
Abstract
Introduction
An anterior glottic web can develop as a complication following surgical interventions for bilateral vocal fold lesions involving the anterior commissure.1,2 The resulting web can restrict vocal fold mobility and disrupt the mucosal wave through aerodynamic changes, leading to dysphonia, breathiness, and difficulty in phonation. 3 In severe cases, it can cause airway compromise and necessitate further interventions. 2 Several treatment methods have been employed to manage glottal webs, including laryngeal keel insertion with external or endoscopic approaches, staged operations with subsequent additional surgery, mucosal sutures, single and double mucosal microflaps (sliding technique), butterfly mucosal flap, and mitomycin-C (MMC) application.4-20 Bilateral vocal fold mucosal flaps combined with microsurgical mucosal sutures, endoscopic technique with ultrasound-guided mucosal fold lateralization, and anterior subglottic mucosal flap were also introduced for anterior glottic web treatment.21-23 However, these approaches have certain limitations and may not always yield satisfactory outcomes. 24
Laryngeal keel insertion with the external approach, which involves creating an open wound and scarring, can pose significant risks and lead to further voice decrement for the patient. 25 The endoscopic approach can also be uncomfortable for the patient, as the keel is fixed to the skin using buttons or other mechanisms.16,26-28 Moreover, using suture material to secure the keel can create a potential site for granulation tissue formation. 24 The displacement of the keel may result in respiratory distress or marked hoarseness. 6 Mucosal suturing, although attempted to approximate the edges of the anterior commissure, may not always be technically feasible, especially in cases with a significant mucosal gap.9,21,25,29 This limitation can impede the successful execution of the technique and hinder optimal wound healing. 9 Staged operations have been employed as a preventive strategy, but they are not without drawbacks.7,30-32 The recurrence or progression of the lesions during the waiting period between surgeries can pose challenges and complicate the management of the condition. 32 MMC application, while promising in preventing excessive scar tissue formation, still has certain limitations.10,33,34 The evidence regarding its effectiveness in preventing glottic web formation has yet to be conclusive.34,35 Factors such as the MMC application’s appropriate dosage and duration need further investigation.10,33 In addition, potential adverse effects and complications associated with MMC usage, such as mucosal injury or delayed wound healing, must be considered. 36
While various treatment options exist for anterior glottic webs, the importance of prevention cannot be overstated. Prevention is crucial because once a web has formed, its management becomes more complex, requiring additional procedures such as surgical division or phonosurgical techniques.5,12 Furthermore, treatment outcomes for established webs may not always be satisfactory, and there is a risk of recurrent web formation even after intervention. 8 Given these limitations, there is a need for alternative preventive strategies to effectively reduce the incidence of anterior glottic web formation in cases of bilateral vocal fold lesions involving the anterior commissure.
Our study proposes a modified preventive approach for anterior glottic web formation. Our process involves the simultaneous removal of bilateral vocal fold lesions involving the anterior commissure, followed by the application of MMC to the surgical site. Subsequently, at 4 to 6 weeks postoperatively, a laryngoscopic examination is performed. If there is a thick fibrin exudate that spans both vocal folds, it may indicate a possibility of web formation. In that case, a second operation is conducted to remove the fibrin exudate (scab) and reapply MMC. Our approach combines lesion removal with the application of MMC and includes a second-look operation when needed. The goal is to reduce the occurrence of anterior glottic webs.
Patients and Methods
Patient Population
A single-center retrospective study was conducted, comprising 23 patients who received laryngomicroscopic surgery (LMS) treatment for bilateral vocal fold lesions affecting the anterior commissure. The study period was between June 2021 and April 2023. Patients with previously established glottic web or adhesive scar between the two vocal folds were excluded from the study. Figure 1 illustrates the flowchart depicting the management of bilateral vocal fold lesions involving the anterior commissure. Table 1 provides an overview of the demographics and clinical characteristics of the patients. The study protocol was approved by the Institutional Review Board of our institution (No. 2023-06-044-001), and patient confidentiality was strictly maintained throughout the study.
