
Abstract
Introduction
Tonsillectomy is a common surgical procedure performed to treat various infectious and neoplastic conditions and is associated with a variety of postoperative complications, including bleeding and infections.1,2 While most of the literature investigates pediatric patients undergoing the procedure, tonsillectomy is still a frequently performed surgery in adults. 3 Moreover, while these surgeries are generally considered safe, there is growing evidence suggesting that certain patient factors may influence the risk of medical and surgical complications following adult tonsillectomy.
Over recent decades, there has been a 3-fold increase in the prevalence of obesity [body mass index (BMI) ≥ 30] in the United States. 4 As a greater proportion of patients who are obese undergo tonsillectomy, it is important to understand the relationship between obesity and complications following surgery. Studies have also previously identified obesity as a risk factor for hemorrhage following tonsillectomy, 5 suggesting that there is an increased need to identify patients with elevated BMI to adequately mitigate their risk before surgery.
Traditionally, the World Health Organization (WHO) classification system has been employed to categorize patients into BMI groups for health assessments. However, it is increasingly evident that this categorical approach may not fully capture the nuanced relationship between BMI and surgical outcomes in contemporary patients, considering evolving patient demographics, lifestyles, and surgical techniques.
Furthermore, studies that have examined the impact of elevated BMI on complications following tonsillectomy have yielded mixed results. Some studies show no association between elevated BMI and postoperative complications, 3 while other studies indicate obesity may be a risk factor for postoperative complications following tonsillectomy, 6 including hemorrhage and respiratory events.5,7 This discrepancy underscores the necessity to establish data-driven BMI thresholds specific to tonsillectomy that can accurately predict postoperative complications. Therefore, this study aimed to identify data-driven BMI strata associated with varying risks of 30 day complications following tonsillectomy in adults.
Methods
The REporting of studies Conducted using Observational Routinely-Collected Data (RECORD) guidelines for reporting of studies conducted using observational routinely collected health data were used to ensure proper reporting of methods, results, and discussion. 8
Data Source
A retrospective cohort study of patient data from the American College of Surgeons National Surgery Quality Improvement Program (ACS-NSQIP) database was performed. ACS-NSQIP is a multi-institutional outcome program specifically designed to assess and adjust for surgical risks. Details pertaining to data collection strategies, inclusion criteria, sampling procedures, and measured outcomes have been previously documented. 9 Each hospital assigns a trained surgical clinical reviewer (SCR) to collect preoperative through 30 day postoperative data on randomly assigned patients. SCR training is provided by ACS. The database contains a comprehensive set of more than 100 variables from over 600 participating institutions, covering patient demographics, risk factors, preoperative laboratory values, procedural details, and 30 day morbidity and mortality outcomes. 10 In addition, the database provides only de-identified information to users, thus exempting this study from Institutional Review Board approval.
Study Population
Patients who underwent tonsillectomy were identified using Current Procedural Terminology (CPT) code CPT-42821 or CPT-42826. Patients with missing data including age, gender, height, and weight were excluded. To reduce confounders, patients presenting with pregnancy, ventilator dependency, congestive heart failure, greater than 10% preoperative weight loss, preoperative transfusion requirements, systemic sepsis, contaminated and infected wounds, a reported age under 18 years, a BMI less than 18.5 kg/m2 or greater than 60 kg/m2 were also excluded. In total, 44,161 patients undergoing adult tonsillectomy were included in this study. The inclusion and exclusion criteria are depicted in Figure 1.
