
Abstract

Kopetzky 1 divides the history of simple mastoidectomy into 2 chronological periods—the experimental (1656-1864) and the modern thereafter. One of the “experimenters” Johann Riolan, in 1649, suggested trepanation of the mastoid bone to treat deafness and tinnitus on theoretical grounds. There is no evidence that he or his contemporaries actually operated on the temporal bone. Jean-Louis Petit is credited with performing the first successful mastoidectomy for suppurative disease in 1736. 2 Petit, the outstanding French surgeon of his day, used a trepan to cut into the mastoid bone (Figure 1). S.F. Morand, a French surgeon educated in England, reported mastoid trepanation to treat what was likely a subdural abscess in 1768. Loeffler and Hagstrom each tried to correct hearing loss by perforating the mastoid. This failed and instead spread infection. 3 Following the death of Baron Berger, the personal physician of the King of Denmark, from meningitis after mastoid perforation, mastoid trepanation fell into disrepute.
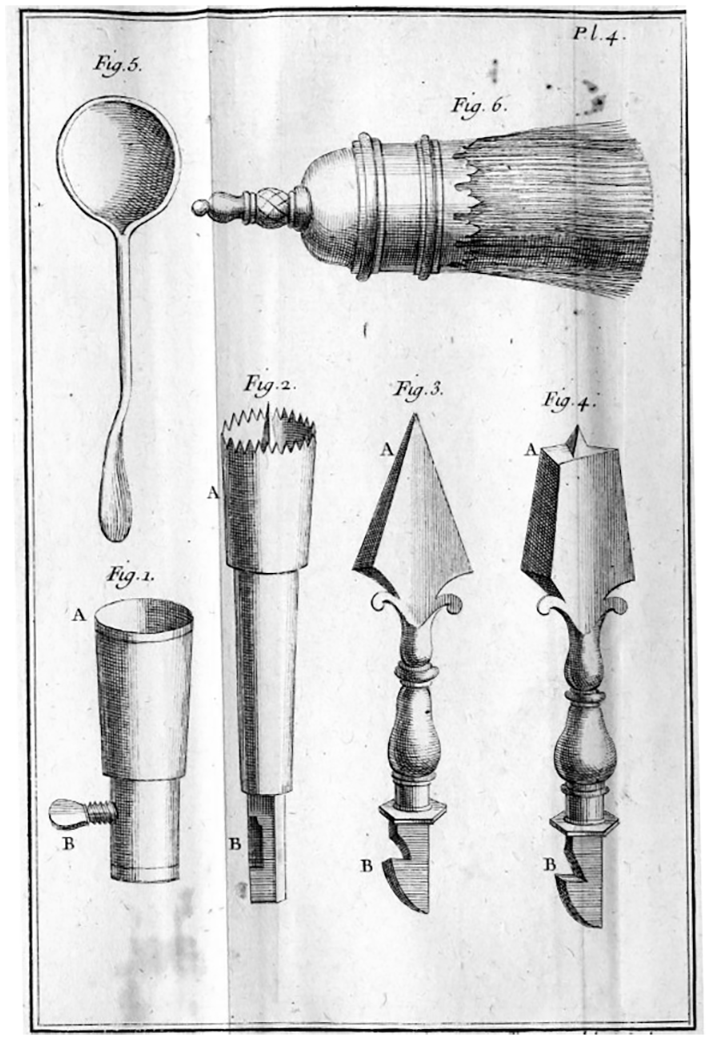
The mastoid trepanation tools of Jean-Louis Petit. 2
Credit for the rebirth of mastoid surgery belongs to Hermann Schwartze and his assistant, Adolf Eysell, who ushered in the modern age of mastoidectomy. They established mastoid surgery on a firm anatomic basis and improved the available instrumentation. In infectious cases, they advocated opening any existing draining fistula with a curette, then enlarging the cortical perforation with a sharp gouge. When the cortex was intact and hard, a curved gouge and mallet were used to remove the cortex. Infected tissue and any sequestrum were then scooped out with a sharp spoon (curette). Schwartze preferred to remove successive shells of bone with the gouge rather than boring in with a trepan or drill. 4 Other surgeons remained concerned about injury to the dura and sigmoid sinus by hammer blows and continued to use a trepan to find the mastoid antrum. As late as 1911, Ballenger 5 advocated boring a hole in the suprameatal triangle with a “Russian perforator” to identify the antrum, then removing the remainder of the mastoid cortex with hammer and gouge (Figure 2).
