
Abstract
Introduction
Sudden sensorineural hearing loss (SSNHL) is defined as deterioration of hearing in at least 3 consecutive audiometric octaves over 30 dB within 3 days. 1 The annual incidence rate of SSNHL is reported to be 5 to 30 per 100,000 persons, and the mean age at onset is in the 40s to 50s, with no sex preference.2,3 SSNHL is uncommon in children and young adults, with pediatric patients (≤18 years of age) accounting for only 6.6% of the total incidence of SSNHL. 4 In children with SSNHL, the age at onset is typically 12 to 13 years, with equal incidence in girls and boys; 54.3% to 88.1% of these patients have been reported to present with severe (61-80 dB) to profound (>80 dB) hearing loss.5,6 SSNHL has dramatic adverse effects on the young population, such as speech and learning difficulties, impairment of social interactions, psychological problems, and reduced quality of life.
Paradoxical embolism refers to the migration of emboli from the vena cava to the systemic circulation through right-to-left shunting (RLS), which is caused by a cardiogenic passageway [eg, patent foramen ovale (PFO)] or a noncardiogenic channel (eg, pulmonary arteriovenous fistula). Cryptogenic stroke originating from RLS is more common in the young than in the old, 7 and paradoxical embolism is one of the most common causes of cryptogenic stroke in children and young adults.8-11 The labyrinthine artery is a narrow terminal branch of the anterior inferior cerebellar artery or vertebrobasilar artery, and has no vascular collaterals; thromboembolism of the anterior inferior cerebellar artery or vertebrobasilar artery is a widely accepted etiology for SSNHL.3,12-15 After reading the literature, we found that only 3 studies of adults have reported the relationship between paradoxical embolism and SSNHL. However, to our knowledge, the role of paradoxical embolism in the pathogenesis of SSNHL in children and young individuals has not yet been reported. Therefore, this study aims to preliminarily explore the impact of paradoxical embolism on SSNHL onset in juveniles and young adults. Ethics approval for this study was granted by the institutional review board and the medical ethics committee of Peking Union Medical College Hospital (No. K3027).
Patients and Methods
We consecutively enrolled young patients (<35 years) with severe-to-profound SSNHL who visited the Department of Otorhinolaryngology of Peking Union Medical College Hospital between August 2021 and September 2022. SSNHL was defined as deterioration of hearing in at least 3 consecutive audiometric octaves over 30 dB within 3 days. 1 The average hearing thresholds at 0.5, 1, 2, and 4 kHz were evaluated using pure-tone audiometry (PTA). Severe deafness was defined as 61 to 80 dB HL and profound hearing loss as >80 dB HL. The exclusion criteria were syndromic deafness, detectable triggers for SSNHL (eg, viral or bacterial infection, congenital inner ear malformation, autoimmune diseases, noise exposure, trauma, barotrauma, and ototoxic drugs), and high-risk factors for thromboembolic events (eg, diabetes, hypertension, history of deep vein thrombosis, and hypercoagulable state). All patients underwent contrast transcranial Doppler ultrasonography (c-TCD; TCD-2000S, Chioy, China) with a mixture of 9 mL normal saline and 1 mL air, as described in the literature. 16 RLS was defined as the presence of more than air bubble (microemboli) in the middle cerebral artery on c-TCD after the rapid bolus injection of the air/saline solution. The c-TCD grading standard for RLS was as follows: (1) grade 0, no microbubbles detected; (2) grade 1, 1 to 10 microbubbles; (3) grade 2, more than 10 microbubbles, noncurtain type; and (4) grade 3, embolic signals of curtain or shower type. 16 Contrast transthoracic echocardiography (c-TTE; EPIQ 7C, Philips Medical Systems, Netherlands) was used to detect PFO-RLS by observing microbubbles in the left atrium within 3 cardiac cycles and pulmonary arteriovenous fistulas (pulmonary-RLS) after 4 cardiac cycles, during the strain or release phase of the Valsalva maneuver.17-19 All patients underwent head magnetic resonance imaging (MRI) to detect structural abnormalities and tumors of the auditory pathway, and 6 patients underwent whole-exome sequencing to screen for common deafness-related genes.
