
Abstract
Introduction
Dysphonia persisting for over a week affects 1 in 13 adults in the United States annually, imposing a significant burden and influencing overall quality of life.1,2 Voice therapy (VT) is the cornerstone of treatment for dysphonia secondary to common laryngeal pathology such as muscle tension dysphonia, presbylarynx, and vocal fold nodules. Typically, VT is administered over a period of weeks to months, and patients participate in person. 3
Historically, technological advances have been utilized to improve access to healthcare in rural and underserved areas. 4 With the advent of the telephone in the late 1800s, a group of doctors utilized a drugstore line to provide access to care for remote patients. 5 The “radio doctor” provided the first live consultation in 1927. 4 In the 1950s, recorded videos were transmitted via satellites to provide care for inhabitants of rural Alaskan villages. 6 The National Aeronautics and Space Administration (NASA) made some significant advances in telemedicine in the 1960s to meet the needs of astronauts. 7 Historically, cost and insurance coverage have been the major obstacles inhibiting the use of telemedicine. 8 The federal government swiftly made several modifications such as Health Insurance Portability and Accountability Act (HIPAA) flexibility, expansion of Medicaid and Medicare policies, and increased licensure flexibility to allow for broad access to telemedicine during the COVID pandemic. These changes resulted in broader adoption of telemedicine across various medical specialties, prompting many healthcare professionals to shift some or all of their practices to telemedicine. There are numerous benefits to telemedicine, such as reduced or eliminated transportation needs, increased flexibility in scheduling, increased access, and decreased financial burden. 9
In otolaryngology and allied health professions such as speech language pathology (SLP), the COVID-19 pandemic presented unique challenges due to restrictions on social contact and aerosolizing procedures. Our institution rapidly integrated telemedicine to allow us to continue to serve as many patients as possible, which was later integrated into daily practice following the ending of COVID-related restrictions. The aim of this study was to assess whether the telemedicine platform could improve completion rates for VT compared to traditional in-person sessions. In addition, we wanted to explore the demographic factors that are associated with completion of VT, including the impact of the Area Deprivation Index (ADI) score on VT participation and investigate whether telemedicine increases participation for patients in more disadvantaged geographic areas.
Methods
Patient Selection
Institutional Review Board (IRB) approval was obtained from the University of Arkansas for Medical Sciences (UAMS) IRB (IRB #273962). Retrospective review of electronic medical records was performed to identify patients who were referred to VT. All patients who were referred to VT were included in the study. Exclusion criteria comprised individuals who did not enroll in a VT session at UAMS and patients with incomplete charts. The data collected included the following variables: age, sex, race, ethnicity, marital status, employment status, payer status, Voice Handicap Index (VHI) scores, completion status of VT, number of therapy sessions attended, distance traveled to attend VT, and the time required to reach VT. Zip codes were utilized to determine ADI scores (0-100). When interpreting this scale, a higher score refers to an individual who resides in a more disadvantaged neighborhood.
The study cohort was divided into 2 subgroups: patients who underwent in-person VT and patients who opted for telemedicine VT. All patients were offered both options, as long their insurance covered the recommended method. All patients receive VT from the same 2 speech language pathologists (H.P. and H.P.). The determination whether a patient had completed VT and reached goals was made by the SLP, and data regarding patients’ therapy status were extracted from the charts by 2 different reviewers (M.C.B. and N.A.). The last VT note contains the session number, whether or not the recommended therapy was completed, and to what degree the patient was able to complete his or her VT.
