
Abstract
Subperiosteal orbital hematoma secondary to sinusitis is rare. Thus far, 19 cases of this disease have been reported, of which none involved postoperative skin anesthesia in the region innervated by the supraorbital nerve. In this article, for the first time we report a case of subperiosteal orbital hematoma secondary to sinusitis with skin anesthesia in the area innervated by the supraorbital nerve after surgery.
Introduction
Subperiosteal orbital hematomas can be categorized as either traumatic or nontraumatic, of which the latter are infrequent. Common symptoms prompting patients to seek emergency department care include periorbital pain, swelling, exophthalmos, and diminished vision. In the existing literature, spontaneous hematomas have been attributed to acute and chronic sinusitis, hemorrhagic diseases, elevated intracranial venous pressure, and orbital vascular malformations. However, as a causative factor sinusitis is exceptionally uncommon in comparison with other etiologies. When patients present with related symptoms, it is imperative that clinicians consider the possibility of spontaneous orbital hematoma associated with sinusitis, as well as investigating potential causes such as trauma, hematological disorders, cardiovascular conditions, and other diseases. This is crucial so that patients can receive appropriate treatment and achieve a favorable prognosis.
Case Report
A 41-year-old male presented to our clinic with a history of 11 days of left frontal and periorbital pain that had worsened for 1 day without fever. Computed tomography (CT) scan showed soft tissue shadow in the left frontal and ethmoid sinuses (Figure 1A and B). Antibiotics and analgesic treatment were ineffective. The patient experienced severe pain, and he developed left periorbital edema several hours after the visit (Figure 2A). Visual acuity and eye movement were normal. Because neurogenic edema caused by periorbital cellulitis or painful stimulation was suspected, endoscopic sinus drainage was performed promptly, and the patient’s pain disappeared after surgery. Two days after the operation, the periorbital swelling had not subsided, and the intraocular pressure was 30.7 mmHg. Orbital CT scan revealed a subperiosteal lesion in the roof of the left orbit (Figure 1C and