
Abstract
Significance Statement
The ear is a common site of keloid formation, usually after ear piercing, causing cosmetic concerns. In contrast, bilateral ear keloid development secondary to trauma caused by using masks with ear loops has not been reported, yet. We present an unusual case of large bilateral posterior auricular keloids secondary to prolonged mask use during COVID-19 pandemic. Both keloids were successfully treated with a combination of surgical excision and local triamcinolone injection.
Case Presentation
A 43-year-old Caucasian male patient presented to the outpatient Ear, Nose, and Throat department with an 18-month history of large gradually growing bilateral masses behind the pinna, causing cosmetic concerns. The patient had been working as a healthcare professional during COVID-19 pandemic and had been extensively using protective facial masks with ear loops on a daily basis. There was no previous surgical intervention in the region. Past history included hypertrophic scar formation after an abdominal operation.
On clinical examination, the presence of firm large subcutaneous masses indicative of posterior auricular keloids on both sides was confirmed (Figure 1). The skin was intact without ulceration. Considering patient’s history, keloid formation was secondary to chronic trauma of the auricular skin due to prolonged use of facial masks with ear loops.
Preoperative photo of the left (A) and the right (B) auricular keloid.
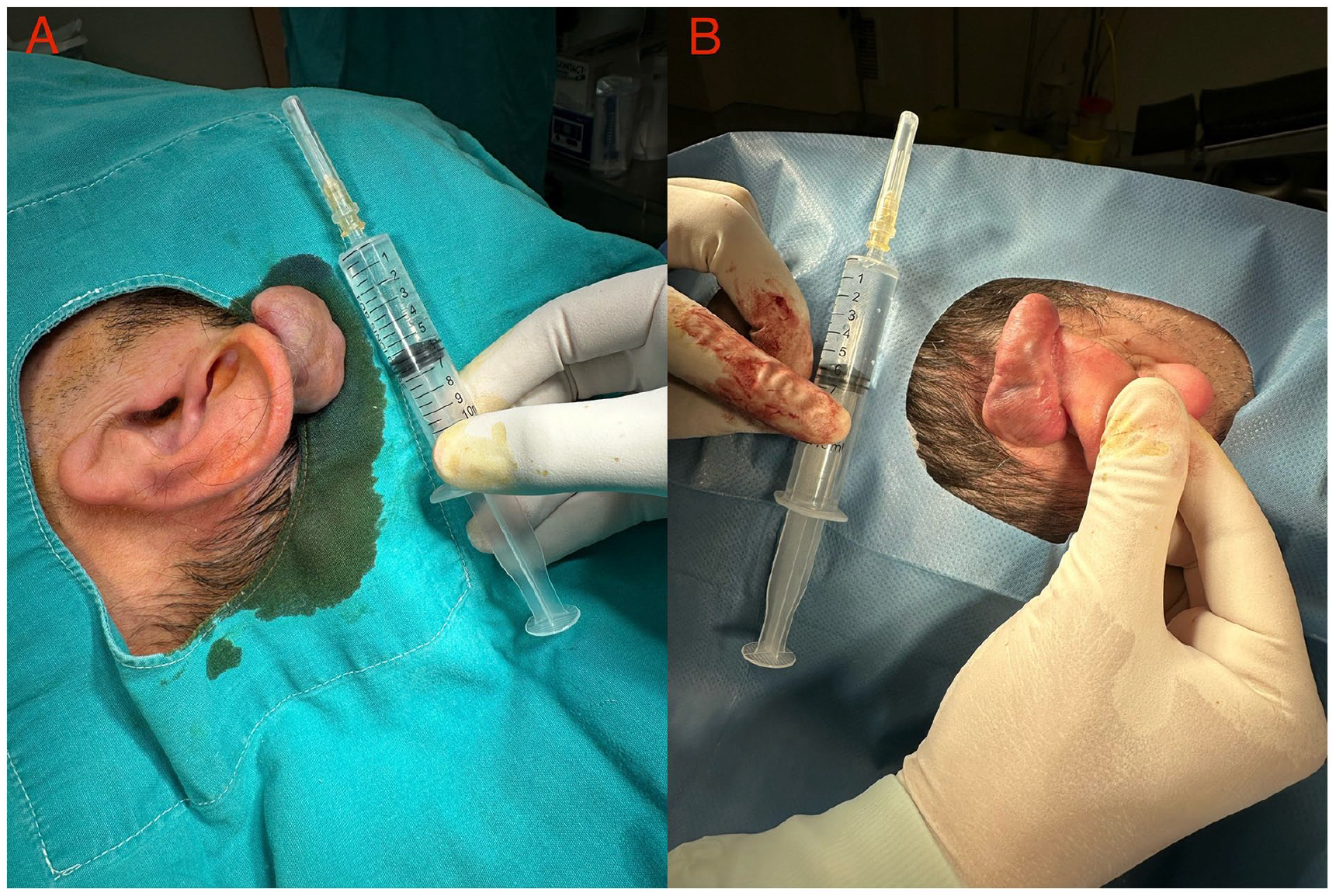