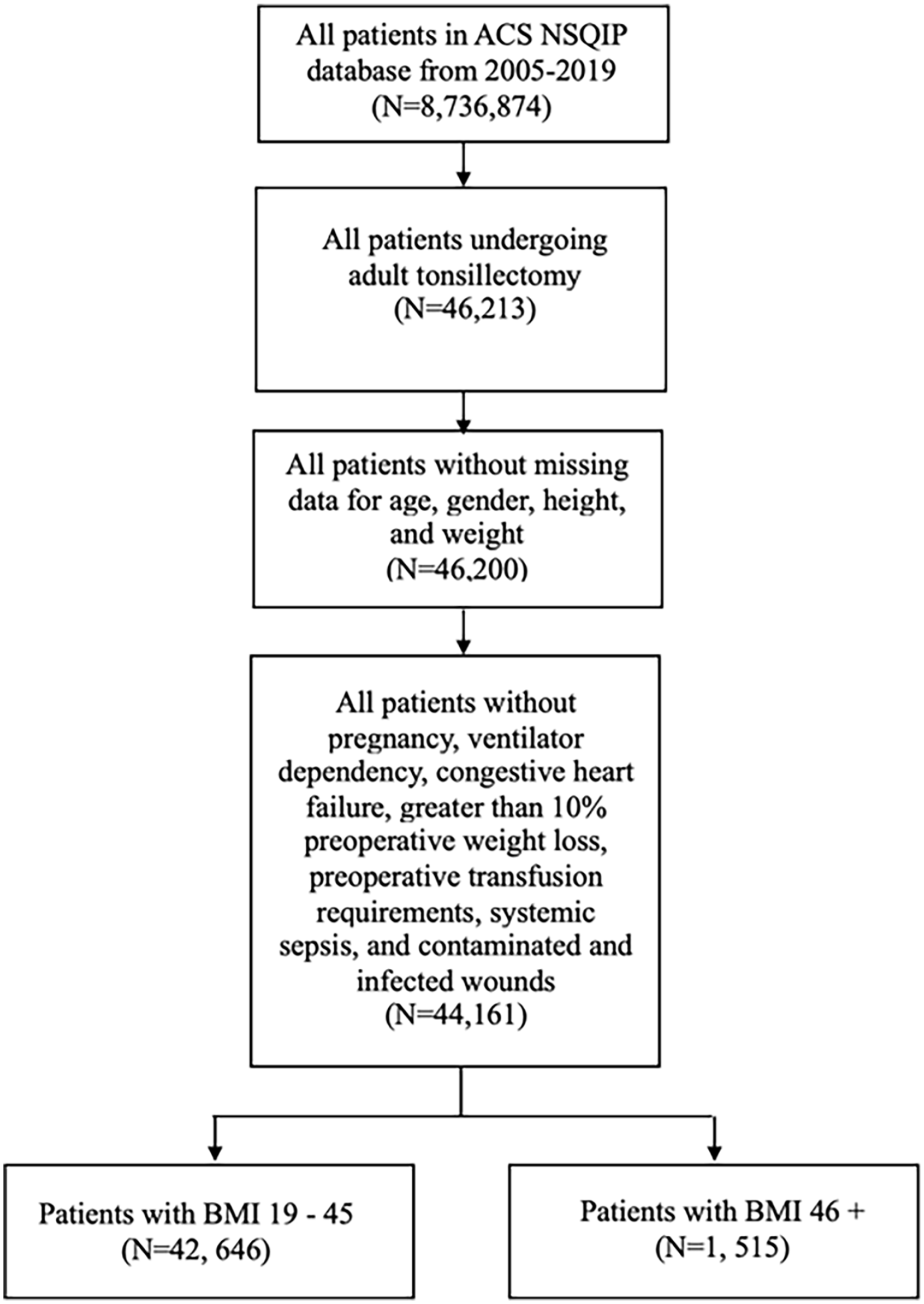
Flow diagram showing exclusion and inclusion criteria.
Demographic Comorbidities and Outcome Variables
Patient demographics and comorbidities included age, gender, race, diabetes, smoking status, dyspnea, history of severe chronic obstructive pulmonary disease, ascites, hypertension requiring medication, steroid use, and bleeding disorders.
The primary outcome was the creation of data-driven BMI strata that maximize the likelihood of 30 day all-cause complications. All-cause complications included superficial surgical site infection (SSI), deep SSI, organ-space SSI, wound disruption, pneumonia, unplanned intubation, prolonged ventilator use, pulmonary embolism, renal insufficiency, acute renal failure, cardiac arrest, myocardial infarction, postoperative sepsis, septic shock, transfusion, urinary tract infection, cerebrovascular accident, bleeding, and deep vein thrombosis (DVT). Major complications included deep SSI, organ-space SSI, wound disruption, pneumonia, unplanned reintubation, pulmonary embolism, prolonged ventilator use, acute renal failure, stroke, cardiac arrest, myocardial infarction, sepsis and septic shock. Minor complications included superficial SSI, deep venous thrombosis or thromboembolism (considered the same event in the NSQIP), renal insufficiency, urinary tract infection, and blood transfusion. This classification of major and minor complications aligns with previous studies using ACS-NSQIP for surgical outcome analysis.11-13
Statistical Analysis
Using the stratum-specific likelihood ratio (SSLR) analysis, data-driven BMI strata were established to identify the BMI threshold that maximized the likelihood of 30 day all-cause complications. SSLR is an adaptive technique that surpasses traditional receiver operating characteristic (ROC) curves in enabling the identification of data-driven strata that optimally differentiate indicated complications. The SSLR methodology has been widely used in surgical literature to derive data-driven BMI thresholds that maximize complication rates.14,15 Introduced by Pierce and Cornell in 1993, 16 SSLR employs likelihood ratios to establish these strata. In our study, the likelihood ratios indicated the degree of increased or decreased likelihood of experiencing a 30 day all-cause complication following tonsillectomy among patients above or below a certain BMI value.