Technical Setup and Session Protocol
To ensure transparency and replicability of the telemedicine setup, the research team utilized desktop computers featuring 64-bit processors running Windows 10. These computers were equipped with external webcams, microphones, and speakers to facilitate effective teletherapy sessions. Teletherapy services were delivered through either the Epic platform or the HIPAA-compliant website https://doxy.me. Notably, the internet connection speed was 1000 Mbps, ensuring undisrupted communication during sessions. Weekly sessions were scheduled for 45 minutes, typically lasting from 30 to 45 minutes over a span of 3 to 12 weeks, contingent on the severity of the disorder and patient progression. Leveraging the Doxy.me platform via the Google Chrome browser ensured compliance with HIPAA regulations while addressing connectivity issues.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics v29.0 (IBM Corp). Mean, standard deviation (SD), minimum, and maximum were calculated for continuous variables. Chi-square analysis was used for comparison of categorical variables, with use of Fisher’s exact test in cases of low numbers. T test and Analysis of Variance (ANOVA) were utilized for comparison of continuous variables. A P value ≤ .05 was considered statistically significant.
Results
A total of 521 patients were referred to VT at our institution between 2019 and 2021. Out of the total 521 patients, 259 were excluded from the study due to incomplete records or not initiating VT. Among patients initiating VT sessions, 76 (29%) chose telemedicine VT (TVT) sessions, while 186 (71%) opted for in-person sessions. The demographic distribution among the patients consisted of 78 males (26%) and 219 females (74%), with a mean age of 57.1 years (range: 10-89 years old). No statistically significant differences were observed between these 2 groups in terms of sex (P = .892), age (P = .173), employment status (P = .656), national ADI score (P = .470), and state ADI score (P = .466). Though not statistically significant, employed patients showed a higher preference for TVT compared to retired patients (26% vs 23%). Single patients demonstrated greater inclination toward TVT (26%) than married patients (22%), and female patients exhibited higher preference for TVT compared to male patients (26% vs 21%). There were no significant disparities in the type of insurance in either group (P = .838; Table 1).
