
Abstract

Significance Statement
Primary malignant melanoma of the parotid gland is extremely rare. The appearance of T1 hyperintense and T2 hypointense areas on magnetic resonance imaging may suggest malignant melanoma. Histopathological data, clinical examination, and radiological screening are important for differentiation from metastatic lesions. The primary treatment for this tumor, which has a poor prognosis, is surgical resection.
A 73-year-old male patient was admitted to our center with a mass in the left preauricular area, which had increased in size over the past 6 months. The patient, who was receiving medical treatment for atrial fibrillation, had no other known chronic illness, previous surgery, or trauma. Clinical examination revealed a 6 cm × 2 cm hard, mobile mass in the left parotid gland. There were no skin lesions on the face or scalp. Neck examination revealed several hard masses extending along the left cervical chain. Contrast-enhanced magnetic resonance (MR) imaging was performed in the patient; whose laboratory tests were unremarkable. The images showed a 47 × 38 × 46 mm lobulated, contoured, irregularly circumscribed mass lesion located in the superficial lobe of the left parotid gland and extending into the deep lobe. The lesion was heterogeneously hyperintense on T1- and T2-weighted images, showed restriction on diffusion-weighted images and was intensely heterogeneously contrasted. In addition, there were numerous lymphadenopathies at left levels 2, 3, 4, and 5, the largest of which was 22 mm × 19 mm, round in shape, with no discernible hilum and similar signal characteristics to the parotid lesion (Figure 1). Diffuse edematous hyperintensities were observed around these lesions and on the face. A tru-cut biopsy of the mass in the left parotid gland was subsequently performed. HMB45, S100, and SOX10 were diffusely positive on pathological examination and the patient was diagnosed with malignant melanoma (Figure 2). Positron Emission Tomography-computed tomography (PET-CT) scan of the patient showed no lesion other than the parotid mass and lymphadenopathies in the cervical chain. The patient was diagnosed with primary parotid malignant melanoma and surgery was recommended. However, the patient refused and neoadjuvant chemotherapy was administered.
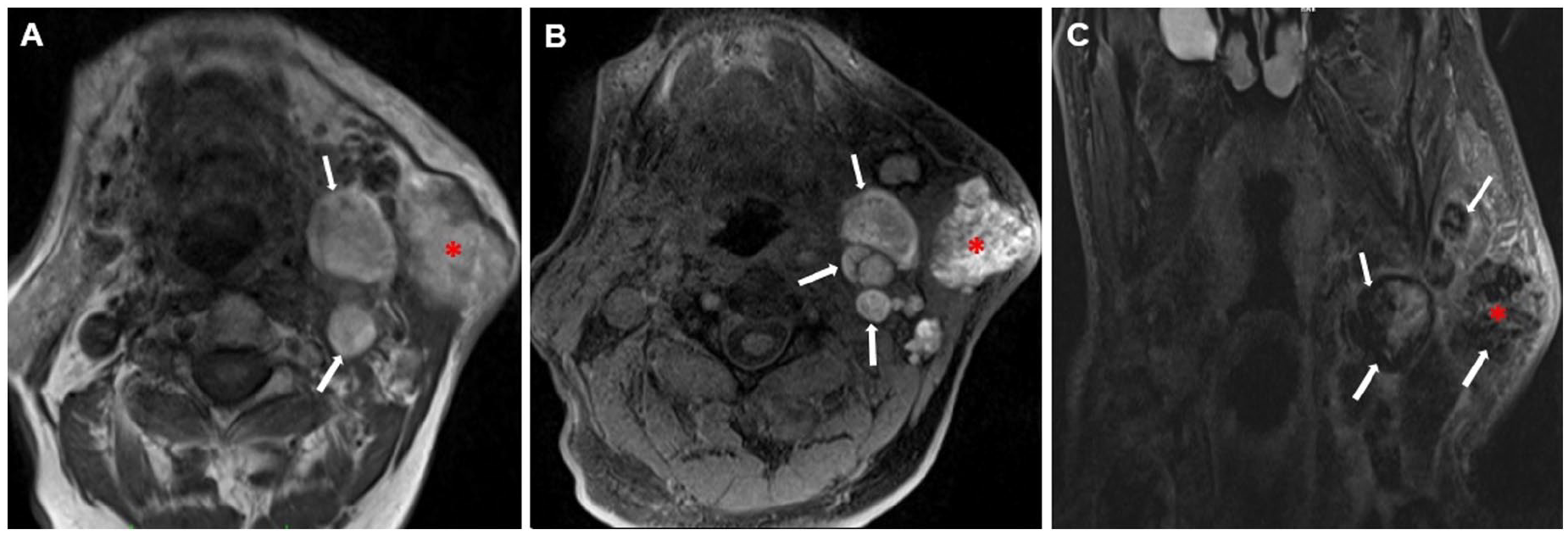
Axial T1-weighted (A) and fat-suppressed T1-weighted (B) images show a hyperintense mass lesion (asterisk) and lymph nodes with similar signal characteristics (arrows). In the T2-weighted coronal section (C), the lesion (asterisk) and lymph nodes (arrows) appear hypointense.