We conducted an SSLR analysis for 30 day all-cause complications following tonsillectomy to identify the BMI threshold that maximized complication rates. To conduct SSLR, we determined the rate of 30 day all-cause complications for each BMI value in our sample. We subsequently calculated likelihood ratios and a 95% confidence interval (CI) for each BMI value based on the total rate of 30 day all-cause complications. BMI values with overlapping likelihood ratio CIs were systematically collapsed. This process was continued until adjacent strata displayed a significant difference in SSLRs, which was indicated by likelihood ratio 95% CIs that did not overlap. A BMI threshold was established at this point, which indicated the BMI value at which 30 day all-cause complication differences were optimized.
Following the identification of data-driven strata, univariate analysis was conducted to assess demographic variables, preoperative comorbidities, and 30 day outcomes stratified by the strata. Demographics and outcomes were analyzed using appropriate chi-square and student t tests. The results were presented as the number of patients in each category, the incidence or prevalence rate (%), mean ± standard deviation, and the corresponding P value, where applicable. Demographic variables and preoperative comorbidities that showed significance (P < .05) in the univariate analysis were controlled for in multivariate binary logistic regression modeling to account for any potential confounding variables. Significance was assessed at a P value of less than .05. All analyses were performed using Statistical Package for the Social Sciences (SPSS) v.21 (IBM Corporation).
Results
Thirty-Day Major Complications
SSLR identified 2 data-driven BMI strata that maximized the likelihood of 30 day all-cause complications: 18 to 45 and 46+ (Table 1). The 30 day major complication incidence rate was 1.35% in the 18 to 45 BMI cohort and 2.44% in the 46+ cohort (Table 2, P < .001).
BMI Thresholds for 30 Day Complications Identified Through Stratum-Specific Likelihood Ratio Analysis.
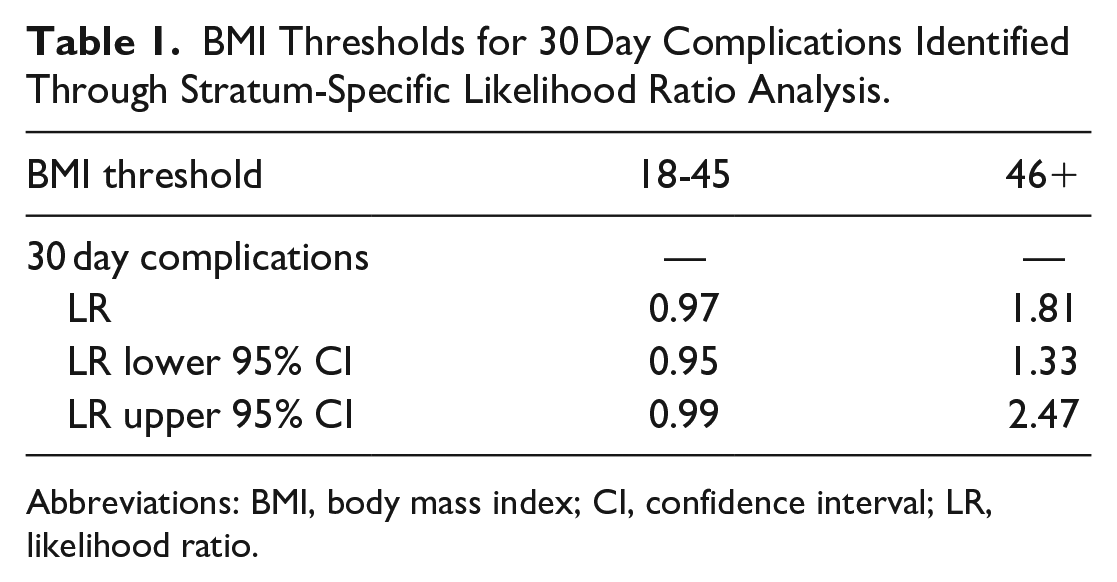
Abbreviations: BMI, body mass index; CI, confidence interval; LR, likelihood ratio.
Incidence of 30 Day Complications by BMI Strata.
