
Abstract

Significance Statement
This case report highlights a rare presentation of monkeypox, initially manifesting as tonsillitis in an immunocompetent patient. Such atypical symptoms can lead to misdiagnosis, underscoring the need for clinicians to consider monkeypox as a differential diagnosis even in immunocompetent individuals with common presentations like tonsillitis. This insight is crucial for timely and accurate diagnosis and treatment in the context of the ongoing global monkeypox outbreak.
Monkeypox infection has been progressively emerging worldwide since May 2022. Tonsillitis is a common disease in the field of otolaryngology, but diagnosing monkeypox infection through the subsequent appearance of rashes in the body can be quite challenging. In this article, we describe a rare case of monkeypox infection in a 38-year-old immunocompetent male who first presented solely acute suppurative tonsillitis, highlighting its clinical characteristics, diagnostic difficulties, and treatment.
A 38-year-old man with underlying hepatitis B disease initially visited the local clinic for a 5 day sore throat. Acute suppurative tonsillitis was first diagnosed and a 5 day course of oral amoxicillin was administered. The patient came to our outpatient otorhinolaryngology department due to a persistent symptom. Laryngoscopy revealed bilateral tonsil enlargement with white ulcerative lesions and diffuse swelling with erythematous change in oropharynx (Figure 1). We arrange admission for intravenous amoxicillin/clavulanic acid and analgesic treatment. On the 11th day after the appearance of the sore throat, he developed fever, multiple non-itchy reddish papules and pustules on the scalp, face, trunk, and 4 limbs (Figure 2). After careful history collection, monkeypox infection could not be completely ruled out because he had unprotected sexual contact with other males in the Philippines 2 weeks before the sore throat. Real-time polymerase chain reaction testing of samples, including those from auricle pustules, throat swabs, and abdominal vesicle swabs, all confirmed a positive diagnosis of monkeypox. For monkeypox infection, we only provided symptomatic treatment and isolation. No new papules were present after 3 days. White ulcerative lesions on the bilateral tonsils also subsided after 5 days. During subsequent outpatient follow-up, there were no sore throat, fever, or new skin lesions.
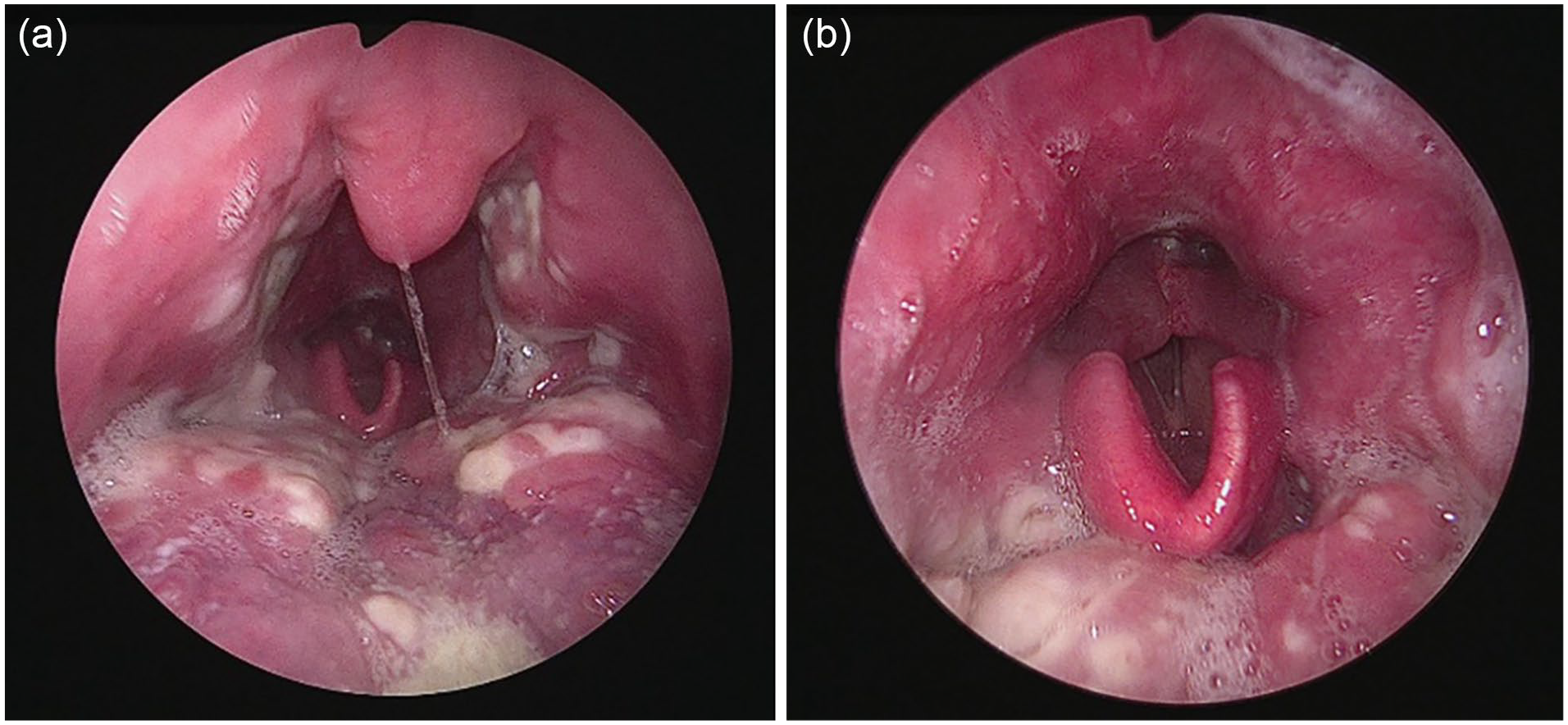
Laryngoscopy showed (A) bilateral tonsils enlargement with white ulcerative lesions and (B) oropharyngeal swelling with erythematous change.

Papules on the back.
The most reported clinical features of monkeypox included skin lesions (95%), fever (62%), or lymphadenopathy (56%). 