
Abstract
Significance Statement
Laryngomalacia is characterized by dynamic obstruction of the upper airway. Early detection using dynamic observation across the respiratory cycle helps assume accurate diagnosis and effective management. We present a case of laryngomalacia that mimicked characteristics of subglottic stenosis which could have resulted in unnecessary surgery.
Laryngoscopic Clinic
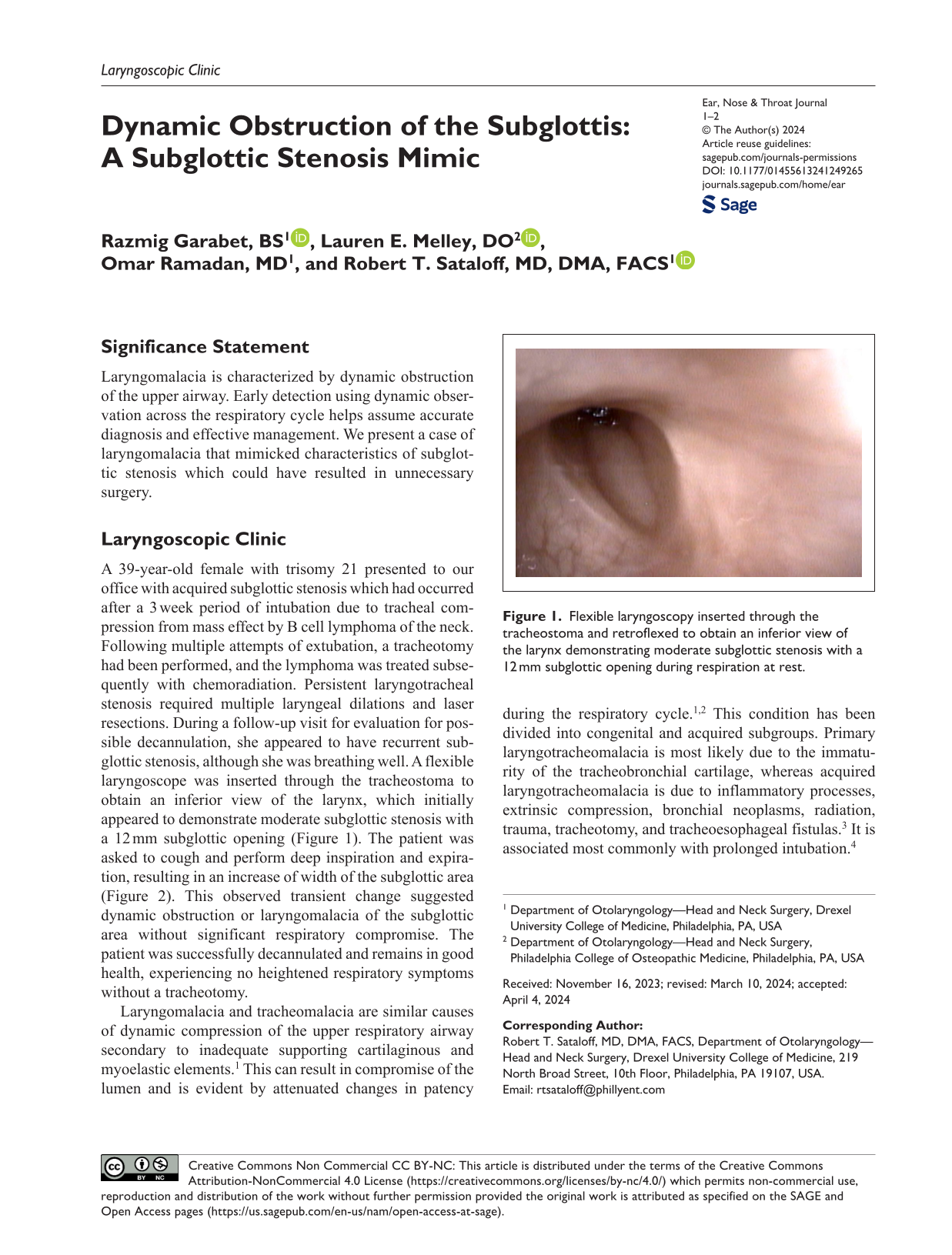
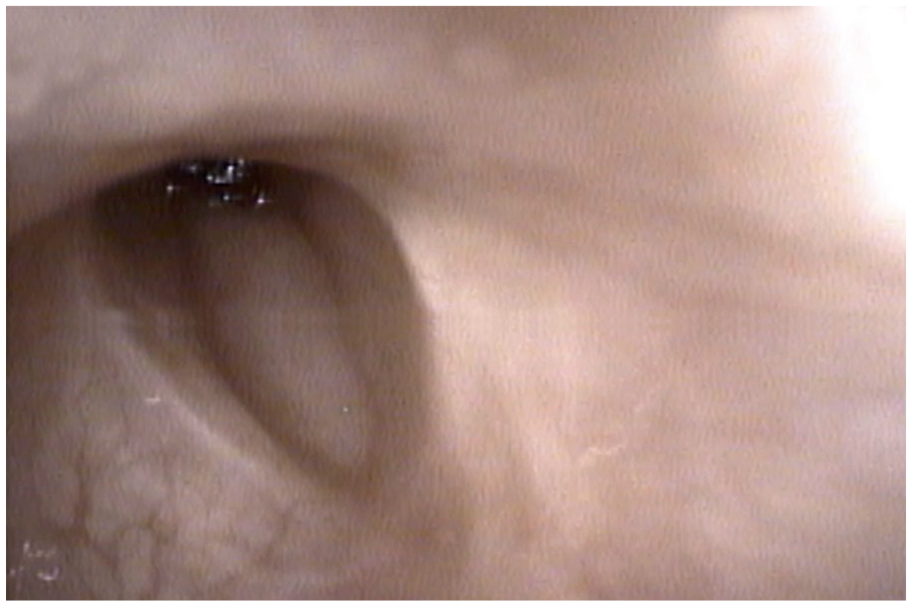
A 39-year-old female with trisomy 21 presented to our office with acquired subglottic stenosis which had occurred after a 3 week period of intubation due to tracheal compression from mass effect by B cell lymphoma of the neck. Following multiple attempts of extubation, a tracheotomy had been performed, and the lymphoma was treated subsequently with chemoradiation. Persistent laryngotracheal stenosis required multiple laryngeal dilations and laser resections. During a follow-up visit for evaluation for possible decannulation, she appeared to have recurrent subglottic stenosis, although she was breathing well. A flexible laryngoscope was inserted through the tracheostoma to obtain an inferior view of the larynx, which initially appeared to demonstrate moderate subglottic stenosis with a 12 mm subglottic opening (Figure 1). The patient was asked to cough and perform deep inspiration and expiration, resulting in an increase of width of the subglottic area (Figure 2). This observed transient change suggested dynamic obstruction or laryngomalacia of the subglottic area without significant respiratory compromise. The patient was successfully decannulated and remains in good health, experiencing no heightened respiratory symptoms without a tracheotomy.
Flexible laryngoscopy inserted through the tracheostoma and retroflexed to obtain an inferior view of the larynx demonstrating moderate subglottic stenosis with a 12 mm subglottic opening during respiration at rest.

Flexible laryngoscopy inserted through the tracheostoma and retroflexed to obtain an inferior view of the larynx demonstrating increased of width of the subglottic area when patient asked to cough and to inhale and exhale deeply.
Laryngomalacia and tracheomalacia are similar causes of dynamic compression of the upper respiratory airway secondary to inadequate supporting cartilaginous and myoelastic elements. 1 This can result in compromise of the lumen and is evident by attenuated changes in patency during the respiratory cycle.1,2 This condition has been divided into congenital and acquired subgroups. Primary laryngotracheomalacia is most likely due to the immaturity of the tracheobronchial cartilage, whereas acquired laryngotracheomalacia is due to inflammatory processes, extrinsic compression, bronchial neoplasms, radiation, trauma, tracheotomy, and tracheoesophageal fistulas. 3 It is associated most commonly with prolonged intubation. 4