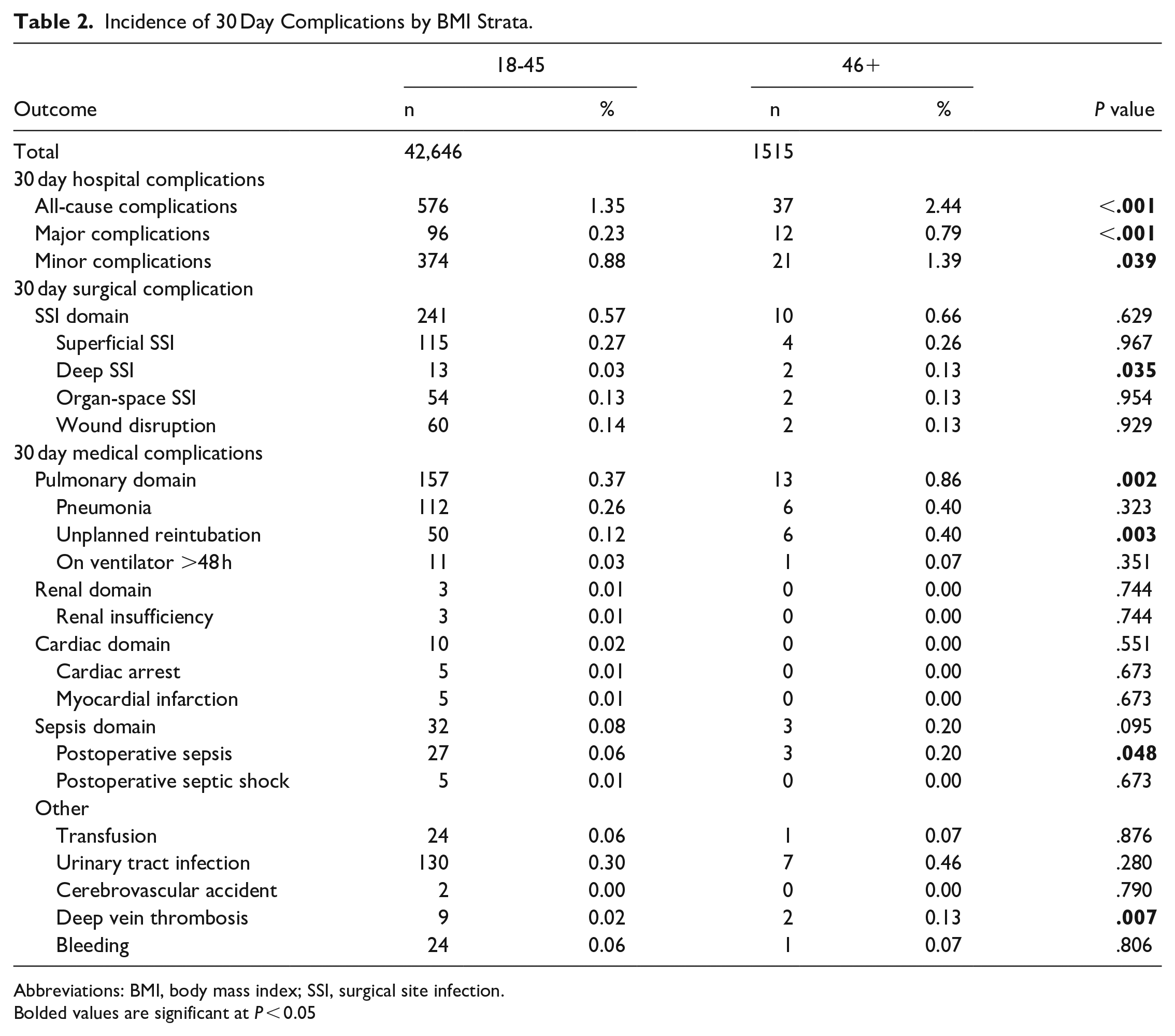
Abbreviations: BMI, body mass index; SSI, surgical site infection.
Bolded values are significant at P < 0.05
Descriptive Statistics
A total of 46,213 patients were identified with CPT-42821 or CPT-42826. Following exclusion, 44,161 patients were selected for analysis. The demographic and clinical characteristics of these patients are presented in Table 3. Patients in the 46+ strata were more likely to be marginally older (31 years vs 30 years), male (82% vs 65%), have diabetes (13% vs 3%), dyspnea (5% vs 1%), hypertension requiring medication (25% vs 8%), and smoke (19% vs 16%; all P < .01; Table 3).