The management included a combination of complete surgical excision and triamcinolone acetonide corticosteroid (TAC) injection. Specifically, after local anaesthesia infiltration with 2% lidocaine hydrochloride, both keloids were completely removed (Figure 2) followed by primary low-tension closure with interrupted 4.0 polypropylene sutures. In addition, we proceeded with local infiltration of 1 ml of TAC 40 mg/ml on each surgical site. The use of a mask strap to avoid further ear skin irritation was recommended. The sutures were removed after 8 days. Local TAC injection on both surgical sites was repeated at 1 and 3 month(s) after surgery. The findings on histological examination confirmed the clinical diagnosis of auricular keloids of dimensions 3.8 cm × 2.7 cm × 2.6 cm on the left side and 4.4 cm × 2.9 cm × 2.3 cm on the right side (Figure 3). The patient has been followed up for 10 months since treatment with satisfactory healing and no evidence of local recurrence.

Intraoperative photos after complete surgical excision of both keloids showing the broad base of each specimen attached to the auricle (A: left side, B: right side).
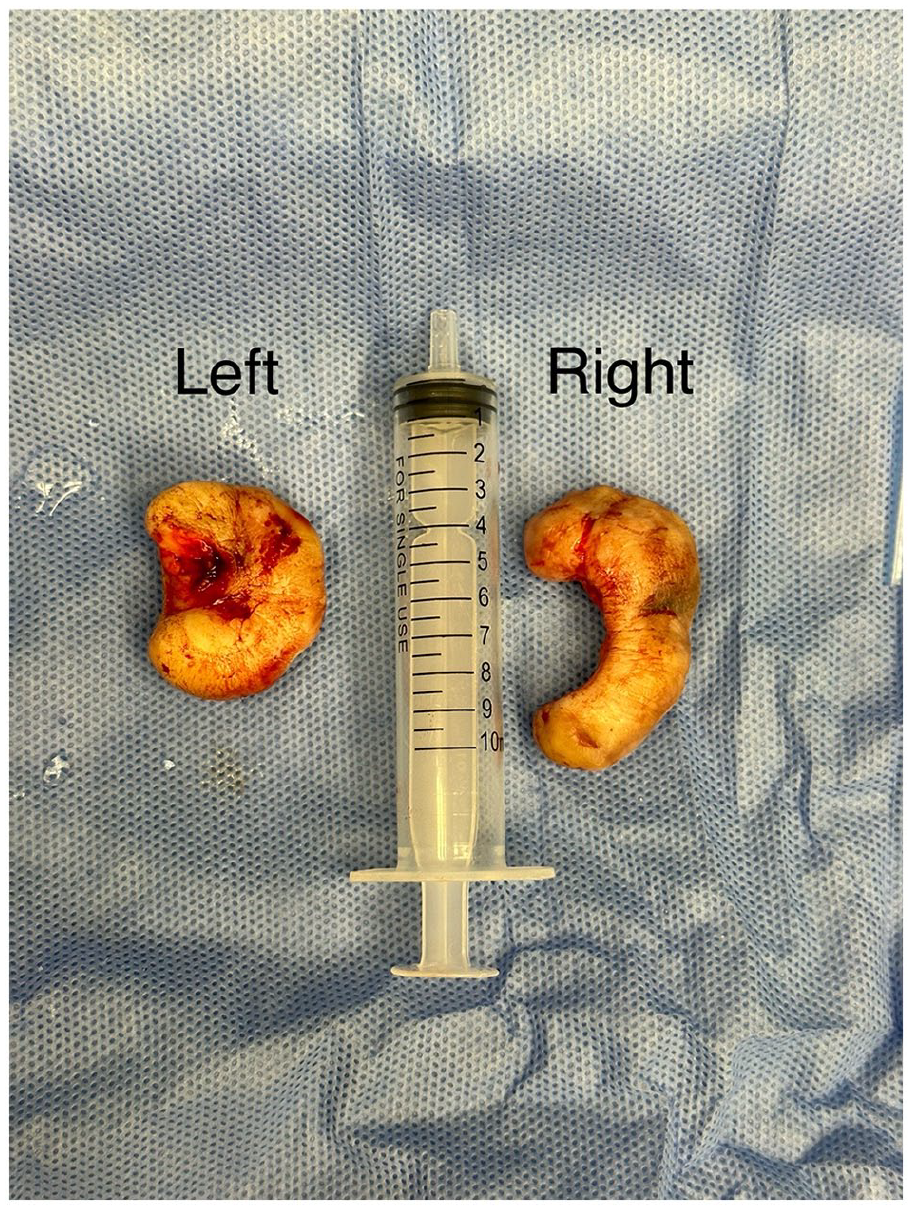
A photo of the left and right keloid specimens after complete excision with dimensions of 3.8 cm × 2.7 cm × 2.6 cm and 4.4 cm × 2.9 cm × 2.3 cm, respectively.
Keloids are benign dermal fibrotic lesions resulting from abnormal wound healing in response to skin trauma. 1 They are characterized by aberrant collagen deposition proliferating beyond the original trauma margins and variable size due to continuous evolvement over time. A higher incidence of keloids is seen with greater frequency in darker skinned individuals of African, Asian, and Hispanic origin with a prevalence of up to 16%. 2