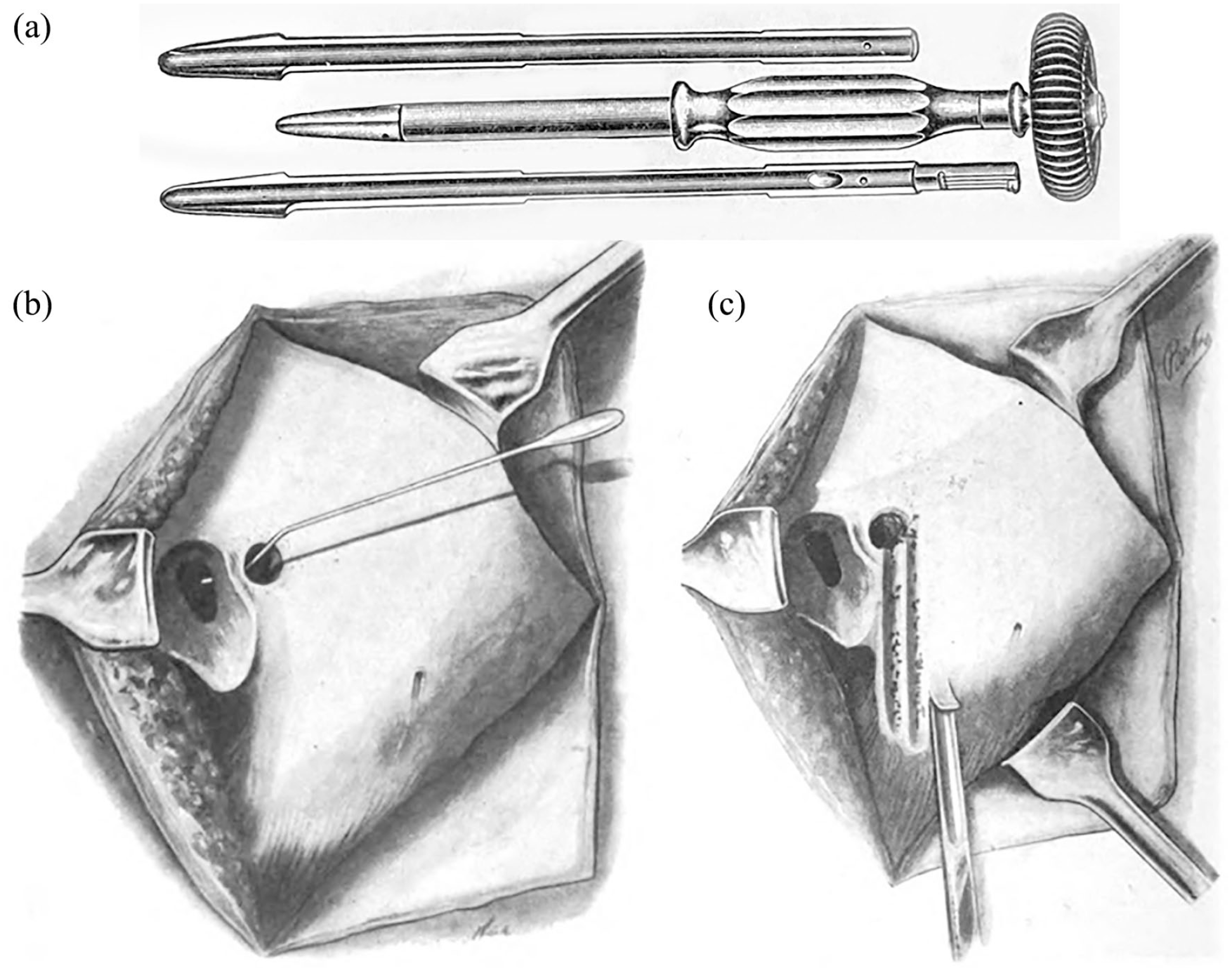
(a) The Russian perforator advocated for trepanation of the cortex by Ballenger. 5 (b) Trepanation of the mastoid at the suprameatal triangle. A probe is passed from the mastoid antrum to the epitympanum for confirmation. 5 (c) The mastoid cortex is removed with a curved gouge struck by a lead-filled mallet. 5
Adam Politzer
6
nicely describes the experience of opening the antrum in a patient with coalescent mastoiditis: If the middle portion of the planum mastoideum between the spinous supra meatum and the apex of the mastoid process is exposed, the cortex of this portion is chiseled away with a large gouge placed at an angle to the surface. When the cortex is sclerotic this must be done gradually layer by layer. Frequently the abscess is reached after the first blow with a hammer, whereupon the pus, which is under high pressure, flows out rapidly. Now and then the pus in the abscess cavity pulsates, a symptom which indicates that the dura or lateral sinus is exposed through the suppurative process in the middle ear.
A video from 1934 of a mastoidectomy using chisels and gouges is available at the Wellcome Museum website (https://wellcomecollection.org/works/zru3d57d). The video demonstrates the use of a gouge and mallet for the removal of the mastoid cortex, and a chisel and mallet for resecting the posterior meatal wall and outer attic wall.
As early as 1893, the use of a powered drill for performing a mastoidectomy was suggested by William Macewen, a Scottish neurosurgeon. 7 He claimed that the use of a rotary burr propelled by a surgical engine was the safest method for exposing the mastoid antrum. The “engine” was driven by hand or waterpower and the burr was inserted into a handpiece and held like a pen. He cautions that the burr should not be used to remove granulation tissue, as the facial nerve might be contained within it.
It was the influence of the brilliant otologic innovator, Julius Lempert, that led to wide acceptance of the surgical drill for mastoid resection. His simple subcortical mastoidectomy, via an endaural approach, gradually replaced the hammer and gouge with the more controlled electric dental drill and curette. 8
Footnotes
Data Availability
No data are included in this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Glenn Isaacson, MD, is a member of the Editorial Board of the ENT Journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics/Human Subjects
This study did not involve human subjects and has no identified ethical issues.