Demographic and Clinical Comorbidities of 2 BMI Strata for Patients Undergoing Adult Tonsillectomy.
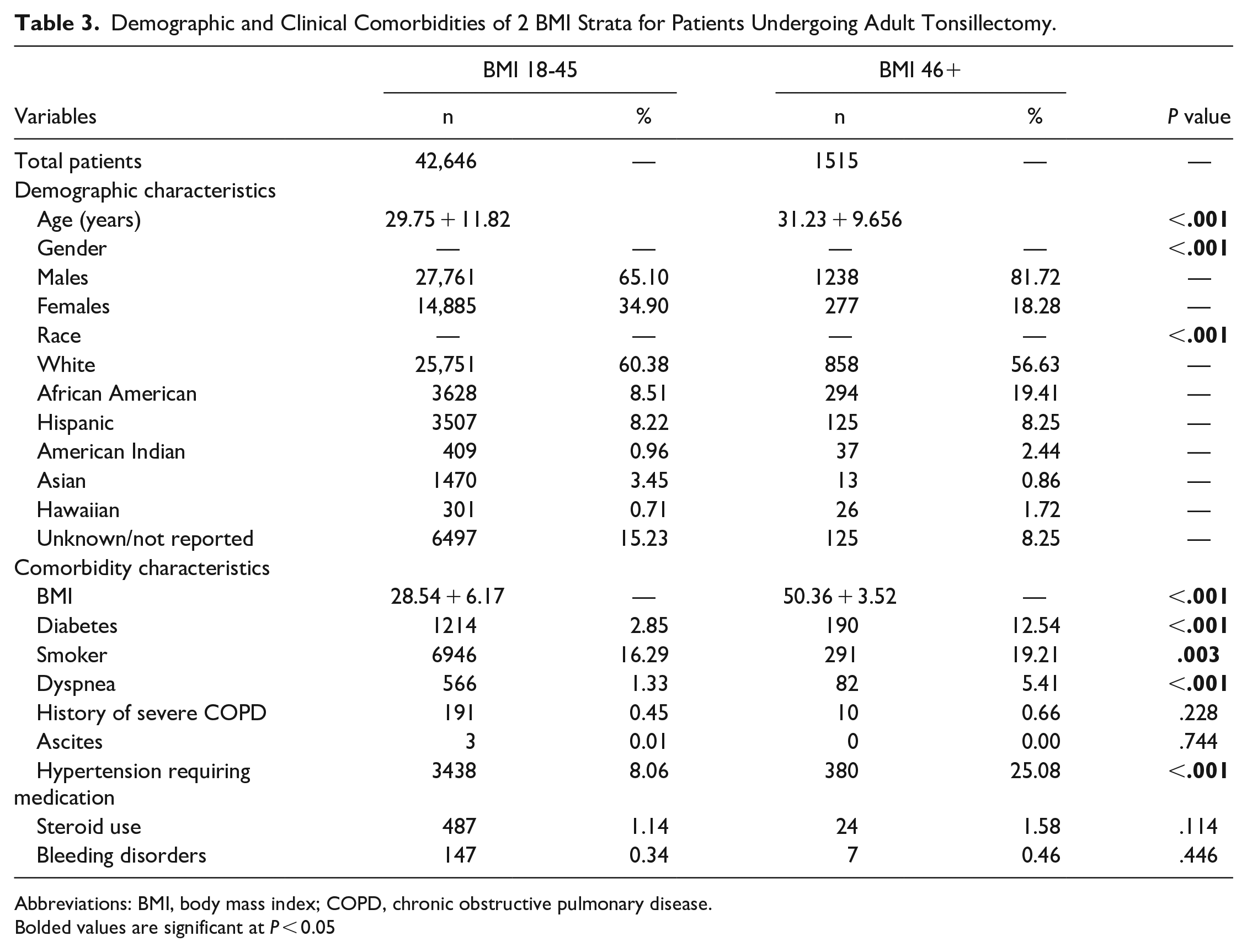
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease.
Bolded values are significant at P < 0.05
Univariate Analysis
When compared to the 18 to 45 cohort, the 46+ cohort had a higher incidence of all-cause complications (2.44% vs 1.35%, P < .001), major complications (0.79% vs 0.23%, P < .001), minor complications (1.39% vs 0.88%, P = .039), deep SSIs (0.13% vs 0.03%, P = .035), pulmonary domain complications (0.86% vs 0.37%, P = .002), unplanned reintubation (0.40% vs 0.12%, P = .003), postoperative sepsis (0.20% vs 0.06%, P = .048), and DVT (0.13% vs 0.02%, P = .007). No significant difference was observed for other outcomes (P > .05 for all, Table 2).