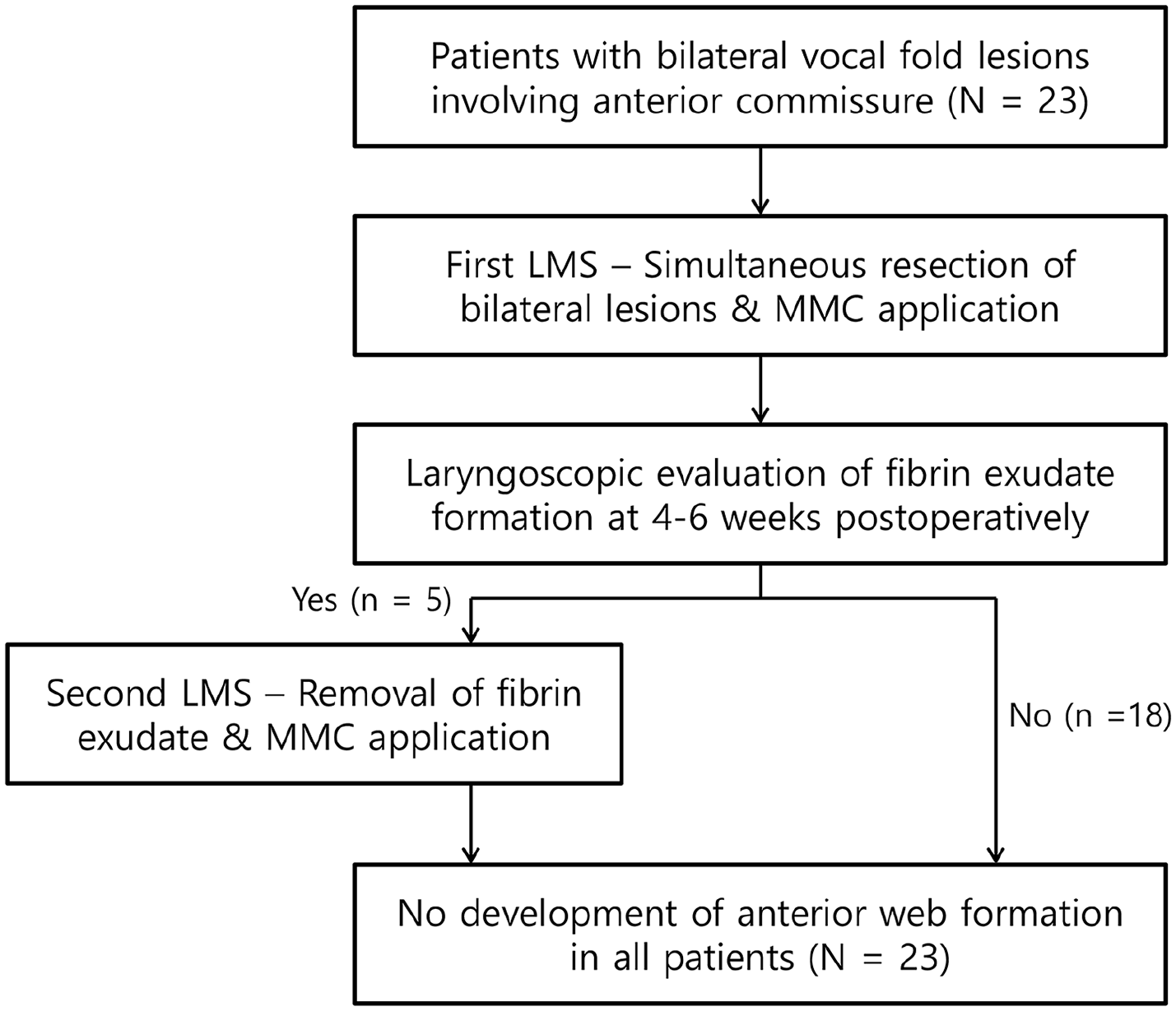
Management of bilateral vocal fold lesions involving the anterior commissure.
Demographics and Clinical Characteristics of All Patients.
