
Abstract

Significance Statement
Dysphonia plica ventricularis is the pathological interference of false vocal folds in phonation. It usually is associated with severe muscle tension in the laryngeal area, which can be a result of functional voice disorders. Voice therapy is the standard treatment, and psychological therapy is necessary in some cases. Cognitive behavioral therapy is the primary modality of psychotherapy treatment. Hypnotherapy also can be effective and should be considered as an alternative adjunctive treatment.
Case Presentation
A 67-year-old male with a history of anxiety presented with sudden onset of dysphonia that had started 15 months prior to our initial evaluation. His voice was severely strained. Laryngeal examination showed severe muscle tension dysphonia with dysphonia plica ventricularis (DPV; Figure 1). Laryngeal examination during inhalation, which eliminates false vocal fold contact, further demonstrated presbylarynx, glottic insufficiency, and a left vocal fold scar (Figure 2). Laryngeal electromyography revealed mild bilateral superior laryngeal nerve paresis. The patient underwent extensive voice therapy, including the usual approaches and inhalation phonation exercises, without success. He then underwent left vocal fold fat implantation for scar followed by extensive postoperative voice therapy sessions, but he was still unable to use his true vocal folds to phonate.
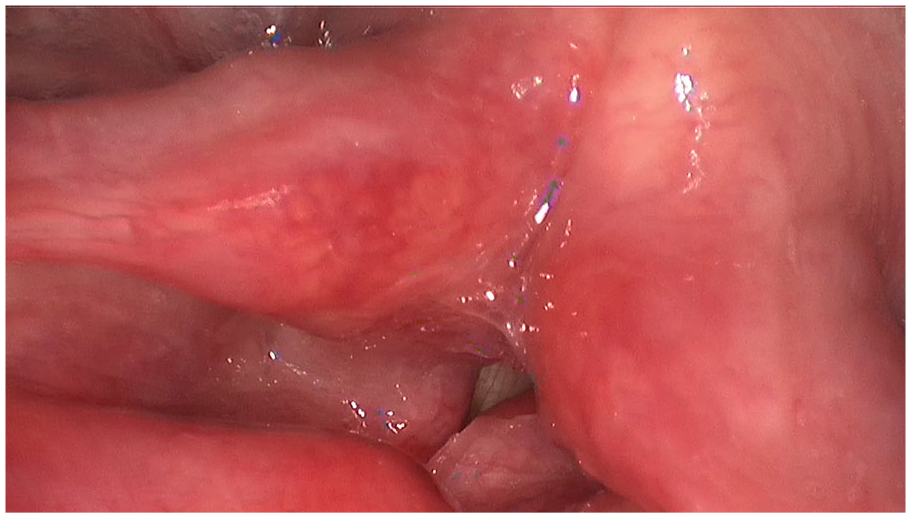
Laryngeal examination showing dysphonia plica ventricularis.
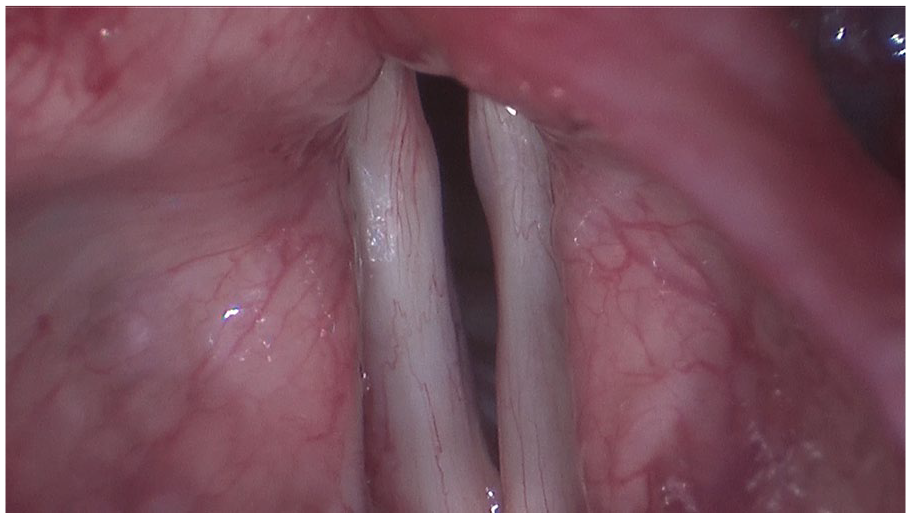
Laryngeal examination during inhalation showing presbylarynx, glottic insufficiency, and left vocal fold scar.
At that point, 2 options were discussed with the patient: (1) botulinum toxin injection of the false vocal folds and supraglottic muscles and (2) hypnotherapy. We encouraged hypnotherapy which he accepted hoping that it also might help his anxiety. Substantial improvement in his voice was noted after 3 hypnosis sessions (Figure 3).