Demographic Variables for Subgroups and Total Cohort.
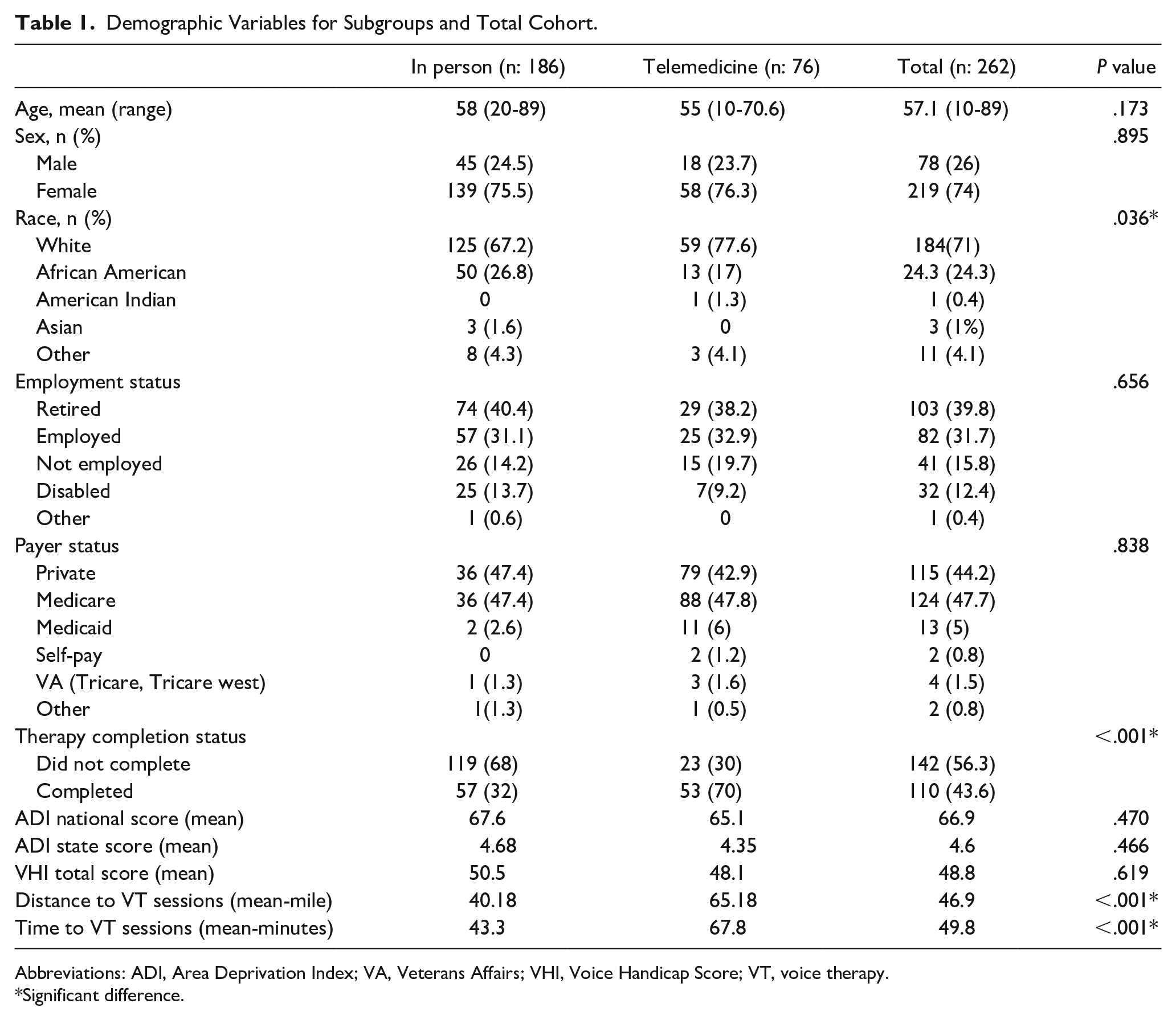
Abbreviations: ADI, Area Deprivation Index; VA, Veterans Affairs; VHI, Voice Handicap Score; VT, voice therapy.
Significant difference.
Participants in the TVT group exhibited significantly higher completion rates (70.0% vs 31.6%; P < .001). A significant difference in race was observed between the 2 groups, with the telemedicine group having a higher percentage of white patients compared to the in-person group (77.6% vs 67.2%, P = .036). Patients in the telemedicine group reported on average residing farther away and requiring longer travel time to reach in-person VT (65.1 vs 40.1 miles, P < .001; 67.8 vs 43.3 minutes, P < .001; Table 1).
The average National ADI percentile for all patients in the study stood at 66.92% (SD: 22.13; Figure 1). Moreover, 64% of patients (n: 189) had an ADI score above 50%, while only 36% (n: 63) had a score below 50%. Meanwhile, the average National ADI total score was 65.1% (range: 9%-98%) for the Telemedicine VT group compared to 67.6% (range: 9%-100%) for the in-person VT group (P = .470), while the average state ADI percentile score was 4.35 (range: 1-10) in the Telemedicine VT group and 4.68 (range: 1-10) in the in-person group (P = .468). Of note, the average national ADI score for those who completed VT was 63.3 (range: 9-100), versus 68.4 (range: 9-100) for those who did not (P = .085). The average state ADI score for those who completed VT was 4.1 (range: 1-9), versus 4.7 (range: 1-10) for those who did not (P = .086). The average total pretreatment VHI score was 48 (range: 40.6-55.6) for the TVT group and 50.5 (range: 45.4-55.6) for the in-person VT group (P = .619), with no significant difference between those who completed VT and those who did not (47.8 vs 50.7, P = .501) noted.
