
Abstract
Introduction
Ménière’s disease (MD) is a complex clinical condition characterized by recurrent vertigo, fluctuating sensorineural hearing loss, ear fullness, and tinnitus. The exact pathogenesis of MD is still unclear, and current treatment aims to control symptoms and reduce the severity and frequency of vertigo attacks. 1 For patients with ineffective conservative treatment for vertigo attacks, intratympanic injections have emerged as a minimally invasive outpatient procedure and an effective treatment option.
The treatment of MD involves medication and surgical interventions with the aim of treating and preventing vertigo attacks, improving or preserving hearing and vestibular function, and preventing bilateral MD. Common surgical methods include labyrinthectomy, vestibular nerve sectioning, and canal plugging. These surgeries can alleviate or eliminate vertigo symptoms but may result in partial hearing loss. Medications used in MD treatment mainly include gentamicin or corticosteroids, which are widely used in clinical practice. These drugs are delivered to the middle ear through the tympanic membrane to reach the inner ear, aiming to alleviate symptoms and help control vertigo attacks. However, intratympanic gentamicin (ITG) may have significant side effects in controlling vertigo, 2 as it can be ototoxic to the inner ear and may result in hearing loss for patients. Conversely, intratympanic injection of corticosteroids are generally well-tolerated, can achieve higher perilymph concentrations, and carries no risk of systemic side effects. Recently, Cao et al 3 conducted a meta-analysis comparing the efficacy of different intratympanic medications for treating MD, showing that long-term treatment with intratympanic methylprednisolone (ITM) had similar efficacy to gentamicin. However, their conclusion was mainly based on 2 comparative studies without any additional supporting evidence, such as hearing tests or speech discrimination scores. On the other hand, Jiang et al 4 conducted a meta-analysis on MD, which suggested that ITG was superior to corticosteroids in controlling vertigo, but this result did not fully consider the diagnostic criteria for MD.
For MD patients who cannot be effectively treated with medication, a number of surgical options, such as endolymphatic shunt (ELS), vestibular nerve section, and labyrinthectomy, can provide definitive treatment for episodic vertigo. However, both labyrinthectomy and vestibular nerve section result in permanent vestibular dysfunction. In contrast, ELS is nondestructive, with a favorable surgical morbidity and minimal impact on hearing. Therefore, in the presence of functional hearing, ELS is a preferred surgical treatment option.
The American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNS) released the fifth edition (AAO-HNS 2020) of the diagnostic criteria for MD in 2020, 5 which includes the following key modifications compared to the AAO-HNS 1995 criteria: (a) elimination of the “certain” and “possible” MD categories, (b) a defined range of vertigo duration lasting from 20 minutes to 12 hours, (c) updated research requirements to improve patient care. Most notably, AAO-HNS 2020 focuses more on clinical interventions, providing specific recommendations for various clinical key issues. It emphasizes the use of appropriate treatment methods to improve acute and chronic symptom control and reduce unnecessary testing and medication treatments. However, there is a lack of randomized controlled trials (RCTs) following the AAO-HNS 2020 guidelines, leading to lower confidence in the results of meta-analysis. Therefore, this study performs network meta-analyses of all RCTs based on the AAO-HNS 1995 MD diagnostic criteria, which can also mitigate heterogeneity issues among the studies. The goal is to determine whether there are differences in the effectiveness of the 2 treatment methods in controlling vertigo and their impact on hearing. This evaluation aims to provide evidence for the selection of MD treatment strategies in clinical practice.
Materials and Methods
Literature Search Strategy
A systematic literature search was conducted in Embase, PubMed, and Medline from 1995 to October 2023. A search strategy using a combination of medical subject terms and text keywords: Meniere’s disease, steroids, glucocorticoids, dexamethasone, methylprednisolone, and gentamicin.
MeSH terms and keywords related to pharmacological included: “steroids,” “gentamicin,” “glucocorticoids,” “dexamethasone,” “methylprednisolone,” and “placebo.” For example, the search strategy in PubMed is (Meniere’s disease) AND (steroids) AND (gentamicin) OR (glucocorticoids) OR (dexamethasone) OR (methylprednisolone) OR (placebo) AND (intratympanic injection).