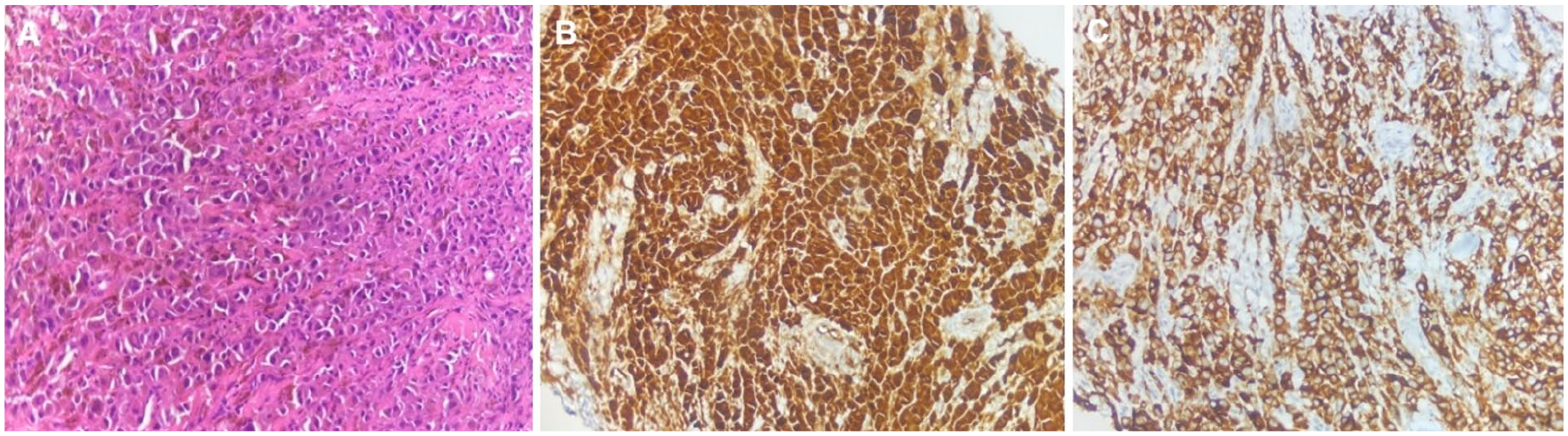
The figure shows histological appearance of malignant melanoma in the parotid gland (H&E ×200) (A), strong nuclear and cytoplasmic reactivity of neoplastic cells for S-100 protein (×200) (B), and immunoreactivity of neoplastic cells for HMB45 (×200) (C). H&E, hematoxylin and eosin.
The parotid gland is an important lymphatic drainage filter in the head and neck, including a large area in the scalp and face. Therefore, most of the parotid malignant melanomas are metastatic. Primary parotid malignant melanoma is very rare and accounts for 0.7% of parotid malignancies. 1 There are different theories about the manifestations of non-primary parotid malignant melanomas. The first one is that 10% to 35% of cutaneous malignant melanomas may regress or even become invisible. In this case, metastasis in parotid lymph nodes may be observed as primary. 2 In addition, melanocytes containing melanin have also been detected in the parotid gland. This shows that malignant melanoma may originate directly from the parotid parenchyma. 3 The diagnosis of primary malignant melanoma of the parotid gland is made under the following conditions: Most of the tumor should be in the parotid gland, the tumor should not involve lymph node tissue, there is no evidence of other malignant melanoma (MM) lesions in the body, and there is no suspicious pigmented lesion or MM excision. Clinically, patients usually have a hard mass in the parotid region that can be fixed to the skin and may be accompanied by facial nerve paralysis.1,4 Radiologically, there are no specific findings on CT, but MR imaging may be helpful. While many parotid gland tumors appear hypointense on T1-weighted images, malignant melanoma lesions may show hyperintense areas due to the hemorrhagic products and melanin they contain. This will also appear as hypointensity on T2-weighted images. 5 Definitive diagnosis is made by histopathology. The prognosis of parotid malignant melanomas is known to be poor. Surgery is the preferred treatment. Postoperative radiation and chemotherapy are questionable.1-4
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.