Multivariate Analysis
After controlling for confounders, a BMI of 46+ was shown to be an independent risk factor for all-cause complications [odds ratio (OR): 1.62, 95% CI: 1.14-2.30, P = .007, Table 4], major complications (OR: 2.86, 95% CI: 1.51-5.43, P = .001, Table 4), pulmonary domain complications (OR: 1.86, 95% CI: 1.03-3.36, P = .041, Table 4), unplanned reintubation (OR: 2.65, 95% CI: 1.08-6.49, P = .033, Table 4), and DVT (OR: 6.54, 95% CI: 1.25-32.94, P = .026, Table 4).
Multivariate Logistic Regression Analysis for 30 Day Complications by BMI Strata.
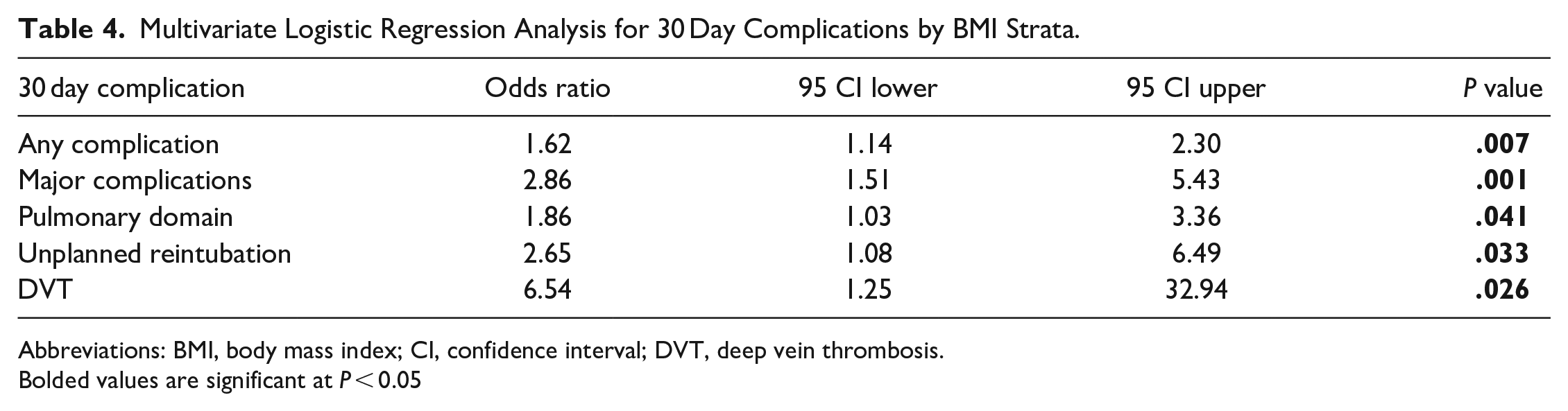
Abbreviations: BMI, body mass index; CI, confidence interval; DVT, deep vein thrombosis.
Bolded values are significant at P < 0.05
Discussion
Utilizing the SSLR analysis, our investigation revealed a BMI threshold of 46 that maximized the likelihood of 30 day all-cause complications following adult tonsillectomy. In contrast to previous research, which primarily relied on discrete BMI categories defined by the WHO classification, our investigation assessed BMI on a continuum. Thus, this study is the first of its kind to evaluate 30 day outcomes based on data-driven BMI strata rather than utilizing an arbitrary tiered system and offers a novel perspective on the association between BMI and postoperative tonsillectomy outcomes.
Previous studies that have investigated the association between obesity and tonsillectomy have found that pediatric patients with obesity may be at a greater risk of respiratory complications following tonsillectomy. 17 In addition, Hoshino et al established that obesity is independently associated with post-tonsillectomy hemorrhage. 5 De et al established that obese children undergoing adenotonsillectomy for obstructive sleep apnea are at increased risk for residual obstructive sleep apnea on the night of surgery and that special considerations are warranted for postoperative monitoring and treatment. 18 However, even though a significant number of adults undergo tonsillectomy, 19 few studies examine the landscape of obesity and tonsillectomy in adult patients.