D). After 2 days, the swelling had not significantly improved. Magnetic resonance imaging (MRI) T1-weighted images (T1WI) showed a low signal intensity lesion in the left supraorbital area, and T2-weighted images (T2WI) showed intermediate signal intensity (Figure 1E and F). Considering the large extent of the orbital lesion, endoscopic orbital decompression was performed. After dissection between the lamina papyracea and orbital periosteum, dark blood and clots were drained (Figure 2B-D). The final diagnosis was subperiosteal orbital hematoma combined with sinusitis. After surgery, the periorbital swelling subsided significantly, with normal visual acuity and eye movement (Figure 3). Two days after the second operation, the patient developed skin anesthesia in the area innervated by the left supraorbital nerve (Figure 4A). Orbital MRI showed edema in the tissues surrounding the superior orbital nerve (Figure 4B), which gradually decreased during subsequent treatment. Two weeks after the operation, the periorbital swelling subsided (Figure 5A). One month after the operation, MRI showed that the periorbital edema had disappeared and the hematoma did not recur (Figure 5B and C).
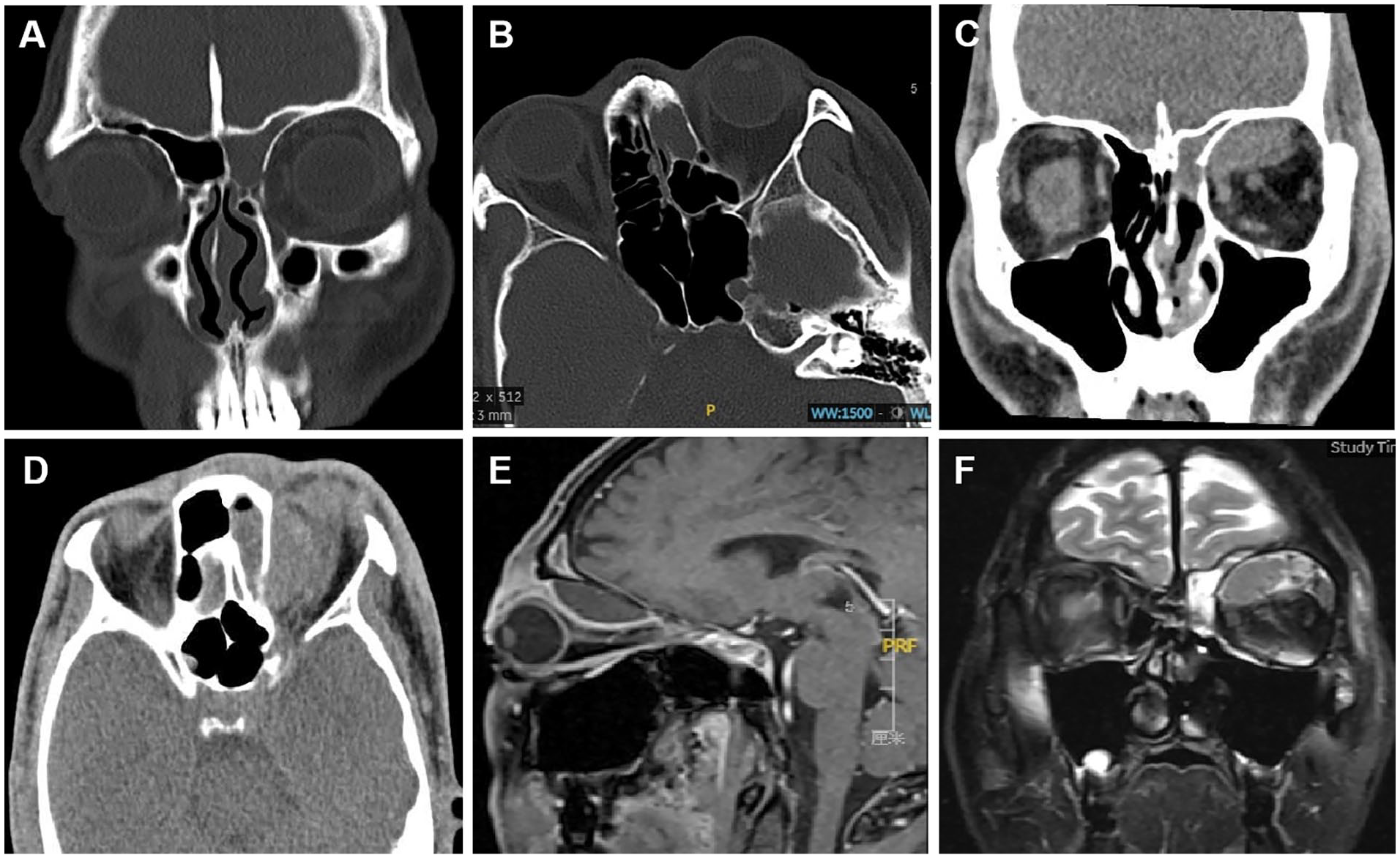
(A and B) The first preoperative CT scan. Soft tissue shadow in the left frontal and ethmoid sinuses. (A) Coronal plane; (B) axial plane (C and D) the second preoperative CT. A well-demarcated biconvex nonenhancing soft tissue density lesion in the left supraorbital area. And the lesion had displaced the upper rectus muscle. (C) Coronal plane; (D) axial plane; (E and F) the second preoperative MRI. (E) T1WI showed a low signal intensity lesion in the left supraorbital area. (F) T2WI showed an intermediate signal intensity. CT, computed tomography; MRI, magnetic resonance imaging; T1WI, T1-weighted images; T2WI, T2-weighted images.

(A) The first preoperative photograph. Photograph of patient showed left-sided swelling and proptosis. (B-D) Intraoperative endoscopic views. (B) After removal of the orbital cardboard, dark red fluid was drained. (C) After the bloody discharge was cleared, blood clot was seen. (D) After removing dark red fluid and blood clots.

Two days after the second surgery, the patient had reduced periorbital edema and normal eye movements.
