the tumors during postoperative follow-up. Surgery should be tailored based on clinical and radiological findings. Although the incidence of recurrence is higher with tympanotomy than with radical mastoidectomy, data are insufficient to determine statistical significance. 29
The overall recurrence rate is 22% 29 and 9% of patients develop regional metastases. The most common sites of metastases are the cervical lymph nodes,13,14 liver, and bones. 30 Owing to nonspecific clinical presentations in MEANTs, preoperative assessment of lymph node status is challenging. However, we recommend careful neck node detection during follow-up. Recurrent disease usually occurs after an average of 11 years of treatment. Prognostic histopathological/immunohistochemical biomarkers for MEANTs recurrence or malignant progression have not been determined. 31 Overall, 40% of patients with recurrent disease later develop metastases. 29 These data indicate that for patients with recurrence, the malignancy of the tumor may be relatively high, and extensive surgery should be performed. Another case report described a patient who developed iliac crest osseous metastasis 10 years after undergoing resection of a middle ear carcinoid tumor. However, our patient did not have such a long follow-up period, which prevented recurrence survival analysis. Therefore, our results should be interpreted cautiously, and further studies are needed. Although these tumors have long been considered as low-aggression neoplasms, long-term follow-up studies are necessary to confirm this hypothesis.
Conclusion
Patients with MEANT commonly present with nonspecific findings, which can make diagnosis challenging. However, clinicians should consider MEANT when encountering non-pulsatile tumors with clear inner boundaries of the external auditory canal and abundant quasi-circular vessels. In addition, the presence of new bone or a neoplasm at the pharyngeal tympanic canal orifice observed during preoperative examination or surgery should raise the suspicion of MEANT. The primary treatment for MEANTs is complete surgical removal, and long-term clinical follow-up is necessary to monitor for recurrence or complications.
Footnotes
Author Contributions
H.Y. is responsible for the design. D.Y. is responsible for the manuscript draft and implementation of the trial. D.Y., Q.L., and H.Y. are responsible for the implementation of imaging data analysis. All authors contributed to the drafting and approved of the final manuscript.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the 2023 Fudan Clinical Scientist Training Program, Excellent Doctors-Excellent Clinical Researchers Program (SYB202008), the National Natural Science Foundation of Shanghai (21ZR1411800), the National Natural Science Foundation of China(No.82201283), the Shanghai Science and Technology Committee (STCSM) Scienceand Technology Innovation Program(21Y31900500), and Fudan-Fuxin Research funding (FNF202237).
Statement of Ethics
The study has been granted an exemption from requiring ethics approval (the Ethics Committee of the Eye, Ear, Nose, and Throat Hospital of Fudan University, Shanghai, China). Written informed consent was obtained from participants.
Patient Consent for Publication
Obtained.