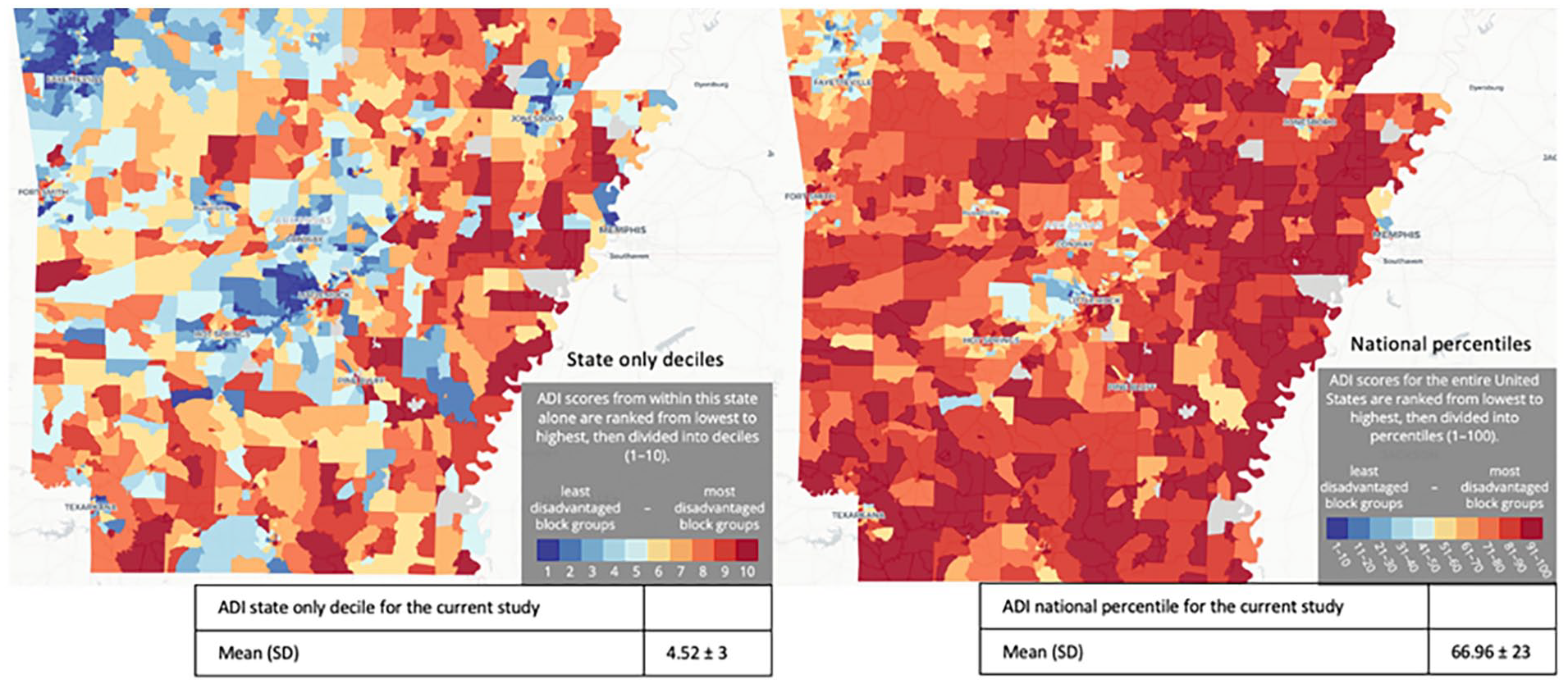
National and state ADI score distribution of the patients residing in the state of Arkansas 22 and patients included in the study. ADI, Area Deprivation Index.
