
Abstract
Introduction
Eagle syndrome refers to an elongation of the styloid process that leads to a wide array of clinical symptoms. It was first described by Eagle in 1937 and has been continually reported on, with new developments in diagnosis and treatment.1,2 An elongation of the styloid process or calcification of the stylohyoid complex, either congenital or acquired, may lead to Eagle syndrome. 2 It has been documented following tonsillectomies and trauma but may also present independent of these. 3 A wide variety of symptoms may be seen due to compression on local neurovascular structures. This can include the nearby internal and external carotid arteries, vagus nerve, facial nerve, auriculo-temporal nerve, lingual nerve, chorda tympani, glossopharyngeal nerve, and hypoglossal nerve. Symptoms most commonly include pain, a foreign body sensation, and dysphagia. Some present with referred otalgia or temporomandibular joint pain, odynophagia, toothache, mouth ulceration or glossodynia, as well as auditory symptoms. Occasionally neurological symptoms or syncope may be present, and some data suggest an increased risk of transient ischemic attack, stroke, and carotid artery dissection.2-5 Eagle originally found that 4% of patients with an abnormal stylohyoid complex have pain. 1 Some studies have found Eagle syndrome to be more common in women and patients over the age of 40. 4 The epidemiology of Eagle syndrome has been difficult to determine as there is no firm diagnostic criteria. 2
The diagnosis of Eagle syndrome is made based on history, physical examination, and imaging.2,4 Treatment may include conservative therapy or surgical intervention. Conservative therapy involves the use of medications such as non-steroidal anti-inflammatory drugs (NSAIDs) anticonvulsants, and antidepressants. Local injections or physical manipulations may also provide temporary relief but do present some risk. These measures often prove helpful, but effects diminish over time.2,3,6 Surgery is a more definitive way to treat certain cases of Eagle syndrome.2,7 There are a variety of surgical techniques, the most common are cervical and intraoral approaches. The cervical approach provides the best exposure to the styloid process but does leave a cervical scar and carries a risk of damaging the facial nerve, particularly the marginal mandibular branch, due to the approach and dissection down to the styloid process.2,8 The intraoral approach through the tonsillar fossa allows for no external scar but visualization is often suboptimal due to incomplete exposure of styloid process and limited ability to manipulate tissue through the posterior pharynx, which may theoretically increase the risk of neurovascular injury. Additional risks include infection and postoperative airway edema. Typically, a tonsillectomy is performed with the intraoral approach increasing the risk of bleeding associated with the additional procedure, however, tonsil-sparing techniques are also used.2,8
Transoral robotic surgery (TORS) is a relatively new surgical technique that is increasing in popularity for a variety of head and neck surgeries since its Food and Drug Administration (FDA) approval in 2009. 9 TORS has been established as a proven technique for early-stage oropharyngeal cancer, and its safety for other head and neck indications is also being established.10-12 The benefits and drawbacks of TORS is an ongoing discussion. Generally, the benefits are a minimally invasive approach with smaller incisions, decreased blood loss, shorter hospital stay and recovery, better functional outcomes, and lower morbidity and complications. 13 Depending on the case, TORS may also provide better visualization and access to structures (Figure 1).9,13 The main drawback is cost and accessibility to the robotic system and instruments. Utilization also warrants specific training, leading to a learning curve for surgeons. Depending on the experience level, operative times may be longer or shorter than traditional approaches.9,13

Transoral robotic surgery for Eagle syndrome. (A) Exposure of styloid process. (B) Transection of styloid process. (C) Removal of styloid process.
When considering the benefits and drawbacks of using TORS versus another approach, it is important to take the unique surgery or case into account. TORS has begun to be introduced for the treatment of Eagle syndrome. This may allow for similar benefits of an intraoral approach, but with better visualization, thus decreasing risk of damage to neurovascular structures and other complications.14,15 The overall objective of the study was to see if TORS is safe and effective in the treatment of Eagle syndrome.