Corticosteroids (systemic followed by intratympanic), Ginkgo biloba extract, batroxobin, and hyperbaric oxygen were routinely administered for 1 month to all patients within 3 days after the onset of SSNHL, according to the Chinese guidelines for the treatment of SSNHL. 20 Hearing recovery was divided into 4 levels: (1) complete recovery, final hearing <25 dB HL; (2) partial recovery, final hearing between 25 and 45 dB HL with hearing gain ≥15 dB; (3) slight recovery, final hearing >45 dB HL with hearing gain ≥15 dB; and (4) no improvement, hearing gain <15 dB. 21
Results
Demographic and Test Characteristics
Eight patients with severe-to-profound SSNHL under 35 years of age visited our hospital. One patient was excluded due to a hypercoagulable state, though his c-TCD showed the presence of RLS. The remaining 7 patients (1 male patient and 6 female patients) were enrolled in the present study. Among these, 5 patients were juveniles (≤18 years old), and 2 were young adults (19-35 years old). The average age of the patients was 19.4 ± 6.5 years. The left ear was affected in 5 patients, while the right ear was affected in 2 patients. Except for a young female with migraine since adolescence and a family history of migraine, none of the other patients had a history of chronic or hereditary medical diseases. No precipitating factors for SSNHL were detected in any of the patients. The most common accompanying symptoms were tinnitus and vertigo. A 15-year-old female also had headache and amaurosis attacks at the onset of SSNHL. Three patients had severe hearing loss, and the other 4 patients had profound hearing loss. The average PTA threshold at the time of SSNHL onset was 86.8 ± 16.7 dB HL. After receiving the standard therapy for SSNHL for 1 month, 2 patients made a complete recovery; 3 patients had slight improvement; and another 2 patients showed no improvement after a mean follow-up period of 10.1 ± 11.7 months. Of the 6 patients who underwent whole-exome sequencing, none had known deafness gene variations, and no patient had abnormalities on head MRI.
RLS was confirmed in all patients through c-TCD: 3 patients had grade-3 RLS (curtain or shower type); 2 patients had grade-2 RLS (>10 microbubbles); and 2 patients had grade-1 RLS (1-10 microbubbles). In one patient with grade-1 RLS, numerous microbubbles were observed within 3 cardiac cycles on c-TTE, indicating the presence of a large PFO. A patient with grade-2 RLS was found to have numerous air bubbles on c-TTE after 6 cardiac cycles, suggesting the presence of a pulmonary arteriovenous passage. In one patient, PFO was found by cardiac catheterization; this patient underwent surgery to occlude the interatrial defect. The detailed clinical information of the patients is shown in Table 1.
Detailed Clinical Information of Patients With Severe-to-Profound Sudden Sensorineural Hearing Loss.