1 The proportion of initial presentations with oropharyngeal symptoms, including sore throat, pharyngitis, odynophagia, epiglottitis, and oral or tonsillar lesions, was only around 5%.1,2 Monkeypox presenting solely as acute tonsillitis at the beginning is rare, and the solitary occurrence of tonsillitis in immunocompetent individuals with monkeypox is extremely rare. Few articles in the literature report on monkeypox infection with acute tonsillitis as the initial manifestation, and all patients are coinfected with human immunodeficiency virus (HIV), regardless of whether they received antiretroviral therapy or not.3-5 Those without HIV infection are less likely to have tonsillitis than those with HIV. 6 In our case, the patient is neither HIV positive nor immunosuppressed, so exclusively tonsillar signs were not previously known to be a typical feature of monkeypox infection. At initial presentation, throat features included ulcers, pain, secondary bacterial superinfection, and quinsy, which could all be mistaken for bacterial tonsillitis. Infection in patients presenting in such ways may have gone undiagnosed in the community for some time. This could help explain why the outbreak had become so widespread at the point of detection.
Monkeypox infections are commonly seen in men (97%-99%), with a particular prevalence among homosexual or bisexual men (95%-98%).1,7,8 The average age is about 38 years old.1,9 The median incubation period was 7 days.1,7 HIV disease was present in about 40% of cases with monkeypox infection.1,2,7 Among the multitude of symptoms and signs, diarrhea, fever, and genital or perianal lesions were statistically significantly more prevalent among HIV patients compared to non-HIV patients in a global cross-sectional study. 2 There were no significant differences in the overall incidence of a sore throat, diagnosed as pharyngitis, between patients with (29%) or without HIV infection (20%). 2 In terms of treatment and prognosis, no significant differences were observed in the proportion of patients who needed antiviral therapy, hospitalization due to the severity of the disease, and the outcome of the disease when comparing the 2 groups. 2
The treatment of monkeypox involves supportive care, isolation of infected individuals, and in some cases antiviral therapy. Most of the cases were mild and self-limited.1,6 However, some more severe cases may require hospitalization for airway management and steroid treatment due to airway compromise caused by acute tonsillitis. 3 This case leads to the conclusion that monkeypox infection is a disease with a relatively good prognosis and is a reminder to clinical physicians to be vigilant about history taking and differential diagnosis, especially in the immunocompetent patient.
Monkeypox that presents with papules following the symptoms of acute tonsillitis can easily lead to misdiagnosis. Such a diagnosis is rare in the absence of immunosuppressed conditions. This case highlights the diagnostic challenges associated with monkeypox infection, particularly when it occurs outside endemic regions. Early recognition and diagnosis of this disease are crucial for effective management and epidemiological control.
Footnotes
Author Contributions
C.W.H.: data curation, formal analysis, writing—original draft. J.Y.L.: visualization. S.C.L.: methodology, conceptualization, supervision, writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This case report, which does not contain identifiable private information, was granted a waiver of informed consent by the Institutional Review Board (IRB) at our institute.