Inclusion and Exclusion Criteria
Inclusion criteria: (a) Met the diagnostic criteria for MD of AAO-HNS 1995; (b) excluded other diseases causing vertigo; (c) other otologic disorders of the participant were not described. Exclusion criteria: (a) Nonhuman experimental studies, in vitro studies and reviews; (b) other causes of vertigo; (c) studies where full text or accurate rates of raw data extraction were not available; (d) ITG, ITM, and intratympanic dexamethasone (ITD) were not combined with other drugs.
Data Extraction
The Cochrane Risk of Bias Tool for RCTs was used to evaluate the risk of bias of included RCTs. Two reviewers carried out assessments independently and in duplicate, and resolved conflicts via consensus or third-party adjudication. The following information was extracted from the selected literature: first author, year of publication, total number of participants, follow-up time, number of last follow-up, mean age, type of tympanic chamber injection drug, mean and variance of pure-tone average (PTA) audiometry before and after follow-up, number of vertigo control ratings, and number of vertigo and tinnitus recovery at the last follow-up.
Before conducting a network meta-analysis, it is necessary to recalculate the changes in the mean and variance of PTA before and after follow-up. Assuming the mean and variance of PTA before follow-up are represented as m1 and sd1, and after follow-up as m2 and sd2, with the sample size remaining constant at n. The values of the change are represented as m and sd, and can be calculated using the following formulas:


Data Analysis