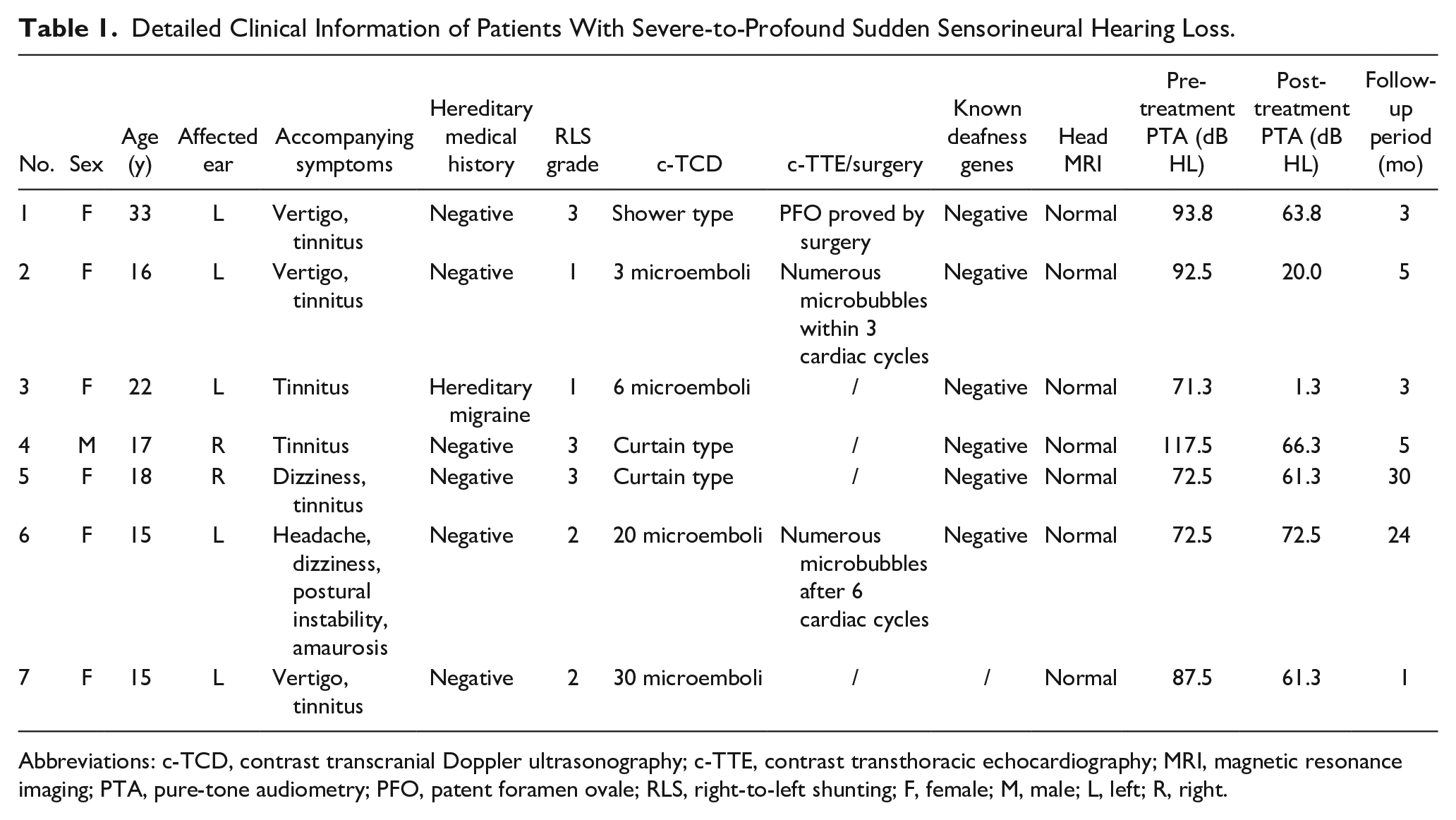
Abbreviations: c-TCD, contrast transcranial Doppler ultrasonography; c-TTE, contrast transthoracic echocardiography; MRI, magnetic resonance imaging; PTA, pure-tone audiometry; PFO, patent foramen ovale; RLS, right-to-left shunting; F, female; M, male; L, left; R, right.
Typical Cases
Patient no. 1
A 33-year-old female developed sudden deafness in the left ear with vertigo and tinnitus 4 months ago. She had no relevant medical history and no obvious precipitating cause for SSNHL. The average PTA threshold in her affected ear was 93.8 dB HL. Numerous microbubbles (shower type, grade-3 RLS) were noted passing through her middle cerebral artery on c-TCD (Figure 1). No wave of auditory brainstem response was elicited at 95 dB HL, and both the cervical and ocular vestibular-evoked myogenic potentials showed no abnormalities on her affected ear. She underwent cardiac catheterization in the Department of Cardiac Surgery, which revealed a 1 mm PFO. Subsequently, she underwent surgical closure of the PFO to prevent future ischemic stroke. Standard medication for SSNHL was prescribed for 1 month, including batroxobin, corticosteroids, Ginkgo biloba extract, and hyperbaric oxygen therapy. Her hearing recovered slightly, with a hearing gain of 30 dB.