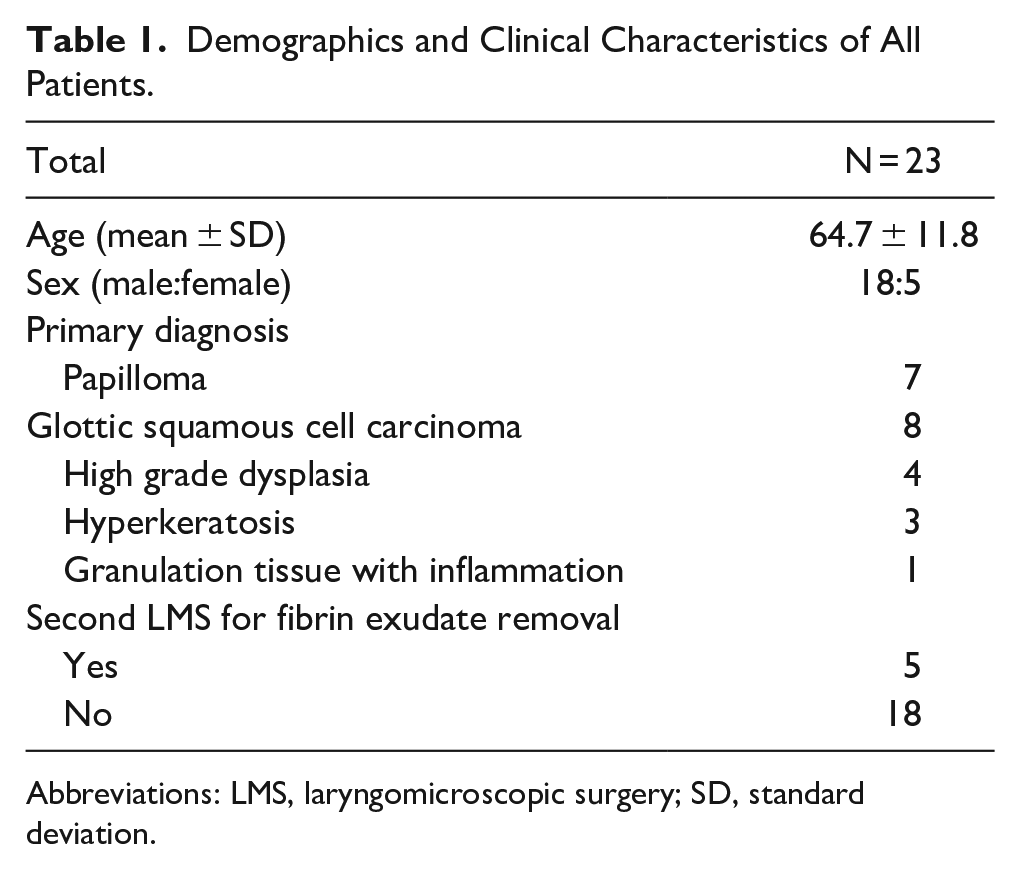
Abbreviations: LMS, laryngomicroscopic surgery; SD, standard deviation.
Surgical Procedure
Bilateral lesions were resected simultaneously using a AcuPulse CO2 laser (continuous superpulse mode laser with 1 watt) and microinstruments. As an AcuPulse CO2 laser keeps very brief laser-tissue interactions, there is a minimal thermal damage and tissue cooling techniques using this laser are not needed. After achieving hemostasis, cottonoid pledgets soaked with 0.04% MMC solution (Korea United Pharm. INC) was topically applied to the surgical site for 4.5 minutes. The patients were advised to refrain from using their voice for 2 days. At the time of the initial surgery, an operator explained the possibility that surgery to remove a web may be necessary after 4 to 6 weeks if it is observed in the outpatient visit. A laryngoscopic examination was performed at 4 to 6 weeks postoperatively. If a thick fibrin exudate was observed, overriding both vocal folds and indicating a potential for web formation, a second LMS procedure was performed to carefully remove the fibrin exudate using micrograsping forceps. Following this, topical MMC with the same concentration and duration was reapplied. In cases where no fibrin exudate was present, patients were observed at 2 to 6 month intervals based on their disease characteristics.