Relative risk ratio and its 95% confidence interval (CI) for vertigo and tinnitus were calculated using a random effects model, and standardized mean difference and its 95% CI were used for PTA. All data were subjected to meta-analysis using Stata 17 software (StataCorp LLC). We used chi-square test (χ2) values to quantify inconsistencies between studies in each meta-analysis, and the probability of preference ranking curve (SUCRA) to rank the effectiveness of each treatment and to determine the best treatment.
Results
Based on the PRISMA flowchart, inclusion criteria, and exclusion criteria, a total of 13 articles were selected, as showed in Table 1. The total number represents the individuals involved in the studies, some of whom may have discontinued testing during the follow-up period. The number of participants in the experimental and control groups reflects the count at the final follow-up. There are 4 studies on ITG and ITM.6,8,10,18 There are 5 studies comparing ITG with ITD.7,9,11,16,17 Only one study compares ITM with ITD, 12 both ITG and ITD being intratympanic corticosteroid treatments for MD, with follow-up periods exceeding 3 months.
Data Extracted From the Included Literature.
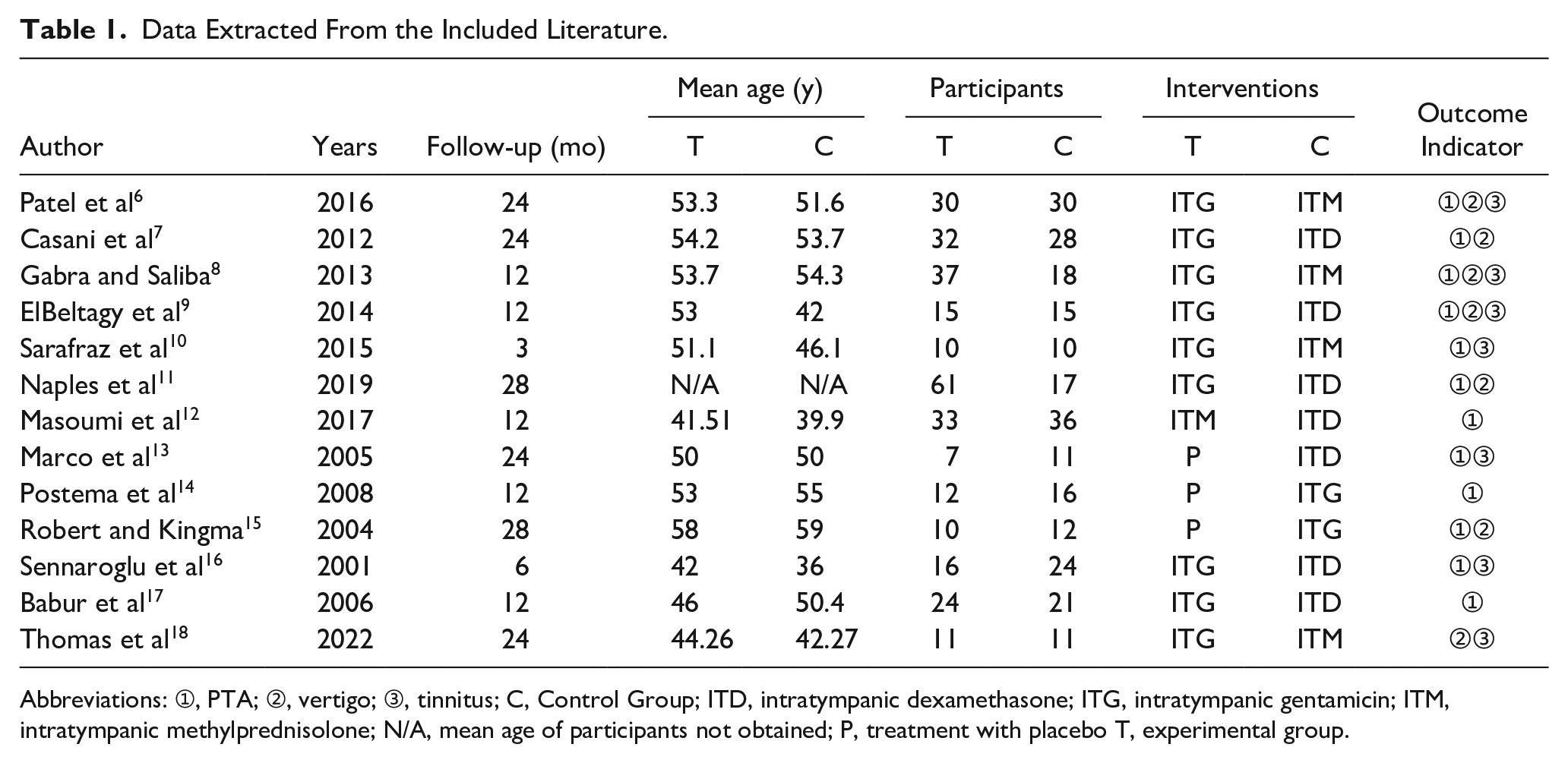
Abbreviations: ➀, PTA; ➁, vertigo; ➂, tinnitus; C, Control Group; ITD, intratympanic dexamethasone; ITG, intratympanic gentamicin; ITM, intratympanic methylprednisolone; N/A, mean age of participants not obtained; P, treatment with placebo T, experimental group.
Quality Assessment
Risk of bias within studies: The results of the risk of bias assessment are summarized and shown in Figure 1. The high risk of bias came generally from incomplete outcome data or other sources of bias such as lacking baseline values, loss to follow-up cases, age differences, inappropriate statistical analysis, or a combination of these factors.