To the best of our knowledge, only one study investigates BMI thresholds undergoing tonsillectomy in adults. Gabriel et al 20 established that Class 3 obesity (BMI > 40 kg/m2) was associated with an increased incidence of same-day admission following adult outpatient tonsillectomy. Although the previously mentioned study elucidates important results, this study’s contribution lies in its use of a data-driven approach, which identifies a critical BMI threshold associated with a significantly increased risk of 30 day complications. In addition, this study evaluates the risk of complications following tonsillectomy. We independently associate a BMI of 46+ with various 30 day complications, including pulmonary domain complications and thromboembolic events, which has not been investigated previously. This novel finding suggests that stratifying patients based on this data-driven BMI threshold could enhance risk prediction and enable tailored management strategies for patients undergoing adult tonsillectomy.
The presence of comorbidities such as diabetes, dyspnea, hypertension requiring medication, and smoking in the 46+ BMI cohort provides a plausible pathophysiological explanation for the heightened incidence of complications. These comorbidities may increase surgical risk, as they are known to have detrimental effects on wound healing, immune response, and cardiovascular function. 21 In particular, comorbidities associated with obesity, such as diabetes, constitute independent risk factors for compromised anastomotic wound healing and non-SSIs. 22 Obesity-related dyspnea further elevates the likelihood of pulmonary postsurgical complications, while obesity itself heightens the risk of thromboembolisms.23,24
Of note, our analysis uncovered some complications which were significant in univariate analysis, yet lost significance after controlling for comorbidities such as diabetes, smoking status, dyspnea, and hypertension (Tables 2 and 4). The loss of statistical significance suggests that these complications, including postoperative sepsis and deep SSI, may in part have contributions from these comorbidity differences between the BMI cohorts and are not independently predicted by adiposity alone. This attenuation of significance observed in the multivariate analysis suggests a potential interaction between high BMI and comorbidities in influencing the rates of these complications. Indeed, prior literature has suggested that deep SSIs have increased odds in patients with diabetes, 25 smoking, 26 and hypertension 27 due to impaired wound healing and vasoconstriction, thereby further substantiating our suspicion of a potential interaction with high BMI for selected complications.
Nevertheless, our findings demonstrate that obesity remains an independent risk factor for all-cause complications after tonsillectomy, even when controlling for these accompanying comorbidities through multivariate regression analysis. Obesity influences wound healing, 28 tissue repair, 29 and the immune response. 30 Thus, metabolic dysfunction and the altered immune response associated with obesity may potentially exacerbate the body’s susceptibility to surgical stress and contribute to the elevated complication rates observed in individuals with a BMI greater than 46. 31
Our study also found an association between obesity and an increased likelihood of pulmonary domain complications and unplanned re-intubation following adult tonsillectomy. These findings may suggest the unique challenges and physiological implications that obesity poses for the respiratory system during and after surgery. Obesity exerts a significant impact on respiratory function, with excess adipose tissue in the chest and abdomen restricting diaphragmatic movement and lung expansion. Consequently, obese individuals often exhibit reduced lung compliance and functional residual capacity, 32 which impairs efficient gas exchange and ventilation. These alterations in respiratory physiology may make obese patients more susceptible to pulmonary domain complications following tonsillectomy.
Furthermore, the mechanical challenges posed by obesity can complicate airway management during intubation. The increased adipose tissue in the neck and throat area can hinder visualization and access to the airway, 32 potentially leading to difficulties in establishing and maintaining a secure airway during the surgical procedure. Such challenges may contribute to an increased risk of unplanned intubation as healthcare providers navigate the complexities of airway management in obese patients. The combination of compromised respiratory function and airway management difficulties in obese individuals undergoing tonsillectomy underscores the need for heightened vigilance, and proper preoperative assessment and planning become crucial to anticipate potential airway difficulties and formulate contingency measures to address complications promptly.
Our study found an association between obesity and an increased likelihood of DVT following adult tonsillectomy. One plausible explanation includes that obesity is known to be associated with a proinflammatory state and increased levels of certain clotting factors in the blood, which can promote the formation of blood clots. 33 Second, the surgical procedure itself can lead to a temporary reduction in mobility, increasing the risk of DVT. Obese individuals often have compromised blood flow due to the excess adipose tissue, which can slow down circulation, further predisposing them to clot formation during periods of immobility. 34 Therefore, the combination of obesity-related physiological changes and reduced mobility postsurgery collectively may elevate the risk of DVT in obese adult tonsillectomy patients, making it crucial to consider preventive measures and close monitoring in this population.