Evaluation of Web Formation and Statistical Methods
In this study, we analyzed the occurrence of glottic web formation before and after LMS. The size of the web was measured and expressed as a percentage of the total length of the membranous vocal fold. We measured glottic web through pointing the anterior commissure and fibrin exudate. More specifically, first, we measured the membranous vocal fold length between the anterior commissure and the vocal processes of the arytenoid cartilages. Second, web length is measured between the anterior commissure and fibrin exudate which is touching the both vocal cords. Then, the percentage was calculated by dividing the web length by the membranous vocal fold length. We presented the demographic and clinical characteristics of the participants through descriptive statistics, displaying categorical variables as frequencies and percentages.
Results
A total of 23 patients were included in our study. The clinical characteristics of all patients are summarized in Table 1. The mean age was 64.7 ± 11.8 years. There were 18 male and 5 female patients, with a male-to-female ratio of 3.6:1. The pathological diagnoses included papilloma, squamous cell carcinoma, dysplasia, hyperkeratosis, and inflammation. Among the patients, glottic cancer and papilloma were the prevalent diseases.
After undergoing LMS for bilateral vocal fold lesions, a laryngoscopic examination was conducted at 4 to 6 weeks postoperatively. Out of the total patients, 18 showed recovery without any anterior web or fibrin exudate. Follow-up periods of the 18 patients were a minimum of 10 months, a maximum of 30 months, and an average of 21 months. However, 5 individuals exhibited thick fibrin exudate overriding both vocal folds following the first LMS treatment. The length of the anterior glottic web in these patients ranged from 40% to 67%. Details of the 5 patients are summarized in Table 2.
The Details of the 5 Patients Who Exhibited Fibrin Exudate Overriding the Anterior Commissure Within 4 to 6 Weeks After Their Initial LMS Procedure.
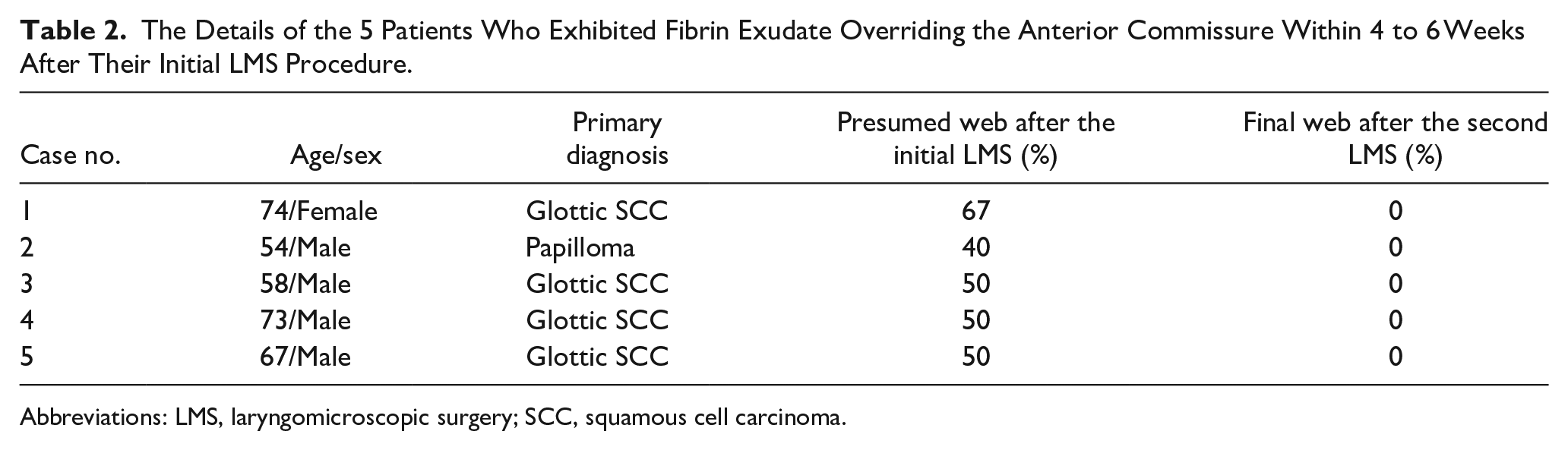
Abbreviations: LMS, laryngomicroscopic surgery; SCC, squamous cell carcinoma.