Patients and Methods
We used the guidelines set forth in the Preferred Reporting Items for Systematic Review and Meta-Analyses 2020 (PRISMA) to report our findings. 16 A comprehensive search (Sup) strategy was written for each database (EW), and then PubMed (National Institutes of Health, National Library of Medicine), Embase.com (Elsevier), Web of Science Core Collection (Clarivate), CINAHL Plus (EBSCO), and Science Direct (Elsevier) were searched. The initial searches were completed in August 2021. A total of 1168 citations were located from all databases. Systematic Review Accelerator’s (https://sr-accelerator.com) Deduplicator was used to identify duplicate citations. After duplicates were removed, there were 754 unique citations, which were uploaded to Rayyan (https://www.rayyan.ai/) for screening. An update was performed in February 2024. All databases were first searched again using the original search strategies, and then an additional search string was added to isolate anything published in 2021, 2022, 2023, and 2024. This yielded 327 new citations. After removing duplicates, 166 remained. These citations were compared to the original ones, which resulted in an additional 20 being removed, leaving 146 unique citations to be uploaded into Rayyan. This addition brought the total number of articles to be screened to 900. An initial screening was done by 2 independent reviewers (DK and AA) based on abstracts. Inclusion criteria included articles describing TORS for Eagle syndrome, had 3 or more patients, and presented original data or patient cases. Exclusion criteria included unrelated articles, wrong surgical technique, abstracts, reviews, foreign language only, fewer than 3 patients, and cadaver studies. Disagreements were resolved with discussion, with a third reviewer (BAC) available for arbitration. Primary outcomes that were evaluated included surgical success rate, estimated blood loss (EBL; mL), postoperative bleeding, other surgical complications, and symptom improvement (complete, partial, none). Secondary outcomes included average operative time (minutes), average length of stay (LOS; days), and time to resuming a regular diet. Data were manually extracted and recorded in a spreadsheet for the final studies. Analyses including calculating percentages, mean, and standard deviation were performed when applicable and other data were reported directly from the studies. No protocol amendments were made over the study.
All studies included in the review were nonrandomized, and therefore the Methodological Index for Non-Randomized Studies (MINORS) tool was used. MINORS is a validated tool to assess nonrandomized surgical studies as described by Slim et al. 17 This tool assessed nonrandomized studies on the following criteria: clearly stated aims, inclusion of consecutive patients, prospective data collection, appropriate endpoints, unbiased evaluation of endpoints, appropriate duration of follow-up, and loss to follow-up no more than 5%. Each noncomparative study was scored from a scale of 0 to 16, with the comparative study scored with a maximum score of 24. A higher score indicates a higher risk of bias.
Results
The results of the literature search are presented in the PRISMA Flow Diagram (Figure 2). A total of 1168 citations were initially identified through the searches, with 327 additional citations during the updated search. After duplicates were removed, abstracts were screened. Twenty studies were included for a full-text review. Further exclusions were made on the same criteria. Ultimately, 4 articles were included for full analysis (Table 1). These included 3 case series and 1 comparative retrospective cohort study. The total sample size of patients who underwent TORS was 19 patients. The mean age of all patients was 54.1 with a range between 37 and 78 for all studies that recorded age. In total, there were 7 males and 12 females included. Across all studies, the patients were mostly female (63% vs 37%). There was a variety of presenting symptoms, the most common of which were neck pain, throat pain, globus sensation, odynophagia, and otalgia.