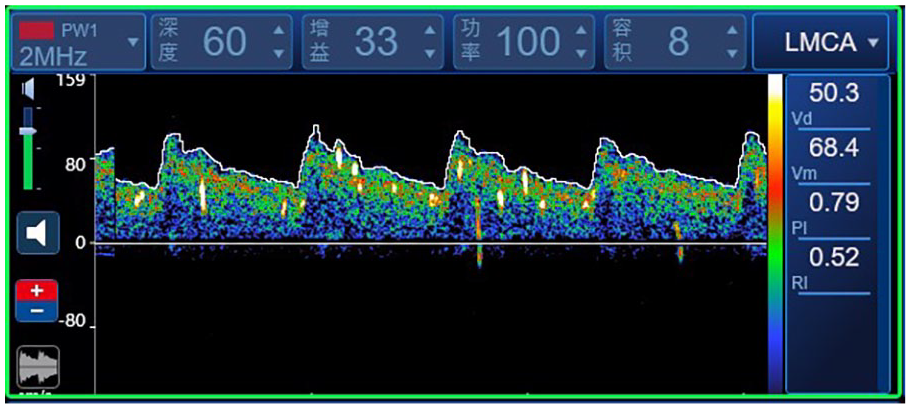
Contrast transcranial Doppler screenshots of patient no. 1. Each bright spot indicates an air bubble. The air bubbles present in the cerebral artery are of the shower type.
Patient no. 6
A 15-year-old female developed severe SSNHL in the left ear 2 years ago. At the time of SSNHL onset, she also developed intermittent attacks of dizziness, postural instability, amaurosis, and tingling headaches involving the frontal, occipital, and temporal regions, which were often triggered by physical exercise and lasted for 2 to 3 minutes. The c-TCD examination showed more than 20 air bubbles passing through the middle cerebral artery (grade-2 RLS; Figure 2). On c-TTE, we detected 15 to 20 microbubbles at rest and 20 to 25 microbubbles when performing the Valsalva maneuver in the left atrium after 6 cardiac cycles, supporting the presence of a pulmonary arteriovenous fistula. Despite standard treatment for 1 month, she had no hearing recovery at her 24 month follow-up.
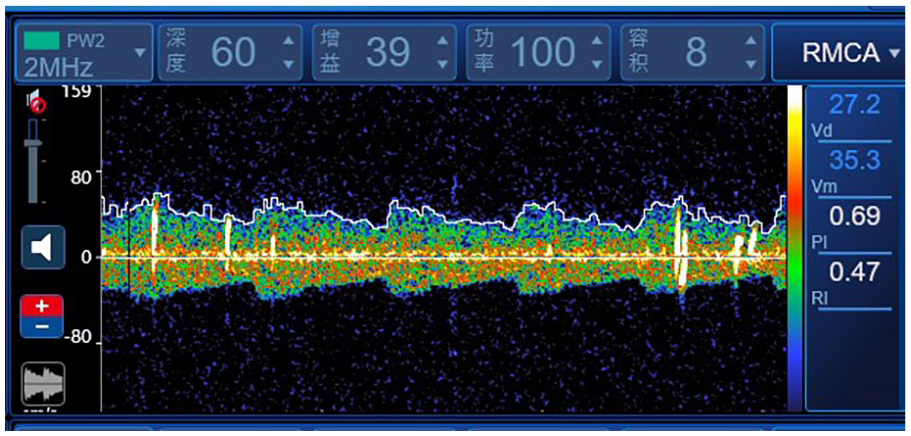
Contrast transcranial Doppler screenshots of patient no. 6. Each bright spot indicates an air bubble. Twenty air bubbles are seen passing through the cerebral artery, indicating grade-2 right-to-left shunting.