For these 5 patients, a second-look LMS procedure was performed to address the fibrin exudate and anterior glottic web. During the second LMS, the fibrin exudate was carefully removed to avoid any additional mucosal injuries. The fibrin exudate can be distinguished from granulation tissue because it is removed like a peel. Also, the smooth shape of a fibrin exudate is distinguishable from a recurrence. In our cases, there are no cases with recurrence or granulation tissue at the second LMS. Among the 5 patients, all patients experienced a clear recovery without any anterior web or fibrin exudate after 2 to 6 months following the second LMS procedure. Follow-up periods of the 5 patients were a minimum of 20 months, a maximum of 29 months, and an average of 24 months. During follow-up periods, there are no cases of relapse. No complications from topical MMC application were seen.
Figure 2 illustrates representative findings for the management of the anterior glottic web. It presents the case of a 67-year-old male patient with bilateral glottic cancer (T1b) who underwent CO2 laser cordectomy. At 6 weeks postoperatively, thick fibrin exudate at the anterior commissure was observed. During the second LMS procedure, the fibrin exudate was meticulously removed to avoid causing any additional mucosal injuries. Subsequently, a clear wound without any exudate or web was identified after 2 months of the second LMS. According to our calculating method, distance from anterior commissure to fibrin exudate is very minimal to measure, which is calculated into 0% web. Less than 15% web is considered acceptable. The wound healed effectively with no complications, remaining stable 23 months after the surgery.
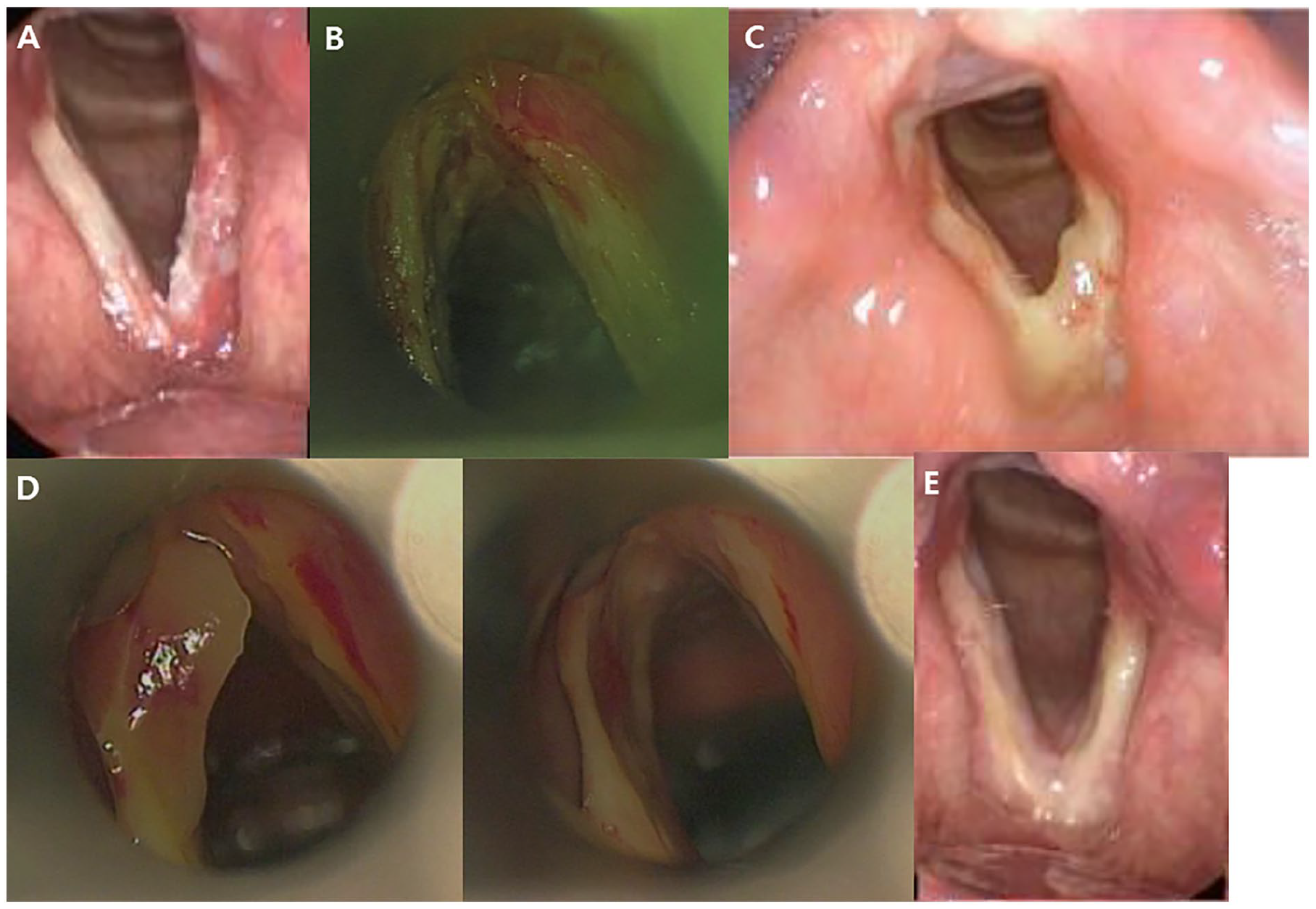
A 67-year-old male with a modified preventive approach. (A) Laryngoscopic finding of lesions. (B) LMS with mitomycin-C. (C) Fibrin exudate and web after 6 weeks. (D) Removal during second LMS. (E) Laryngoscopic finding after 2 months. LMS, laryngomicroscopic surgery.
Discussion
Our study presents a new preventive approach for dealing with the formation of anterior glottic web. Previous studies have investigated different management strategies for this condition, each with their own benefits and drawbacks. Our goal is to introduce an efficient management approach for bilateral vocal fold lesions that reduces the likelihood of anterior glottic web formation.