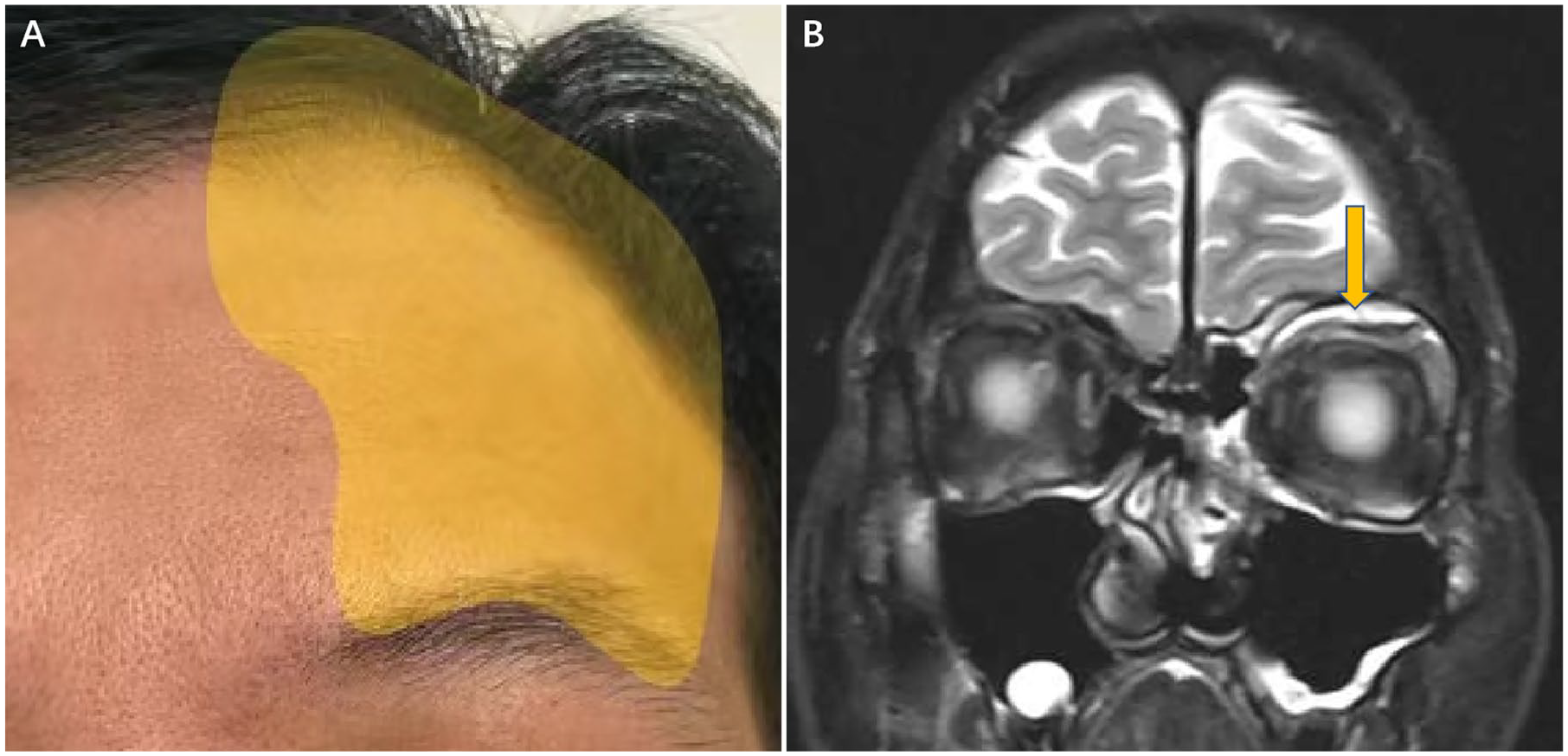
(A) The yellow coverage area was the range of skin anesthesia in patients. (B) The second postoperative MRI showed edema in the tissues surrounding the superior orbital nerve. The linear hypointense shadow indicated by the arrow indicated the trajectory of the supraorbital nerve. MRI, magnetic resonance imaging.
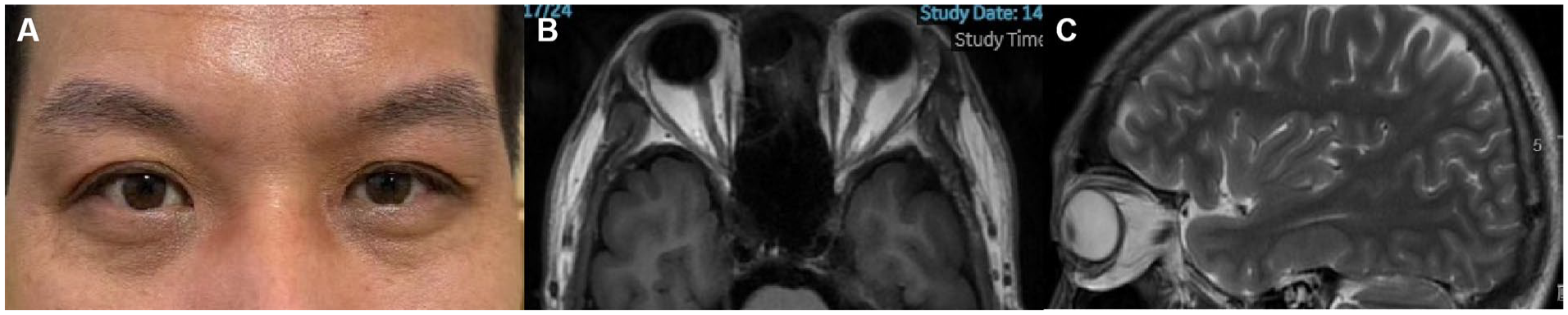
(A) Two weeks after the second surgery, the patient’s periorbital swelling had subsided. (B and C) One month after the second surgery MRI, the patient’s periorbital swelling had subsided. MRI, magnetic resonance imaging.
