
Abstract
Laryngocele, an abnormal dilation of the appendix of the laryngeal ventricle filled with air, is a rare condition predominantly presenting unilaterally. However, bilateral occurrences are exceedingly rare. In this article, we present a case of bilateral laryngocele along with a comprehensive literature review. A 57-year-old male presented with dyspnea, stridor, and bilateral neck masses. His medical history included chronic cough and intermittent hoarseness. Over a 3 month period, the neck masses progressively enlarged, resulting in respiratory distress. Interestingly, he denied experiencing weight loss, decreased appetite, or fever. Clinical examination revealed sizable, soft masses on both sides of the neck, obstructing lymph node assessment. Computed tomography (CT) imaging confirmed the presence of a left combined laryngopyocele and a right combined laryngocele. Subsequently, the patient underwent tracheostomy. Benign biopsy results excluded malignancy. Surgical excision of bilateral laryngoceles resulted in an uneventful recovery. The term “laryngocele” was introduced by Virchow in 1867 to describe the abnormal dilation of the saccule associated with Morgagni’s ventricle. Diagnosis involves a thorough patient history, physical examination, and radiological imaging, notably CT, to differentiate laryngoceles from other conditions. Typically asymptomatic, they are often incidentally discovered around age 50, although symptoms such as voice changes or breathing difficulties can manifest. A review of the literature identified 77 documented cases, primarily in males, exhibiting various symptoms and treatment modalities. This case underscores the rarity of bilateral combined laryngocele, emphasizing the importance of timely diagnosis and surgical intervention for favorable outcomes. Comprehensive research reveals diverse clinical aspects, highlighting the necessity for continued investigation to enhance management strategies.
Introduction
Laryngocele, characterized by the dilation of the appendix of the laryngeal ventricle filled with air, establishes a connection with the laryngeal lumen. 1 This condition encompasses 3 distinct types: external, internal, and combined. External laryngoceles manifest as a protrusion of the laryngocele sac through the thyrohyoid membrane, appearing as a neck mass. Conversely, internal laryngoceles confine their sac within the thyroid cartilage, a less common presentation. Combined laryngoceles exhibit both internal and external components. 1 When infected, a laryngocele is termed a laryngopyocele, with an incidence rate ranging from 5% to 8%. 2 The genesis of a laryngocele is hypothesized to result from increased transglottic air pressure, often observed in activities such as trumpet playing, glassblowing, or weightlifting. Clinical presentation typically includes symptoms such as hoarseness, coughing, and, in cases of significant enlargement, airway obstruction. External laryngoceles present as a reducible neck swelling, exacerbated during coughing or the Valsalva maneuver. 1 Diagnosis is typically achieved through indirect laryngoscopy and lateral neck views during the Valsalva maneuver, with computed tomography (CT) scans aiding in lesion extent determination. 1 Surgical excision via an external neck incision represents the primary treatment modality. 2 While marsupialization of internal laryngoceles can be performed endoscopically, recurrence remains a concern. 3 In adults, the presence of a laryngocele may raise suspicions of associated carcinoma, leading to saccule obstruction. 1
Despite its rarity, laryngoceles predominantly present unilaterally, with isolated cases of bilateral occurrences reported. This report details a case of bilateral combined laryngopyocele, including a laryngopyocele, accompanied by a comprehensive literature review.
Case Presentation
A 57-year-old male presented to the otolaryngology emergency department with dyspnea, stridor, and bilateral neck masses. His medical history included a chronic cough with intermittent hoarseness. The neck masses began 3 months ago, progressively enlarging with worsening respiratory distress. He denied weight loss, decreased appetite, or fever. Clinical examination revealed large, soft, compressible masses on both sides of the neck, hindering assessment of the lymph nodes. CT scan showed a left combined laryngopyocele and right combined laryngocele (Figure 1). Tracheostomy was performed, followed by aspiration of 45 cc of purulent material from the left mass for culture and sensitivity analysis. Laryngoscopic examination under general anesthesia revealed bilateral ventricular expansion with normal mucosal appearance. Precautionary biopsies yielded benign results. Surgical excision of bilateral laryngoceles was performed transcervically and endoscopically (Figure 2). The patient recovered well and was discharged on the fifth day. Closure of the tracheostomy and 1 month follow-up showed no recurrence. Long-term surveillance every 6 months was recommended.