Many of our patients (18 out of 23) experienced a complete recovery without any signs of web formation or fibrin exudate after the first LMS procedure. This suggests that the use of MMC may play a role in preventing thick exudate and web formation, as the first LMS was sufficient to prevent web formation in 78.3% cases of bilateral vocal fold lesions involving the anterior commissure. MMC is an antineoplastic agent known to suppress fibroblast proliferation. 37 Roh et al have demonstrated that LMS with topical MMC application can effectively prevent the formation of anterior glottic web measuring less than 15% of the total length of the vocal folds, which is considered an acceptable small web. 12 Consistent with these previous findings which already proved the effect of MMC for preventing anterior glottic web,11,12 our study also demonstrates the potential of MMC in preventing glottic web formation. Depending on the surgeon’s technique or characteristics of a lesion, anterior glottic web may not occur, but it is certainly a possibility. If there is a possibility of web formation after surgery, our method can provide another option to surgeons and it is a meaningful thing. Future studies are needed to compare our surgical method group with control group.
In this study, we conducted observations on patients 4 to 6 weeks after the initial LMS procedure to assess the resolution of fibrin exudate. Shen et al observed morphologically mucosal healing process after laser cordectomy into 4 stages (wound exposure, exudation, granulation, and mucosa stabilization). 38 After laser cordectomy, fibrin formation is a natural course of the mucosal healing process. 38 Therefore, we can say that fibrin exudate which forms web is due to the surgery. While the optimal duration for observation has not been definitively established in previous studies, based on our experience, we found that fibrin exudate naturally resolved within 4 to 6 weeks following the first LMS. However, cases where fibrin exudate persisted for more than 6 weeks rarely resolved spontaneously and often led to the formation of web along the exudate. A previous study reported a median mucosal stabilization period of 57 days, with laryngeal mucosa stabilization achieved within 100 days after surgery in 80% of patients. 39 Taking this into consideration, it seems reasonable to evaluate fibrin exudate after 4 to 6 weeks of the first LMS procedure, considering the time required for mucosal stabilization. Accordingly, we performed a second LMS approximately within 8 weeks after the first LMS, following the assessment of fibrin exudate at the 4 to 6 week mark.
