
Abstract
Retiform hemangioendothelioma (RH) is a rare intermediate (locally aggressive) vascular tumor that mostly affects the dermis of the trunk and limbs, but has never been reported in the inferior turbinate. A 10-year-old Chinese boy presented with recurrent epistaxis in his left nasal cavity and anemia for more than 2 years. Radiographic and electronic video laryngoscopic images showed an expansile mass in the left inferior turbinate. Endoscopic surgery and electrocautery were performed to resect the tumor beyond the macroscopic border. Histopathologically, the tissues were infiltrated by hyperplastic blood vessels arranged in a retiform pattern, and endothelial cells proliferate significantly in some areas. Immunohistochemistry showed a positive result for CD31, CD34, Fli-1, and ERG. No epistaxis, tumor recurrence, or metastasis was found on reexamination over 18 months after surgery.
Introduction
Epistaxis is a common emergency in the otolaryngology department. Tumors should be considered in a child with long-term and recurrent epistaxis. Retiform hemangioendothelioma (RH), a rare vascular neoplasm, first reported by Calonje et al 1 in 1994, was classified as an intermediate (locally aggressive) vascular tumor in the latest World Health Organization (WHO) classification. 2 With fewer than 50 cases reported so far, the rarity of RH poses challenges in its diagnosis and treatment. Biopsy remains the only diagnostic method currently available. Complete surgical excision (with or without postoperative chemoradiotherapy) is the most effective therapeutic option.
Case Report
A 10-year-old Chinese boy presented with recurrent epistaxis in his left nasal cavity for over 2 years. Bleeding progressively worsened and led to anemia that was treated with blood transfusion before hospitalization. He had no relevant family history or previous radiotherapy. Physical examination showed pale lips and conjunctiva of the lid. Anterior rhinoscopy revealed bleeding middle and posterior to the left inferior turbinate. The remainder of the physical examination was noncontributory. No positive results were noted in routine laboratory examinations except for the blood test revealed iron deficiency anemia status of red blood cell 2.39 × 109/L, hemoglobin 59 g/L, and mean corpuscular hemoglobin concentration 274 g/L. Hematological examination indicated microcytic hypochromic anemia was probably due to long-term chronic blood loss, the hematology consultation suggested. To find the cause of chronic blood loss, electronic gastroscope and SPECT imaging of ectopic gastric mucosa were carried out considering a history of vomiting blood but no positive signs observed. Computed tomography (CT; Figure 1) and electronic laryngoscope (Figure 2) showed an expansile mass in the left inferior turbinate and partial bone destruction can be found in CT scan. There was no clinical evidence of regional lymph node involvement. Recurrent nasal bleeding was suspected to be the main cause of anemia.

Computed tomography (CT) showed an expansile mass with partial bone destruction in the left inferior turbinate.

Electronic laryngoscope image showed an expansile mass in the left inferior turbinate with local bleeding.
We performed endoscopic surgery under general anesthesia after obtaining his guardian’s consent. We widely resected the tumor beyond borders and adequately cauterized the base of the tumor by bipolar coagulation forceps. Postoperative histopathological examination (Figure 3) showed the tumor, composed of abnormally proliferated blood vessels which arranged in a retiform pattern with significant proliferation in partial areas of endothelial cells, located in the submucosa of nasal cavity. Immunohistochemical stains were positive for CD31, CD34, ERG, and Fli-1, and negative for D2-40. Ki-67 (15%) showed a low proliferation index in tumor cells. Transfusion and supportive treatment were also been performed during the perioperative period and epistaxis subsided after surgery, hemoglobin increased to 98 g/L before discharge. Considering the patient’s age, complete resection, and adequate cauterization of the tumor base, we chose closely follow-up instead of postoperative chemoradiotherapy. He was free of local recurrence and distant metastasis 18 months after surgery.
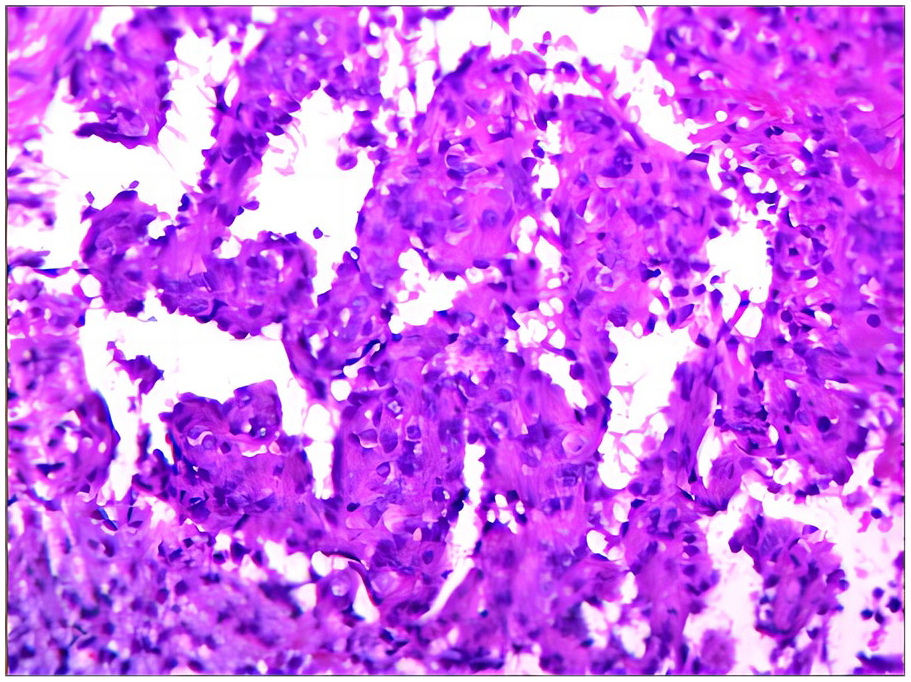
The H&E stain showed the typical characteristics of retiform hemangioendothelioma (surgical specimen, ×100). H&E, hematoxylin and eosin.