Discussion
The annual incidence of ischemic stroke in children is reported to be 1.2 to 2.5 per 100,000,22-25 and cardioembolic diseases account for a quarter of all pediatric strokes, with RLS being the foremost reason. 26 The mechanism of RLS predisposing to ischemic diseases is possibly due to the migration of emboli from the venous system directly to the systemic circulation; in addition, the slow or stagnant blood flow at the loci of right-to-left shunts predisposes to thrombus formation. The labyrinthine artery, a functional end-artery, supplies blood to the inner ear. Cochlear function is highly susceptible to blood pressure fluctuations and impairments of the labyrinthine artery. If thrombosis occludes the labyrinthine artery, severe vertigo and profound hearing loss may occur. 27 Emboli entering the systemic circulation via RLS can theoretically lead to embolism of the labyrinthine artery, and cause cochlear injury as well as sudden deafness, as suspected in studies of RLS in adults with sudden deafness. Ciorba et al found that paradoxical embolism through a 0.5 mm PFO was highly suspiciously associated with the incidence of SSNHL in a 54-year-old man. 28 Iguchi et al (n = 23) and Capuano et al (n = 40) both found that half of their adult patients with SSNHL had RLS, and that patients with RLS were significantly younger than those without RLS, suggesting that RLS may play a more important role in SSNHL in the young than in the old.27,29
The c-TCD, c-TTE, and contrast transesophageal echocardiography (c-TEE) with the Valsalva maneuver are primary examinations to detect RLS by showing microemboli in the middle cerebral artery or left chamber with high sensitivity (>90%).30-33 Of these, c-TEE is an invasive method with some disadvantages such as low compliance and cardiac, pulmonary, and bleeding complications. 34 In contrast, c-TCD and c-TTE are noninvasive and better tolerated by patients. It has been reported that c-TCD has a higher sensitivity than c-TTE to detect PFO-RLS, 35 as c-TTE images may shift during the Valsalva maneuver. 36 Thus, in the present study, considering the compliance and tolerance of young patients, especially children, we chose c-TCD as the primary method to detect RLS. We used c-TTE as a complementary examination to further discriminate PFO-RLS from pulmonary-RLS. Among our patients, only 2 patients agreed to undergo c-TTE; microemboli were detected within 3 cardiac cycles in patient no. 2, indicating the presence of PFO-RLS, and after 6 cardiac cycles in patient no. 6, suggesting pulmonary-RLS. Distinguishing PFO-RLS and pulmonary-RLS is meaningful for future treatments, such as a PFO-closure surgery. Although the qualitative nature of c-TCD in detecting RLS is reliable, its quantitative ability to assess the RLS size is not completely accurate, as the results of c-TCD may be affected by unavoidable methodological factors, such as patient position and individual hemodynamics. It has been reported that c-TCD has a higher efficacy for indicating large RLS than small RLS.37-38 In the present study, only 3 air bubbles were detected on c-TCD in patient no. 2, but numerous microbubbles were noted on c-TTE, suggesting the semiquantitative nature of c-TCD and supporting the complementary function of c-TTE in assessing RLS size. The c-TCD results indicated grade-3 RLS in 3 of our patients, grade-2 RLS in 2 patients, and grade-1 RLS in 1 patient (patient no. 2, who was finally found having numerous microemboli in c-TTE, indicating a large RLS). The magnitude of the RLS is positively related to the incidence of cryptogenic stroke, and large RLS is associated with a high risk of paradoxical embolism. 39 Thus, it is reasonable to presume that large RLS increases the risk of severe-to-profound SSNHL in young patients, and suggest that the present patients had a relatively high risk of developing paradoxical embolism due to the presence of large RLS.