Direct visualization of the airway during respiratory cycles is the gold standard for diagnosis; however, dynamic multidetector CT evaluation also may be utilized for noninvasive diagnostic assessment.5,6 The disease course is typically benign and managed conservatively. Muscarinic antagonists such as inhaled ipratropium may be used as pharmacologic therapy to improve smooth muscle tone and respiratory mechanisms. 7 Continuous positive airway pressure may compensate for dynamic collapse and tracheoplasty and silicone stents may be helpful for more severe cases. 7 Management of patients with laryngotracheomalacia should be individualized, with the goal of improving airway integrity and reducing respiratory distress as needed.
The patient in this case had multiple known risk factors for laryngomalacia such as external compression from the lymphoma (which was inferior to the site of her laryngomalacia), chemoradiation, prolonged period of intubation, and presence of tracheotomy. Individuals with trisomy 21 may present with airway anomalies and a decreased tracheal diameter. 8 A notable proportion of this population has airway diagnoses such as laryngomalacia, tracheobronchomalacia, and symptomatic subglottic stenosis. 9
The condition mimicked subglottic stenosis during laryngoscopy and the diagnosis was not established until a flexible laryngoscope was used to observe the lesion from an inferior view and dynamic lumen changes were seen in association with respiration. Furthermore, this patient’s multiple surgeries for subglottic stenosis may also have assisted in managing the dynamic airway changes that had not been recognized until after her severe laryngotracheal stenosis had been corrected. For instance, the patient had undergone placement of Montgomery T-tube (Boston Medical Products Inc) which contributed to consistent airway patency. Once the lumen stenosis was corrected, the dynamic collapse could be identified and was determined to be asymptomatic.
This current case demonstrates the necessity of maintaining laryngomalacia in the differential diagnosis in patients presenting with characteristics of subglottic stenosis. Dynamic observation of the upper airway throughout the respiratory cycle is essential for diagnosis. Early diagnosis of acquired laryngomalacia may allow for conservative management and avoidance of surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.