Five patients who presented with fibrin exudate or glottic web showed significant improvement after undergoing a second LMS procedure with topical MMC application. Notably, there was a 0% recurrence of anterior glottic web after the second procedure. However, it remains unclear whether the effect is primarily due to MMC or the removal of fibrin exudate. Nevertheless, it is evident that fibrin exudate removal is necessary, as both factors can influence wound healing and the prevention of glottic web formation.
In the classification of glottic web, the Cohen system is commonly used and categorizes glottic webs into 4 types: Type I, Type II, Type III, and Type IV.40,41 Type I represents glottis obliteration of less than 35%, Type II represents 35% to 50% obliteration, Type III represents 50% to 75% obliteration, and Type IV represents 75% to 90% obliteration. 41 In addition to Cohen’s classification, the thickness of the web has been emphasized as a significant factor in determining the appropriate treatment in a previous study. 33 Another study focused on measuring the length of the web by calculating the percentage length of the web portion in the membranous vocal fold. 1 In our study, we measured the length of the web portion in the membranous vocal fold and expressed it as a percentage of the total length of the membranous vocal fold. While there may be a slight error in measuring the length of the web portion, calculating the percentage of the web provides a more accurate measurement compared to Cohen’s classification, which only has 4 types. As we think that measurement of web thickness under the surgery does not seem accurate and large potential for error exists, we only measured the length of the web portion. Also, it seems that there are no significant differences between each web under the surgery.
There is another try to prevent scar formation. After LMS removal of lesion, adjunctive steroid injection is performed to reduce scar contracture and improve voice quality.42,43 Using local steroid injection to wound can be another option and further studies are needed.
There are some limitations to our study that we need to acknowledge. First of all, it is worth noting that our study was conducted retrospectively and took place at a single center, which means that the sample size was relatively small. This may limit the generalizability of our findings to a broader population. To enhance the validity of our results, larger-scale prospective studies involving multiple centers are needed. Another limitation is that we relied on descriptive statistics rather than establishing statistical significance, which restricts our ability to determine the efficiency of our proposed approach compared to other treatment modalities. Future studies should incorporate appropriate statistical analyses to evaluate the effectiveness of our management approach. In addition, we acknowledge that the optimal duration of observation for fibrin exudate and web formation has not been definitively established. There is a case report of anterior glottic web and granuloma formation after 4 months of LMS. 44 Further research is necessary to determine the most appropriate timeframe for assessment. Similarly, investigations are required to determine the optimal dose and duration of topical MMC application to maximize its preventive effects. Furthermore, future research focusing on the role of fibrin exudate removal would be valuable in confirming its impact on preventing anterior glottic web formation. Comparative studies evaluating different treatment modalities for bilateral vocal fold lesions, such as 2-staged operation and keel insertion, would also provide valuable insights to identify the most effective approach and establish it as the primary treatment modality for preventing anterior glottic web.
Conclusions
Our modified preventive approach for the formation of anterior glottic web has demonstrated effectiveness and safety, without significant complications. The use of topical MMC during the initial LMS procedure, followed by a second-look operation to remove fibrin exudate if required, along with subsequent reapplication of topical MMC, has emerged as an excellent treatment option. By implementing this approach, we have observed positive outcomes in terms of preventing anterior glottic web formation. Overall, our preventive approach offers an effective and safe solution for managing anterior glottic web formation.
Footnotes
Acknowledgements
None.
Data Availability Statement
Data of the study are available from the author with reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Samsung Medical Center, Seoul, Republic of Korea (No. 2023-06-044-001).
Statement of Human and Animal Rights
This study was approved by the Institutional Review Board of Samsung Medical Center, Seoul, Republic of Korea (No. 2023-06-044-001). Our study was conducted according to the Declaration of Helsinki.
Statement of Informed Consent
Patient informed consent was waived because this was a retrospective observational study. Patients were allowed to opt out of the research’s use of their data, and the related information.