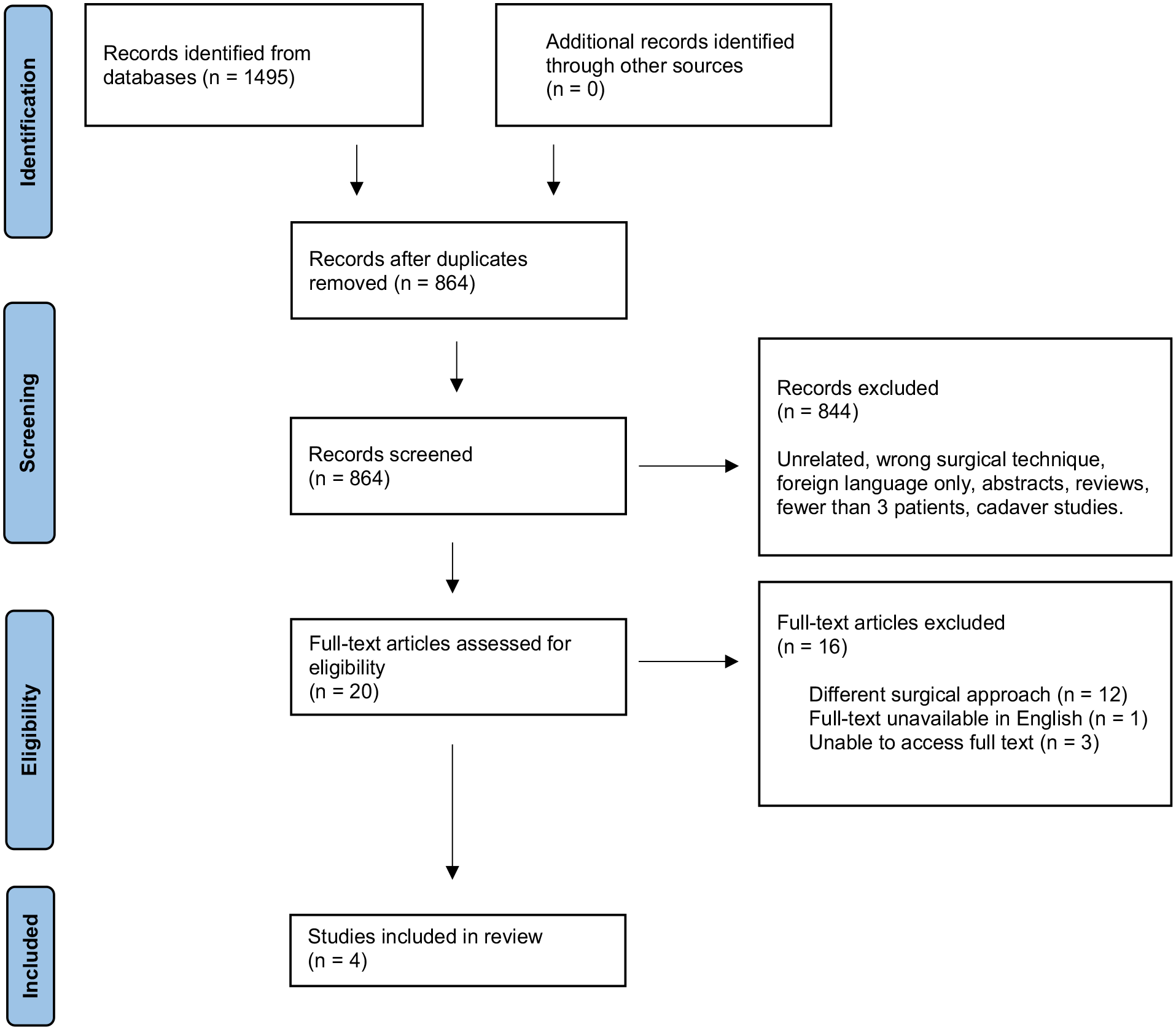
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analyses.
Study Details and Demographics.