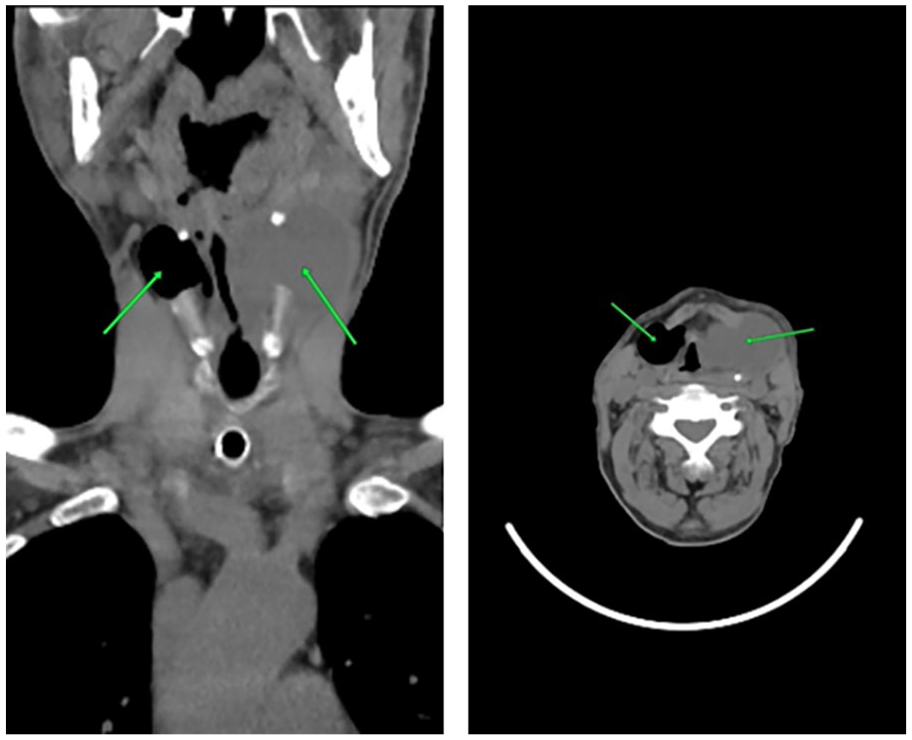
CT scan, coronal and axial plane, showing combined laryngopyocele on the left and combined laryngocele on the right. CT, computed tomography.
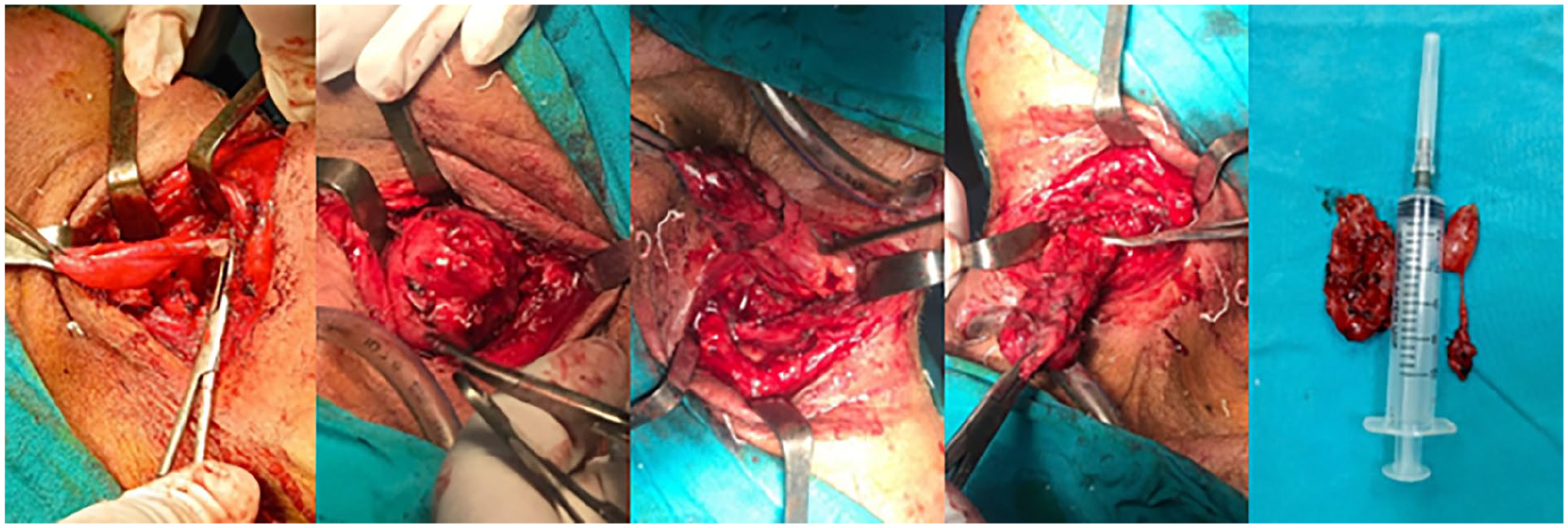
View during and after laryngocoeles resection.
Surgical technique: The surgical procedure commenced with microsuspension laryngoscopy, involving bilateral vocal cord striping to excise redundant and sagging mucosa of the ventricular fold while preserving the anterior commissure and adjacent vocal cord mucosa to prevent synechia. Subsequently, a transverse cervical incision was made in a cervical crease, followed by subplatysmal elevation of superior and inferior cutaneous flaps. A meticulous dissection along the wall of the pyocele was performed, with identification and ligation of the superior laryngeal pedicle including the vein and artery. Preservation of the interior branch of the superior laryngeal nerve was ensured. The posterior limit of dissection extended to the level of the lateral thyrohyoid ligament, which was also conserved. The peduncle of the pyocele was ligated and transected with reversed borders. Closure of the thyrohyoid foramen was achieved with a buried suture. Muscular closure was performed with multiple separate sutures, and a z drainage was fixed with multilayer suture of the surgical incision.
Discussion
In 1867, Virchow introduced the term “laryngocele” to describe the anomalous enlargement of the saccule associated with Morgagni’s ventricle, maintaining continuity with the laryngeal cavity. 1 Diagnosis typically involves patient history, physical examination, and radiological imaging, notably CT scan. Radiological modalities play a pivotal role in distinguishing laryngoceles from other entities such as thyroglossal duct cysts, branchial cleft cysts, cystic hygromas, and tracheoceles. 4 In our case, bilateral laryngoceles were identified preoperatively via CT imaging. Laryngoceles commonly remain asymptomatic and are frequently detected incidentally in individuals around their fifth decade. Symptomatic presentations may include voice alterations, respiratory distress, or throat discomfort. 4
Our literature review revealed 77 documented cases of bilateral laryngocele, encompassing the case discussed herein. Among these cases, age data were available for 41 instances, spanning from 16 to 87 years, with a mean age of 48 years. Age information was unavailable for 36 cases, predominantly due to their inclusion in broader studies where individual patient details were not recorded (Table 1).4-57
Summary of All Cases of Bilateral Laryngocele.