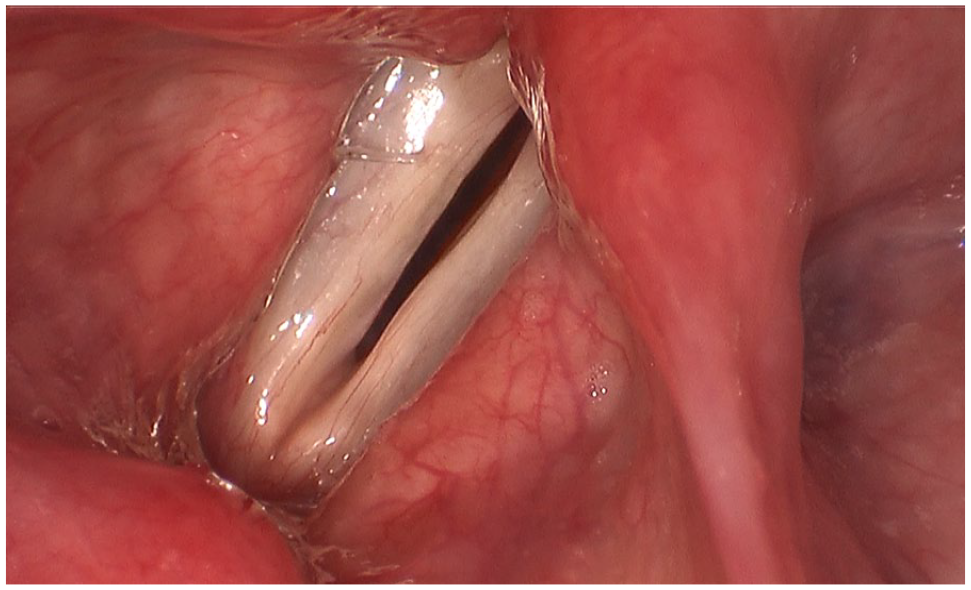
Laryngeal examination after hypnosis showing true vocal fold phonation without false vocal fold approximation, but with glottic insufficiency.
Later, the patient underwent bilateral, left greater than right, vocal fold fat injection that improved his glottic closure and decreased phonatory effort.
Discussion
DPV, also known as ventricular dysphonia, occurs when the false vocal folds approximate and interfere with phonation by true vocal fold vibration. 1 It often presents with a low-pitched voice, hoarseness, strain, and restricted voice range. 2 It can result as a compensatory mechanism for severe true vocal fold disease such as true vocal fold paralysis, vertical hemilaryngectomy, congenital anomalies, and invasive tumors. 2 However, it is most commonly caused by severe muscle tension in the laryngeal area. 1 Such excessive tension has been associated with organic voice disorders such as habitual voice abuse/misuse, hormonal changes, laryngopharyngeal reflux, aging, and others; and to functional voice disorders associated with psychological and personality factors such as anxiety, depression, stress, neuroticism, and introversion. 3 A multidimensional evaluation focusing on the patient’s history and psychosocial stressors is an essential part of the diagnostic process. Laryngoscopy, videostroboscopy, videofluoroscopy, laryngeal electromyography, flexible nasolaryngoscopy, aerodynamic analysis, and acoustic analysis also may be helpful in the workup. First-line treatment is typically voice therapy to decrease hyperinflation and restore healthy true vocal fold phonation. Refractory cases may be helped by psychotherapy, anesthetic injections, botulinum toxin injections, and rarely surgical resection of false vocal folds. 2 However, the senior author (RTS) generally is opposed to false vocal fold resection because of the resultant changes in laryngeal physiology; and he has never found it necessary in clinical practice. There is no role for pharmaceutical management currently, but if the DPV occurs as the result of a psychiatric condition, psychotropic medications may be utilized. Also, if the DPV is compensatory in response to a medical condition, pharmaceutical treatment of the underlying condition is appropriate.
Psychotherapy is especially effective for patients with a psychogenic etiology of DPV. Cognitive behavioral therapy is the most commonly utilized form of psychotherapy and incorporates techniques such as assertiveness training, alternative coping strategies, and awareness of social communication.2,4,5 Hypnotherapy is a form of psychotherapy that focuses on deep relaxation techniques to induce a state of heightened focus, concentration, and suggestibility. 6 While there are reports of hypnotherapy as a successful treatment for psychogenic dysphonia,7,8 none have been described specifically for the treatment of DPV. Here we present the first reported case of DPV successfully treated with hypnotherapy, although the senior author has used this approach successfully on other patients. Given that hypnotherapy is effective and noninvasive, it should be considered as an alternative treatment option for selected patients with DPV who do not respond to expert voice therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.