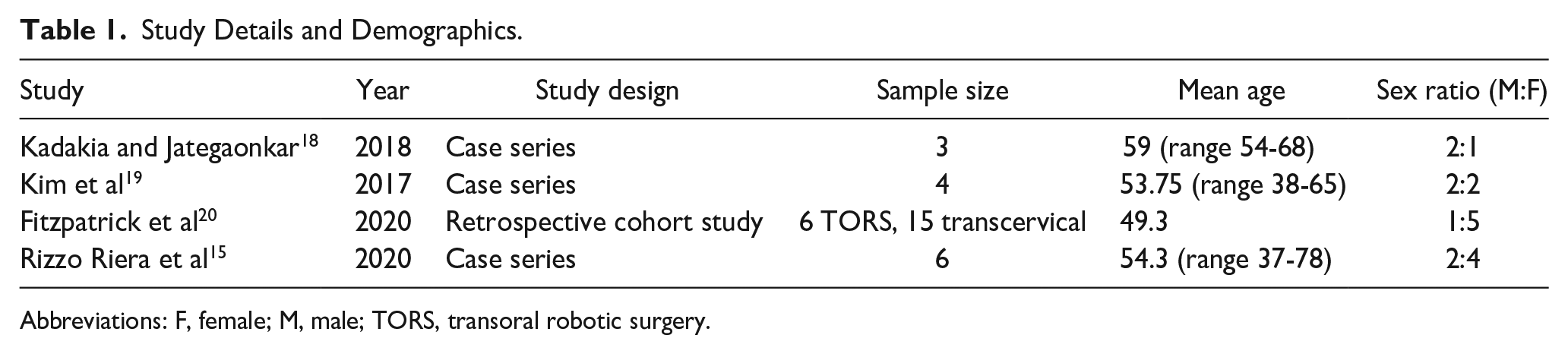
Abbreviations: F, female; M, male; TORS, transoral robotic surgery.
The study by Kadakia and Jategaonkar was a case series of 3 patients who underwent TORS for Eagle syndrome. They had no complications and overall favorable outcomes, with a 100% surgical success rate. The study by Kim et al was a similar case series of 4 patients, all with no complications, overall favorable outcomes, and a 100% surgical success rate. Fitzpatrick et al performed a retrospective cohort study analyzing 6 patients undergoing TORS for Eagle syndrome and 15 treated with a transcervical approach. Of the TORS patients, all 6 had no complications, overall favorable outcomes, and a 100% surgical success rate. The study by Rizzo-Riera et al was a case series of 6 patients, all of whom underwent TORS for Eagle syndrome. They had overall favorable outcomes and a 100% surgical success rate, although there was one reported complication of suture dehiscence.
The TORS technique described in the studies began with robotic arms angled around 30° into the oral cavity. An initial incision was made through the retromolar trigone and pterygomandibular raphe. Blunt dissection was used to open a space between the buccopharyngeal fascia and parapharyngeal space. Styloglossus was then identified inferiorly, and the superior constrictor was elevated. After division of the stylohyoid ligament, the styloid process could be exposed, skeletonized, and excised. The procedure ended with pharyngoplasty by reapproximating mucosal flaps.15,18,19 Fitzpatrick et al did not describe the technique used in their study. 20
Primary Aim Results
The outcomes of each study are reported in Table 2. Across all studies, there was a 100% surgical success rate. Reported EBL averaged 12.5 mL. Of note, Kim et al reported an average of 20 mL which included individual measurements of 5, 5, <10, and 60 mL. The 60 mL value was attributed to a patient with increased mucosal bleeding tendency due to underlying disease. Rizzo-Riera et al did not report specific values but said EBL was minimal in all patients. Postoperative bleeding was not mentioned in 3 studies and no cases of postoperative bleeding were reported in the other. Out of the 19 patients included in the analysis, 18 had no surgical complications (94.5%). One patient had suture dehiscence on postoperative day (POD) 4, which was managed conservatively and healed by secondary intention without further sequela. 15 In total, every patient reported some level of symptom improvement. A total of 84% (n = 16) of patients had complete symptom improvement and 16% (n = 3) had partial improvement. There was a large variety of recorded symptoms at presentation including neck pain (n = 8), throat pain (n = 7), globus sensation (n = 4), odynophagia (n = 4), otalgia (n = 3), syncope (n = 2), pain with mastication (n = 1), right eye pressure (n = 1), hemifacial pain (n = 1), and craniofacial pain (n = 1).