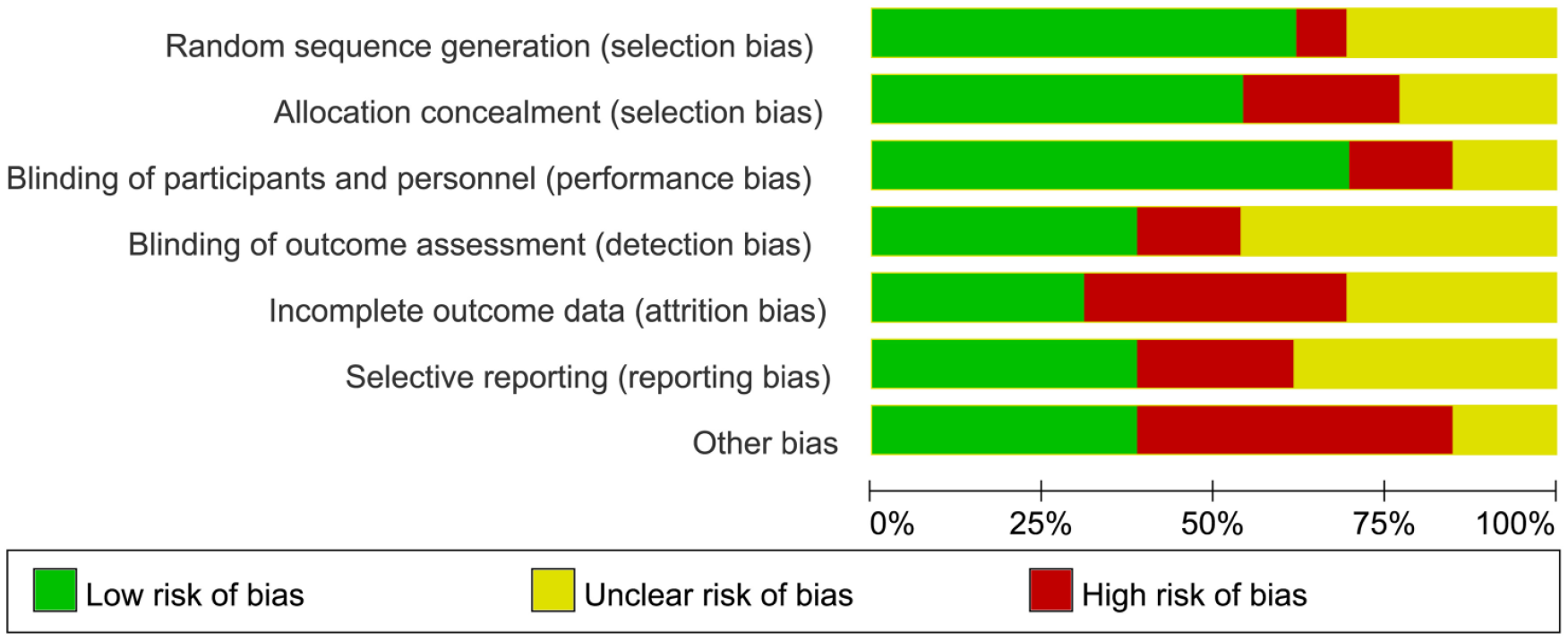
Summary of risk of bias assessment.
PTA Changes
The evaluation of hearing was mainly measured by the change in PTA before and after follow-up, as shown in Table 1; a total of 6 studies with outcome indicators reported PTA. In the 2 articles that studied ITG and ITM, Gabra and Saliba’s 8 study showed that hearing loss improved by 4.30 dB with methylprednisolone compared to gentamicin, while Patel et al 6 study favored ITG, with hearing loss in the methylprednisolone group worsened by a mean of 14.26 dB. Although the study populations were considered similar, the differences in treatment effects may be due to differences in the dose and frequency of the interventions. Considering the conflicting directions of treatment effects, meta-analysis was not performed for these 2 studies.
Three studies7,9,11 reported experimental results for ITG and ITD, and on average, IT gentamicin was associated with some degree of hearing deterioration compared to pretreatment, while ITD may be beneficial in reducing hearing loss. According to a meta-analysis of PTA changes, the mean deterioration of hearing in the ITG group was 0.09 dB [95% CI (−0.42, 0.24)] compared to the ITD group, with no statistically significant comparison between groups.
Vertigo
At the last follow-up, there were 590 reported cases of vertigo, of which 345 achieved complete control of vertigo, and 83 had vertigo but it did not affect their normal life. The complete control rates of vertigo for ITG, ITM, and ITD were 78%, 43%, and 44%, respectively. Gentamicin had the highest control rate for vertigo, while methylprednisolone and dexamethasone showed similar results. Including the 345 individuals who achieved complete control of vertigo in the meta-analysis, as shown in Figure 2, ITG, ITD, and ITM can effectively treat vertigo symptoms in patients with MD.