Discussion
Telemedicine has increasingly been recognized as a valuable tool across various medical disciplines, offering the potential for long-term integration into healthcare practices.9-12 The integration of telemedicine has been particularly accelerated by the COVID-19 pandemic, which necessitated physical distancing and highlighted the importance of remote healthcare services. Telemedicine spans a wide array of applications, ranging from primary care consultations to psychotherapy and physical therapy, leveraging technologies like video conferencing, smartphones, and other wireless devices. 13
VT involves an initial assessment and a series of treatment sessions. The adoption of telemedicine for VT brings unique challenges, as it heavily relies on accurately assessing voice quality, which may be affected by the limitations of teleconferencing platforms. 14 Despite these challenges, telemedicine has shown promise in delivering effective voice treatment for various pathologies. Studies have demonstrated that telemedicine can be as effective as in-person sessions for VT, with no significant differences in outcome measures such as voice quality and patient satisfaction.11,15-17
Access to healthcare in rural and underserved areas has become an increasingly important subject. 18 Such populations often encounter significant challenges consistently accessing medical care and ancillary services due to factors such as increased travel time, lack of scheduling flexibility, and financial constraints. 19 For patients needing VT, telemedicine could broaden access to care and alleviate some financial burden, potentially resulting in higher treatment completion rates. Dawkins et al performed a systematic review that examined factors contributing to healthcare inaccessibility across the globe. 18 Some of the commonly cited factors include demographics, finances, facilitators, sociocultural factors, patient factors (such as perceived need), treatment/service concerns, transportation barriers, and geographic factors. 18
A growing body of literature suggests an association between residing in a disadvantaged neighborhood (characterized by higher ADI scores, lower socioeconomic status, and increased distance from hospital centers) and health outcomes.20-23 Moreover, it has been proposed that individuals from underprivileged areas are more likely to rely on telemedicine visits compared to those from the least disadvantaged category. 24 Among our patients, no significant difference was found between national or state ADI scores and VT method preference (P = .470). One potential explanation for the absence of significant differences between national ADI scores and VT delivery method preference could be our university hospital system’s efforts to mitigate disparities across socioeconomic and geographic contexts. Such efforts include accepting all forms of insurance and providing financial aid to patients, which likely enables patients to pursue in-person therapy.
A significant number of patients who were provided with telemedicine options to alleviate the financial strain of travel expenses and time off work may not possess the necessary tools for telemedicine access, or they might face challenges in navigating the virtual platform. In this study, we did not call patients to ask if they had access to a computer, internet, or smartphone, nor did we assess their health literacy; further studies are needed to evaluate these factors. Patients were provided with both treatment options so that if they had no access to requisite electronic platforms, they could still select in-person sessions. This may be one of the factors affecting completion rates.
Until the COVID-19 pandemic, one of the main barriers to telemedicine therapies has been reimbursement by insurance companies. Our results clearly demonstrate that telemedicine enables improved completion rates compared to traditional in-person VT [70.0% vs 31.6% (P < .001)]. Thus, we suggest the medical community should focus on improving access to telehealth services. Our institution has access to a multitude of Area Health Education Centers dispersed throughout the state, more commonly used to deliver primary care services. Such clinics could be leveraged to provide VT access to patients without computer or internet services. Similar initiatives for improving access to healthcare through telemedicine are being undertaken by the Veterans Health Administration.
The VHI is a widely used patient-reported outcomes measure in laryngology, assessing the impact of voice disorders on patients’ quality of life through a subjective self-assessment of the voice. 25 Similar to this study’s findings among the Arkansan population, Labarge et al conducted measurements comparing VHI scores between in-person clinic and telemedicine platforms and revealed no significant difference. 26
Góes et al, in an observational study analyzing adherence to VT, found no correlation between adherence and gender or previous speech therapy. However, a significant association was observed between the number of sessions attended and age range as well as type of dysphonia. 27 Torbes et al assessed various VT success indicators, including completion of the therapy plan, patient self-report, and the URICA-VOICE scale. They identified several factors as significant contributors to patient VT adherence, including the perceived impact of dysphonia, socioeconomic status, duration of therapy, and the necessity for lifestyle changes. 28