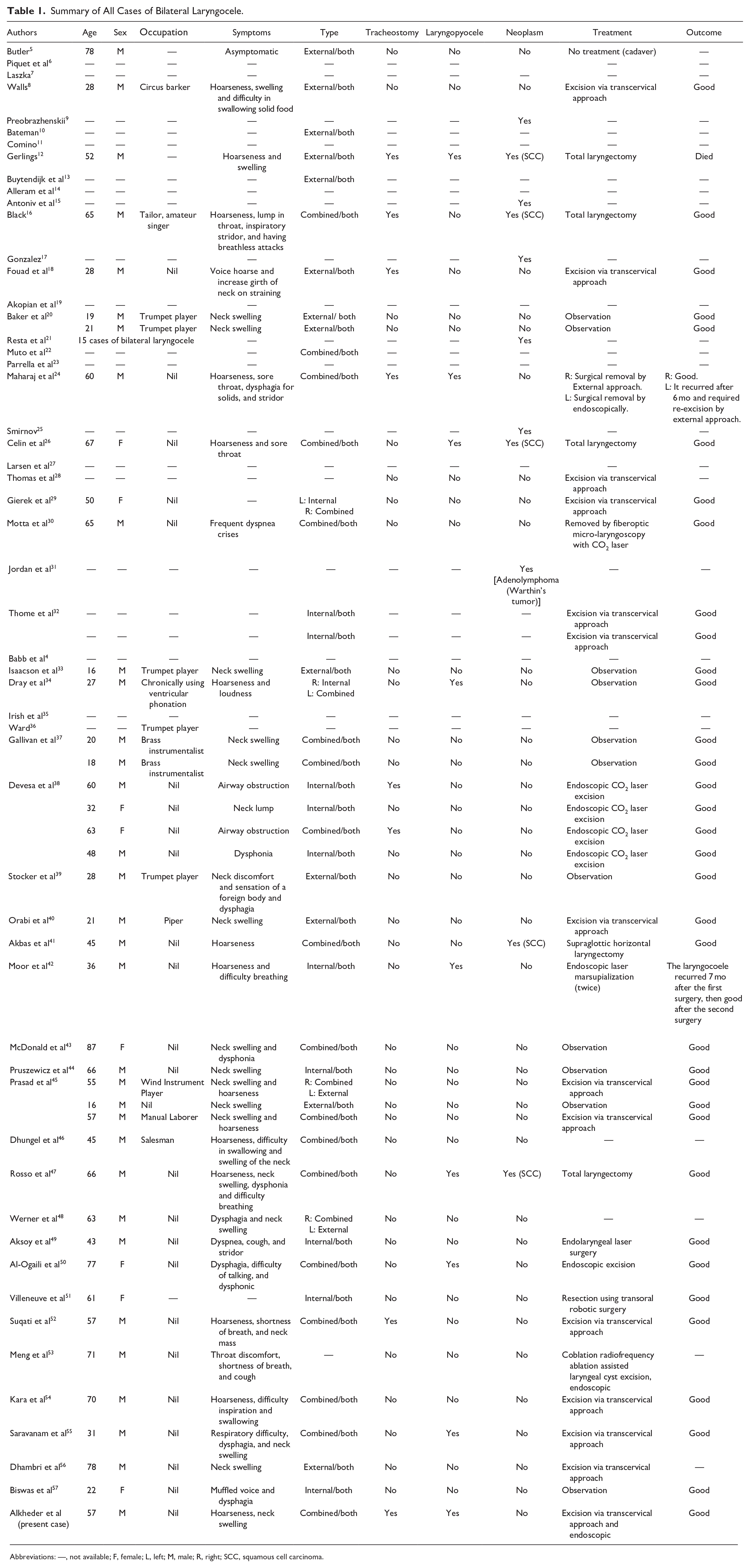
Abbreviations: —, not available; F, female; L, left; M, male; R, right; SCC, squamous cell carcinoma.