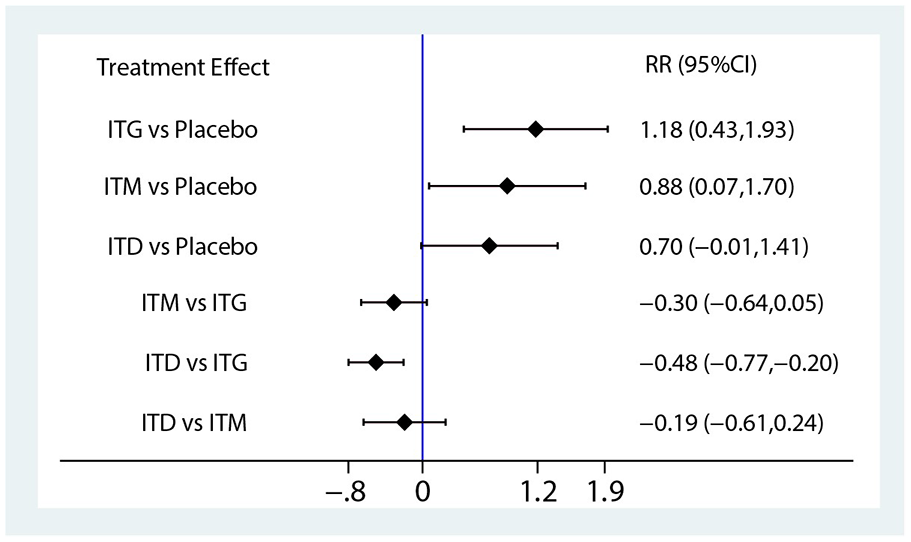
Forest plot of different drugs for vertigo.
The symptoms of MD often fluctuate over time, and any treatment may improve or worsen the symptoms. Therefore, to determine whether intratympanic injection of gentamicin or corticosteroids is truly effective, subgroup analysis of the follow-up time for vertigo treatment effects was performed. For follow-up time of 6 months, 12 months, and 24 months, the network meta-analysis results are shown in Figure 3. In the short term, ITG is significantly better than ITD and ITM. However, as time progressed, the efficacy of ITM increased, while that of ITD decreased. Overall, the subgroup analysis of follow-up time indicated that the optimal efficacy may be observed after a certain period of time with the use of gentamicin or dexamethasone injections, rather than longer treatment duration. Methylprednisolone showed relatively stable results in long-term observation.
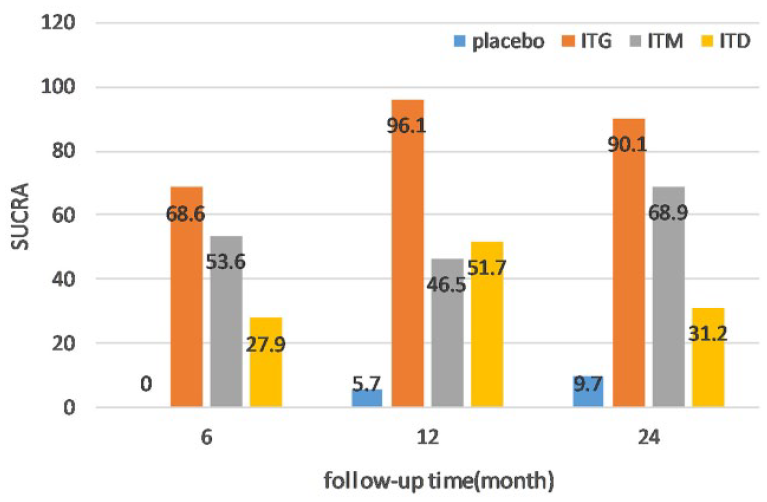
SUCRA values for treatment modalities at different follow-up time.
Tinnitus
Of the 7 studies, 101 participants reported improvement in tinnitus out of a total of 279 after follow-up. The rates of improvement for ITG, ITM, and ITD were 31%, 42%, and 42%, respectively, with methylprednisolone and dexamethasone having better tinnitus improvement rates. Network meta-analysis showed that ITG, ITM, and ITD all showed some improvement in the treatment of tinnitus compared to placebo, with intra-drum injection of dexamethasone (SUCRA = 81.3) showing a better probability of treatment for tinnitus, followed by methylprednisolone (SUCRA = 68.4), and gentamicin (SUCRA = 31.8) being the least effective.