Paradoxical embolism from RLS was considered to be the most probable cause of SSNHL in the young patients in this study, owing to the following considerations and evidence. First, all the young individuals developed severe-to-profound SSNHL, which is highly related to circulatory disturbance. 27 Second, all the patients were confirmed to have RLS through c-TCD, and most patients had large RLS with a high risk of developing paradoxical embolism leading to embolism of the labyrinthine artery and severe-to-profound SSNHL as explained above. Third, none of the patients had any predisposing factors for SSNHL, including viral or bacterial infection, autoimmune diseases, metabolic disease, congenital inner-ear abnormality, noise exposure, trauma, barotrauma, tumor, ototoxic drugs, Meniere’s disease, and previous hearing loss. Other common cardioembolic diseases or arterial ischemia, like atrial fibrillation or flutter, infective endocarditis, vasculitis, and hypercoagulability, were also excluded. Hence, a circulation defect of the labyrinthine or cochlear artery was considered to be the most possible cause of severe-to-profound SSNHL in these young individuals.
In the literature, the reported rates of complete recovery and any recovery after SSNHL are 20.7% to 29.4% and 49.0% to 67.6%, respectively, in adults, 40 and 9.3% to 26.9% and 37.7% to 55.3%, respectively, in children.6,41,42 Capuano et al reported that 20% of adults diagnosed with SSNHL accompanied with RLS had good hearing recovery (within 15 dB of the unaffected contralateral ear), and 40% had fair recovery (more than 10 dB of hearing gain, but did not return to within 15 dB of the unaffected ear). 29 The patient described by Ciorba et al experienced no hearing improvement after treatment. 28 Consistent with the aforementioned results, in this study, 2 young patients had complete hearing recovery; 3 had slight improvement; and 2 had no improvement after therapy. It seems that the recovery rate of SSNHL in patients with RLS is similar to that in SSNHL patients without RLS. Future studies with a larger sample size may draw more concrete conclusions. The mean follow-up period in this study was 10.1 ± 11.7 months, during which time no further improvement was observed in patients with continued hearing impairment, which adversely affected the young patients’ daily activities.
There are some limitations to this study. First, it was difficult to definitively prove that paradoxical embolism was the cause of severe-to-profound SSNHL owing to a lack of direct and objective tools to observe the labyrinthine artery. Second, c-TTE was not conducted in all the young patients, considering their willingness and compliance. Third, the sample size was relatively small, due to the low morbidity of SSNHL in the young adults and the strict inclusion and exclusion criteria. The small sample size might lead to a selection bias, and further research is needed to verify the results of this study.
Conclusions
Paradoxical embolism from RLS is a possible cause of severe-to-profound SSNHL in children and young adults. Paradoxical embolism should be considered when a young patient presents with idiopathic severe-to-profound SSNHL. The c-TCD is recommended to screen for the existence of RLS, and c-TTE should be considered as a complementary examination to assess the RLS size or further discriminate PFO-RLS from pulmonary-RLS.
Footnotes
Acknowledgements
We would like to thank all the patients for allowing us to review their medical findings and records.
Author Contributions
Huiying Sun drafted the initial manuscript and completed the statistical analysis. Ruizhe Yang, Xu Tian, and Yang Zhao collected the data. Yuchen Yang critically reviewed the manuscript. Haiyan Wu and Zhiqiang Gao designed the study, reviewed, and revised the manuscript. All authors read and approved the final manuscript.
Consent for Publication
All authors read and approved the final manuscript.
Data Availability Statement
The data generated during the current study are available from the corresponding author on a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National High Level Hospital Clinical Research Funding (2022-PUMCH-C-041) and Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2023-RW320-03) and Beijing Natural Science Foundation (7222313).
Ethics Statement
Ethics approval was granted by the Institutional Review Board (IRB) and the Medical Ethics Committee of Peking Union Medical College Hospital (No. K3027).
Participants’ Informed Consent
The study was conducted according to established ethical guidelines, and informed consent was obtained from the participants.