Discussion
According to the modified Chandler classification, orbital complications of sinusitis are divided into 5 types: preseptal cellulitis, orbital cellulitis, subperiosteal abscess, orbital abscess, and cavernous sinus thrombosis. Currently, subperiosteal orbital hematoma is not included. 1 Since the disease was first reported in 1937, 19 cases of subperiosteal orbital hematoma secondary to sinusitis have been reported. 2,3 The pathogenesis is considered to comprise phlebitis caused by inflammation of the sinus mucosa, which extends to the subperiosteal orbital veins and causes vascular rupture. 4 The clinical symptoms of the disease include periorbital pain, swelling, ocular proptosis, and impaired vision, which are often difficult to distinguish from intraorbital abscesses. Imaging examination plays an important role in differential diagnosis, and CT scan is often the first choice. According to the literature, the radiodensity of an abscess is 30 to 46 Hounsfield units (HUs), whereas that of a hematoma ranges from 40 to 135 HUs. 5 MRI has stronger diagnostic ability than CT, especially for the diagnosis of hematomas, in which it can identify different stages of bleeding. However, the results are affected by the degree of degradation of blood. Acute and subacute hematomas are hyperintense on T1WI and hypointense on T2WI. In the late stage of subacute hematomas, the T2 signal intensifies. When hematomas undergo transformation into chronic forms, the T1 and T2 intensities gradually decrease over time. Diffusion-weighted imaging is a sensitive sequence in which abscesses often exhibit high signal intensity in contrast to hematomas. 4 At present, there are 3 treatment options for subperiosteal orbital hematomas: conservative observation, needle aspiration, and surgical treatment. The existing opinion is that conservative treatment incurs the risk of optic nerve injury. Needle aspiration is not the best choice for patients with sinus infections, and this method cannot effectively remove blood clots. In most cases, aggressive treatment with surgery is best. 1,2 In existing literature reports, surgical approaches include transorbital incision through the eyebrow arch and the endoscopic transnasal approach, of which the former is the most common. With the gradual popularization of endoscopic technology, we believe that the endoscopic transnasal approach is worth recommending for lesions in the superior orbital region, as it can reduce scarring caused by eyebrow arch incision and also treat sinus lesions simultaneously. In addition to ensuring the complete removal of lesions, attention should be paid to protection of the orbital contents and nerves, and excessive stimulation of normal mucosa should be avoided. In this case, the patient experienced skin anesthesia in the area innervated by the supraorbital nerve after surgery, while the trochlear nerve was not affected. In combination with postoperative MRI, it was considered that the anesthesia was caused by compression of edematous tissue around the supraorbital nerve.
Conclusion
Subperiosteal hematoma secondary to sinusitis is rare in clinical practice. In patients with periorbital swelling, clinicians should pay attention to the possibility of this disease and choose appropriate methods of examination for evaluation, which is crucial for subsequent treatment. If surgical intervention is required, attention should be paid to nerve damage secondary to tissue edema.
Footnotes
Authors’ Note
We declare that the article entitled “Challenges in Diagnosing and Treating Subperiosteal Orbital Hematoma secondary to Sinusitis: A Case” is our original work and has not been submitted for publication nor has it been published in whole or in part elsewhere. We further declare that we are fully aware about the instructions and guidelines of Ear, Nose & Throat Journal and agree to submit this article to this journal. We also declare that the above information given by us is full and correct.
Data Availability
All the relevant clinical data are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Traditional Chinese Medicine of Zhejiang Province Science and Technology plan project (Grant no. 2022ZQ041); National Natural Science Foundation of China (Grant no. 82171157); and The Research Project of Zhejiang Chinese Medical University (Grant no. 2022FSYYZQ04).
Ethics Approval
This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University (2023-YBKS-008-01).
Informed Consent
Written informed consent was obtained from the patient.