Ear keloids are visible and usually impose cosmetic and psychological concerns for patients. Earlobe and helix are common sites for keloid formation usually after ear piercing. In contrast, posterior auricle is a rare location for keloid formation, especially in the absence of a history of previous surgery in this area. 3 To our knowledge, only one case of unilateral posterior auricular keloid which appeared to arise due to prolonged mask use has been reported. 4
The role of using masks in preventing the spread of infectious diseases especially in the COVID-19 era is inevitable. However, prolonged use of masks with ear loops can lead to trauma at the retroauricular skin region, increasing the risk of keloid development.
The management of auricular keloids is challenging. Surgical excision alone appears to have a high recurrence rate of almost 100%, whereas combination therapy seems to be more effective, although no consensus about the best treatment modality exists. Apart from surgical excision, adjuvant therapies consist of intralesional corticosteroid (TAC) or 5-fluorouracil injection, topical mitomycin C or imiquimod application, radiotherapy, pressure therapy, cryotherapy, and laser therapy with variable outcomes. In addition, avoiding sun exposure and using sunscreen on a healing scar can reduce the risk of keloid recurrence. The combination of complete surgical excision with TAC injection has shown favourable results with a mean recurrence rate of 15.4%. 5
The challenges in keloid management highlight the importance of avoiding skin trauma, when feasible, especially in high-risk patients with a tendency to develop keloids. For that reason, we suggest the use of mask straps or head loops aiming to relieve tension from the use of ear hooks, avoid skin irritation and trauma, and ultimately minimize the risk of keloid formation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.