Discussion
RH is a slow-growing vascular tumor that affects a diverse age range. Earlier reports have consensus that RH predominantly occurs in young or middle-aged adults (in second-fourth decade of life).3,4 As the number of reports increasing, the age predisposition becomes less pronounced and it can occur in all age groups from infants to the elderly. Moreover, congenital RH has also been reported, 5 which means age preference deserves further exploration.
The etiology of RH remains unknown, but it has been supposed to be associated with lymphedema, 6 previous tumors or radiation exposure,7,8and human herpes virus-8 (HHV-8). 7 We still do not know how much role medical history played in the development of RH. The correlation between them needs to be further analyzed with more cases. Recently, molecular defects of RH with YAP1 and MAML2 gene rearrangements and fusions have been described. 9 It may be a reliable immunohistochemical marker in vascular tumors.
Clinically, RH typically develops as one or more gradually enlarging exophytic cutaneous or subcutaneous nodule or plaque of variable size which may occur in any part of the body but more in the extremities and trunk,6,10-15 few isolated lesions may occur in the head and neck (including scalp, 16 forehead, 17 medial canthus,18-20 mandible, 21 the postauricular region, 22 infratemporal fossa, 23 and paranasal sinus 24 ), vulva, 25 mediastinum, 16 jejunum, 26 spleen, 27 etc. To our knowledge, this is the first report of RH in the turbinate.
Patients with RH have a slow indolent course, may be completely asymptomatic, or present symptoms related to tumor location such as in our patient who presented as recurrent epistaxis. Patients had no associated pain, itching, or swollen lymph nodes in related area. As there are no specific clinical or radiological manifestations, typical histopathological features are essential for diagnosis.
Histopathologically, RH shows vascular proliferation and infiltrative growth with obscure boundary, usually involves the entire dermis, and extends to subcutaneous tissue. The tumor involved tissues composed of distinctive interconnecting arborizing blood vessels lined by hobnail-like endothelial cells and arranged in a retiform pattern resembling normal rete testis, hence the name “retiform.” Neither significant cellular atypia nor mitotic figures were observed in any published reports, means that RH is not completely malignant.
Immunohistochemically, tumor cells lining in the elongated vascular spaces express endothelial markers including CD31, CD34, ERG, and Fli-1. RH responses to factor VIII-related antigen13,28 and HHV-8 7 in some cases. The diagnostic value of these 2 factors in RH is still undefined. Few reported cases have shown that RH is immunoreactive for D2-40,8,17 which is a marker for endothelium of lymphatic vessels. Whether RH responds to D2-40 or not remains controversial.
For the treatment of RH, typically surgical excision with negative margins plays a major role in the accurate diagnosis and local control of most patients, although there is no therapeutic consensus. Radiotherapy and chemotherapy have also proved to be effective in patients with lymph node metastasis, extended tumor size, local recurrence, or tumors not amenable to surgery. Furthermore, Hirsh et al 29 first reported successful treatment of RH with low-dose cisplatin and moderate radiotherapy without surgical resection. Conservative therapy with a combination of pulsed dye laser, local corticosteroid injection, and external application of imiquimod cream is also an acceptable strategy. 30 As for our patient, endoscopic surgery and bipolar cautery resection enable adequate exposure and visualization of tumor, control of bleeding, and complete removal of tumor in nasal cavity. It is difficult to establish a RH treatment guideline because of the limited number of reported cases as of now. Surgical treatments and adjuvant therapies should be carefully considered to avoid unnecessary interventions and potentially severe complications.
RH is prone to local recurrence but rarely metastasis to distant sites, with few reports of regional lymph node metastasis.1,6,31 Almost all reported recurrences are located at or near the primary site, so closely follow-up is highly recommended rather than additional aggressive therapy. In addition, recent cases have reported death of RH patients, in whom tumor progressed rapidly and been lethal. The exact cause of death is unknown, but more related to the special location of tumor where operation cannot be performed, 8 the large tumor invasion area, 32 or serious complications like shock or multiple organ failure.27,33 Overall, the prognosis of RH has individual variation.
In conclusion, RH is a rare slow-growing vascular tumor that can occur in any part of the body and clinically mimic malignancy with a high rate of local recurrence but low metastatic potential. We report the first case of RH occurring in the inferior turbinate of a young boy, and review reports relating to this rare tumor. Histopathological examination proves to be an important diagnostic tool. Further reporting of similar cases and their treatment experiences might give us better insight into pathogenesis and treatment responsiveness of RH.
Footnotes
Acknowledgements
We thank SAGE for the proper English language, grammar, punctuation, spelling, and overall style service.
Data Availability Statement
All data generated or analyzed during this study are included in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was supported by the National Natural Science Foundation of China (32160149), the Key Science and Technology Foundation of Gansu Province (23YFFA0040), and the Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2023-MS-B08).
Ethical Statement
Our institution does not require ethical approval for reporting individual case or case series.
Informed Consent
Written consent was obtained from the patient’s guardian to publish their anonymized information in this article.