Sensitivity Analysis
As shown in Figure 4, a funnel plot was constructed for the literature included in the treatment of MD, and sensitivity analysis was performed. All included studies fell within the 95% CI, and the studies directly comparing drugs showed an even distribution on both sides of the null line, suggesting a lower probability of small sample effect in the research.
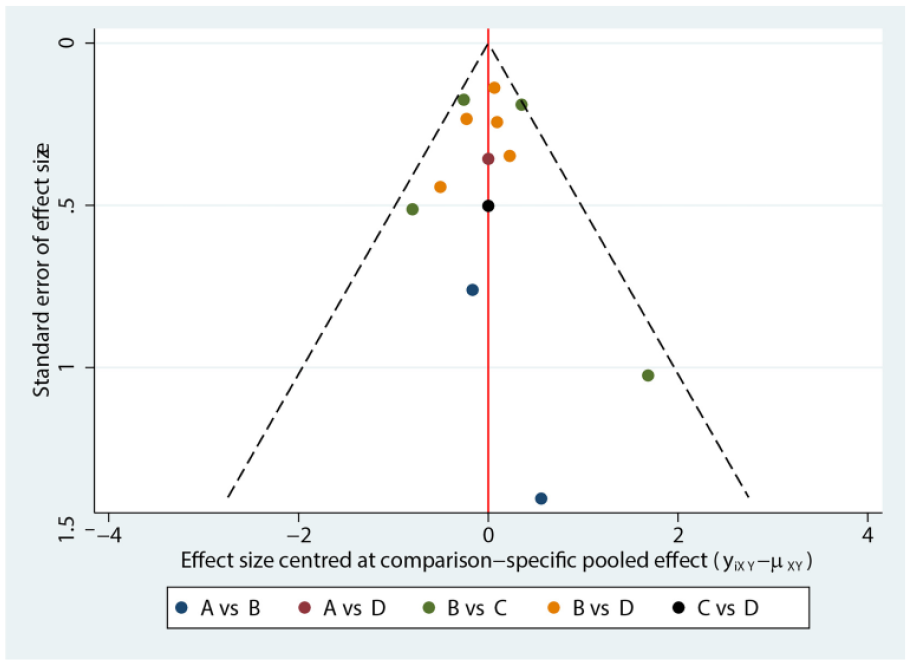
Funnel plot showing publication bias (A = placebo, B = ITG, C = ITM, D = ITD).
Discussion
For patients with MD who do not respond to drug therapy, the use of gentamicin or corticosteroids is a recognized treatment method. However, there is still controversy regarding the clinical efficacy and safety of these 2 treatment methods. In 2011, a Cochrane systematic review evaluated the effects of gentamicin and steroids in the treatment of MD. However, due to the limited sample size, these 2 reviews19,20 did not conduct any meta-analysis at that time. Patel et al 6 conducted a 2 year double-blind RCT, reporting that there was no significant difference in the frequency of vertigo attacks between ITM and ITG in patients with MD. However, they also reported that patients receiving intratympanic steroids were more likely to experience relapses and require repeated injections. Recently, Lee et al 21 and Webster et al, 22 respectively, conducted a meta-analysis, showing that gentamicin was superior to steroids in reducing the frequency of vertigo attacks in the treatment of MD. Regarding hearing protection, Casani et al 7 found that the hearing recovery in the intratympanic corticosteroid group was better than that in the gentamicin group.