Bilateral laryngocele exhibited a higher incidence among males, with 33 cases documented in males compared to 8 in females, while data regarding gender were not available for 36 cases. Among the reported cases, 14 were associated with wind instrument players or chronic voice misuse, whereas 25 cases showed no such association, with information missing for 38 cases (Table 1).4-57
The clinical presentation was varied, encompassing symptoms such as hoarseness, neck swelling, dysphagia, stridor, breathlessness, voice hoarseness, sore throat, dyspnea, dysphonia, sensation of a foreign body, cough, and muffled voice. Neck swelling predominated as the primary manifestation in 25 cases, followed by hoarseness in 15 cases, while one case was asymptomatic and detected incidentally during autopsy (Table 1).4-57
The predominant subtype was combined, observed either unilaterally or bilaterally in 22 cases, followed by the external type seen in 15 cases, and the internal type observed in 12 cases, with subtype data missing for 32 cases (Table 1).4-57
Tracheostomy was necessitated in 8 patients, while 34 patients did not require the procedure, and data regarding tracheostomy status were not available for 35 cases. Laryngopyocele was present unilaterally or bilaterally in 9 out of 42 reported cases, while information regarding laryngopyocele was not reported in 35 cases (Table 1).4-57
Eight patients underwent tracheostomy, comprising 7 males and 1 female, while 34 patients, consisting of 27 males and 7 females, did not necessitate tracheostomy, indicating no significant association between gender and tracheostomy requirement in bilateral laryngocele patients (P > .05; (Table 1).4-57
Bilateral laryngocele was linked with neoplasms in 25 cases, predominantly squamous cell carcinoma (SCC), except for 1 case of adenolymphoma (Warthin’s tumor), while 37 cases showed no neoplastic association, and data regarding neoplastic involvement were unavailable for 15 cases. In addition, 1 case of laryngocele developed following acute neck trauma (Table 1).4-57
Among the studies reporting the association of bilateral laryngocele with SCC, only 5 studies provided gender-specific data, revealing 4 males and 1 female with SCC compared to 37 cases (30 males and 7 females) without SCC, these findings suggest no significant association between SCC and gender (P > .05). In addition, based on the available data, there was no significant association between tracheostomy and neoplasms, as only 2 patients with SCC required tracheostomy (P > .05; Table 1).4-57
Laryngopyocele was documented in 9 out of 42 studies, while tracheostomy was required in 8 out of 42 patients. Among the cohort, 28 patients did not undergo tracheostomy and did not exhibit laryngopyocele, indicating no significant association between tracheostomy and laryngopyocele (P > .05). None of the studies reported the presence of fever in association with laryngopyocele (Table 1).4-57
Three patients presented with both laryngopyocele and SCC, suggesting a potential association (P = .057) and making total laryngectomy the appropriate treatment for these cases with a good outcome (Table 1).4-57
Among the 42 studies analyzed, various treatment modalities were identified. The most prevalent intervention was the external transcervical approach, utilized in 14 cases. Endoscopic excision was performed in 1 patient. In addition, 2 patients underwent excision using a combination of external and endoscopic approaches. Seven patients underwent laryngocele excision via endoscopic laser (CO2), while 1 patient underwent excision using transoral robotic surgery. Another patient underwent excision utilizing radiofrequency endoscopy. Four patients underwent total laryngectomy, and 1 patient underwent supraglottic horizontal laryngectomy as part of the treatment for associated malignancy. Eleven patients were placed under observation, while 1 case was incidentally discovered during autopsy without intervention. Furthermore, details regarding treatment were not provided for 35 cases (Table 1).4-57
All patients who underwent excision via the external approach achieved favorable outcomes without recurrence. However, 1 patient from the cohort undergoing endoscopic excision experienced recurrence after 6 months, necessitating re-excision via the external approach. Similarly, 1 patient among those treated with laser excision encountered recurrence after 7 months and underwent retreatment utilizing laser therapy. Notably, all 11 patients placed under observation exhibited laryngocele regression and symptom improvement. One patient died, who had accompanying SCC in the larynx and had undergone total laryngectomy (Table 1).4-57
Our observations indicate that bilateral laryngocele correlated with malignancy in elderly patients, while it manifested as a benign condition in younger patients. Notably, all 9 young patients, with an average age of 20.7 years, did not require treatment (Table 1).4-57
Conclusion
In conclusion, this case report highlights the rare occurrence of bilateral combined laryngocele, emphasizing the importance of prompt diagnosis and appropriate management in such cases. Surgical intervention, primarily through transcervical excision, remains the cornerstone of treatment, with favorable outcomes observed in most cases. Furthermore, our comprehensive literature review underscores the varied clinical presentations and associations of bilateral laryngoceles, shedding light on factors such as age, gender, symptomatology, and treatment modalities. Continued vigilance and further research are warranted to enhance our understanding and management of this uncommon condition.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.