While certain studies have reported a significant increase in the occurrence of post-tonsillectomy hemorrhage among obese patients, 17 others have failed to establish a clear correlation between weight and bleeding complications following the procedure. 35 In our study, we did not observe a significantly higher odds of bleeding in the 46+ BMI cohort within the 30 day postoperative period. These findings prompt the need for further research to elucidate the complex interplay between BMI and bleeding complications in adults undergoing tonsillectomy. Clarifying this relationship is crucial for informing clinical practice and optimizing patient outcomes, especially in the context of tonsillectomy.
The results of this study have significant clinical implications. Establishing a BMI threshold linked to a higher complication risk (46+) can provide surgeons with a useful risk assessment tool. This threshold aids in identifying patients who might benefit from more vigilant monitoring, tailored interventions, or specialized postoperative care to mitigate the risk of adverse outcomes. Moreover, we utilize a data-driven approach, moving beyond traditional categorical BMI classifications.
Furthermore, our study underscores the potential role of prehabilitation programs in mitigating the risks associated with obese patients undergoing tonsillectomy, specifically regarding pulmonary domain complications. Previous research has found improved surgical outcomes in obese patients following pulmonary rehabilitation. 36 Given that our findings displayed a significantly higher odds of pulmonary domain complications in the 46+ BMI cohort within 30 days of tonsillectomy, targeted interventions, such as respiratory exercises, incentive spirometry, and inspiratory muscle training, in the preoperative period may be considered to increase lung capacity and improve oxygenation for obese patients undergoing this procedure.
In addition, in light of our findings that the 46+ BMI cohort had a significantly higher odds of DVT within 30 days following tonsillectomy, close monitoring for signs and symptoms of DVT, such as swelling, pain, and redness, in the lower extremities is important in the postoperative period. Educating patients about these potential indicators also should be considered, so prompt medical attention can be sought. In addition, the possibility of implementing prophylactic measures to prevent DVT warrants consideration, although further research is needed to better elucidate the nuanced interplay of factors underlying the association between obesity and DVT after tonsillectomy.
The strength of this study is the utilization of a national database and a large sample size for SSLR analysis. Nonetheless, this study is not without its limitations. The retrospective nature of this study presents inherent limitations. The lack of control over data collection procedures and potential selection bias may result in variability in data quality and completeness between different institutions, which may affect the generalizability of the findings. Furthermore, the retrospective design inherently poses challenges in establishing causation. ACS-NSQIP is also limited to 30 day postoperative morbidity and mortality data, which limits the study to short-term outcomes, and we were unable to capture the full spectrum of complications that could arise beyond the 30 day postoperative period. In addition, ACS-NSQIP may not fully capture nuances in the variability in surgical expertise across different healthcare institutions; however, this would be expected to influence both cohorts to a similar degree.
BMI, as a measure of body composition, has inherent limitations, particularly in assessing fat distribution and regional adiposity. Patients with similar BMI scores may have vastly different body compositions, with variations in the proportion of muscle, fat, and bone mass. Thus, utilizing BMI as a measure of body fat may not fully capture these factors. In particular, BMI does not differentiate between different types of adipose tissue, such as subcutaneous fat (located under the skin) and visceral fat (located around internal organs), which precludes insight into individual metabolic profiles. Thus, the reliance solely on BMI as a risk stratification tool may overlook important patient-specific factors that could influence the likelihood of complications following adult tonsillectomy.
Nevertheless, this study is valuable because it addresses a gap in the existing literature regarding the association between BMI and complications after adult tonsillectomy. Previous research in this area mainly relied on the standard WHO classification system, neglecting nuanced variations in BMI and its correlation with surgical outcomes, and primarily focused on pediatric patients. By employing a data-driven approach, this study considers BMI on a continuum, and we identify a specific BMI threshold linked to an increased risk of medical and surgical complications within 30 days following adult tonsillectomy.
Conclusion
A data-driven BMI threshold of 46+ was associated with a significantly increased risk of all-cause complications following adult tonsillectomy. This is the first tonsillectomy study to observe BMI on a continuum and observe at what point BMI is associated with increased risk of complications following adult tonsillectomy. Our identified BMI strata can be incorporated into risk-stratifying models for predicting 30 day complications to minimize them.
Footnotes
Author Contributions
Conceptualization: A.R.; Data curation: A.R.; Formal analysis: A.R.; Funding acquisition: T.A.; Investigation: A.R., T.A.; Methodology: A.R., T.A. Project administration: A.R., T.A.; Resources: T.A.; Software: A.R.; Supervision: T.A.; Validation: A.R., T.A.; Visualization: A.R., T.A.; Writing—original draft: A.R., T.A.; Writing—review and editing: A.R., T.A.
Data Sharing and Data Availability Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.