A substantial body of research indicates that intratympanic corticosteroids therapy exhibits good tolerability with low incidence of side effects and complications, with the most common complications being postoperative otitis media and tympanic membrane perforation. There are variations in intratympanic corticosteroids treatment regimens, with methylprednisolone and dexamethasone being commonly used medications, but they exhibit different pharmacokinetics. 23 Methylprednisolone is more likely to penetrate the round window membrane and achieve higher concentrations in the inner ear lymphatics, whereas dexamethasone is more readily absorbed by the cochlear epithelium and surrounding tissues. Currently, there is a lack of high-quality literature comparing the efficacy of these 2 agents, as well as the optimal treatment frequency, interval, and follow-up time for vertigo control. We compared the control effects of ITM and ITD on vertigo during the follow-up time. By the 12th month of follow-up, ITD had the highest peak SUCRA of 51.7. As time progressed, the SUCRA value decreased, indicating that the control effect of vertigo with ITD does not increase with time but rather diminishes after reaching its peak efficacy. On the other hand, ITM showed fluctuations in controlling vertigo in the first 12 months, with the highest SUCRA value of 68.9 observed at the 24th month.
In our meta-analysis, gentamicin was found to be more effective than corticosteroids in controlling vertigo. However, its use is limited in patients with good hearing thresholds due to the potential risk of hearing loss after treatment. The certainty of evidence regarding hearing outcomes is very low. Analysis of the mean difference in PTA reported before and after follow-up revealed minimal differences among patients receiving ITG, corticosteroids, or placebo, with no significant inconsistency between studies (χ2 > 0.05). However, for the meta-analysis assessing hearing improvement, the CIs for effect sizes were very wide, with results not reaching statistical significance. This indicates uncertainty regarding whether the intervention is beneficial or harmful, further affecting the quality of evidence.
Intratympanic injection of methylprednisolone and gentamicin in the middle ear have similar effects on long-term control of vertigo. Although the exact mechanism of ITM therapy for MD is not yet clear, some studies suggest that corticosteroids enter the inner ear and bind to their own receptors. These receptors are mainly distributed in the spiral ligament of the human inner ear, followed by the stria vascularis and the modiolus. These drugs have effects such as ion homeostasis, immune suppression, and free radical scavenging, which can be used for cochlear protection, especially in the use of ototoxic drugs and noise-induced damage. These findings indicate that the good efficacy of ITM therapy for vertigo may be related to ion homeostasis and the fluid regulation mechanism of steroids. In addition, steroids can alleviate symptoms related to endolymphatic hydrops by regulating the expression of water channel proteins. Recent articles have shown that in refractory MD cases, a combination of ITG and dexamethasone (ITG + D) is more effective in controlling vertigo than using dexamethasone or gentamicin alone.24,25 Two years after treatment, the vertigo control in the combination group (ITG + D) was superior to that in the single ITD group, providing a potential direction for future research.
The heterogeneity in the severity of baseline diseases and the lack of data correlating with severity prevent us from further exploring the role of MD severity in intratympanic injection therapy. In addition, we did not identify confounding effects of other patient characteristics. Our meta-analysis has other limitations, such as the inability to assess clinical information like middle ear conditions or genetic susceptibility from published literature, suggesting a need for more research to address these gaps. In conclusion, based on the best available evidence in the existing literature, this systematic review found that both ITG and intratympanic corticosteroid injections are effective in treating vertigo and tinnitus caused by MD. However, only dexamethasone showed minimal effect on treating hearing loss, while the evidence for methylprednisolone’s effect on hearing loss was inconclusive.
Conclusion
Intratympanic injection of gentamicin and corticosteroids is an effective method for controlling symptoms of MD. Compared to gentamicin, corticosteroids show better hearing protection effects. Considering that ITG has good effects on controlling vertigo, but high cumulative dose and short injection interval are not conducive to hearing protection. To achieve both hearing and vertigo control, corticosteroids may be the best treatment option in drug intervention measures. Because of the limitations of the small sample sizes, our findings imply the need for future large-scale RCTs to support or refute the findings of the current network meta-analysis.
Footnotes
Acknowledgements
We would like to thank the authors of the included studies for supporting this work.
Data Availability Statement
Authentic and usable data sources. The authors will supply the relevant data in response to reasonable requests.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Compliance with ethical standards. These studies involve a reanalysis of published articles and do not involve additional human subjects.