While telemedicine offers numerous advantages, it does come with certain challenges, especially in the field of VT. As highlighted by LaBarge et al, instructing exercises through virtual platforms presents difficulties, particularly when physical techniques like manual circum-laryngeal massage cannot be directly demonstrated on the patient. 26 However, patients with prior experience in massage techniques reported minimal difficulties in adapting to the virtual format. 26 A team at the Boston University College of Health and Rehabilitation Sciences conducted a study with 29 patients, revealing that teleconferencing platforms face challenges in accurately capturing critical measurements essential for precise and clinically meaningful voice evaluations. 14 Notably, there were pronounced pitch variations observed across all virtual platforms when compared to real-life recordings. 14 These variations were attributed to issues related to internet connection or bandwidth affecting the transmission of sound during virtual assessments. To address these challenges and enhance the versatility of telemedicine, potential solutions exist. Trecca et al reported offering hybrid classes enables individuals to opt for in-person learning of exercises until they feel comfortable and ready for VT. 29 Moreover, Bokolo highlight that a reliable internet connection significantly enhances the quality of telemedicine sessions, leading to increased patient satisfaction and ultimately benefiting clinicians in conducting more effective voice evaluations. 30
Telemedicine presents a spectrum of legal and ethical challenges including issues such as authorization, accreditation, and safeguarding patients’ personal data. These complexities underscore the need for standardization and regulatory processes to ensure ethical practice.31,32 Resources are available to healthcare providers and patients for addressing such challenges. For instance, the Health Resources and Services Administration hosts a website offering legal considerations and best practice guides for telehealth. 31 In addition, the American Medical Association provides a comprehensive Code of Medical Ethics specific to telemedicine practice. 33 Using HIPAA-compliant platforms such as the Epic platform or https://doxy.me (as was done in this study) can enhance patient data security. These measures demonstrate commitment to ethical telemedicine practices and contribute to the ongoing advancement of telehealth services.
Despite its challenges, telemedicine holds potential to address the needs of underserved individuals in remote regions, those unable to access VT in person, and those with time constraints. Our research confirms the capacity of telemedicine to reach patients who may encounter difficulties attending conventional clinic appointments. Furthermore, our research highlights telemedicine’s potential to significantly improve therapy completion rates by offering a more convenient VT alternative.
The integration of VT and telemedicine will likely expand moving forward. 34 Expansion will be fueled by technological advancements, growing familiarity with digital platforms among patients and providers, and ongoing research refining telemedicine standards. 35 Furthermore, regulatory and reimbursement frameworks are poised to better facilitate and endorse telehealth services, playing a pivotal role to ensure the long-term adoption and effectiveness of telemedicine. As telemedicine becomes a standard part of VT, it will be important for training programs to incorporate telehealth competencies, ensuring that new therapists are well equipped to deliver high-quality care both in person and remotely.
Limitations inherent in our study stem from its single-institution, nonrandomized, retrospective chart review design. The retrospective nature of our research implies that our results rely on the availability and accuracy of the collected records, introducing potential sources of bias. The absence of randomization is another limitation, opening the door to the influence of confounding factors. Nevertheless, our study underscores the need for future follow-up investigations to comprehensively assess the multifaceted factors affecting VT session completion rates. Due to its large number of participants, this study provides valuable insights into the significance of telemedicine in the VT setting.
Conclusions
Telemedicine holds significant potential in the setting of VT, particularly in terms of completion rates and expanding access to care. Telemedicine shows promise for delivering treatment as effective as in-person sessions.
Footnotes
Authors’ Note
Meeting Information: Presented at the Triological Society Spring Meeting (COSM), May 2022, Dallas, TX, USA.
Author Contributions
Soroush Farsi: data analysis, manuscript drafting and editing. Mary C. Brown: design, conduct, chart review, manuscript drafting. Nickolas Alsup: design, conduct, chart review, manuscript drafting and editing. Hylan Pickett: chart review, data collection manuscript editing. Hannah Petersen: chart review, data collection manuscript editing. Kyle Davis: design, conduct, chart review, analysis, manuscript drafting. Deanne King: design, analysis of the research, manuscript editing. Ozlem E. Tulunay-Ugur: design, participating surgeon, analysis, manuscript drafting and editing.
Data Availability
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approved by the University of Arkansas for Medical Sciences Institutional Review Board: IRB# 273962
Level of Evidence
Level 4.