Surgical Outcomes.
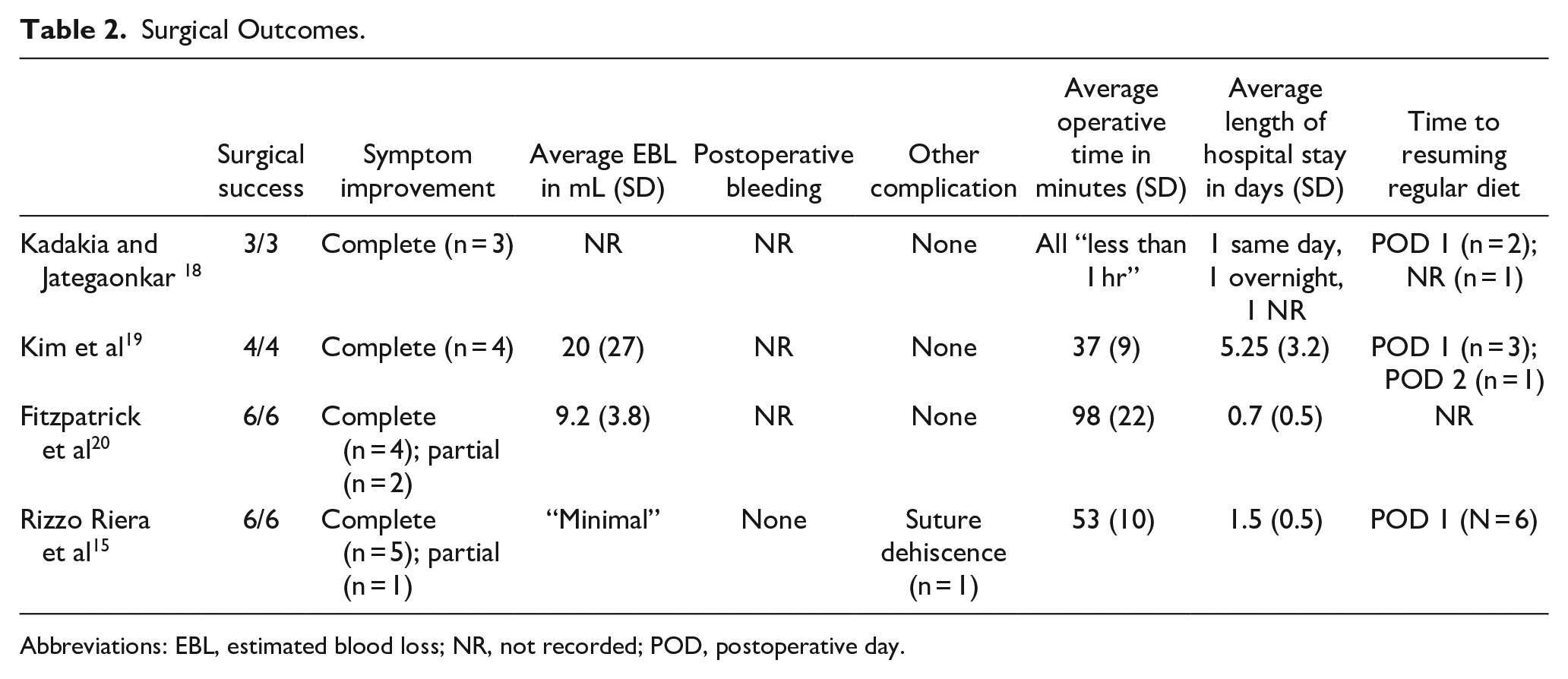
Abbreviations: EBL, estimated blood loss; NR, not recorded; POD, postoperative day.
Secondary Aim Results
Operative time across all studies averaged around 65 minutes. The average LOS of 3 of the studies was 2.1 days, with the study by Kadakia and Jategaonkar not included as discharge was reported as same day (n = 1), overnight (n = 1), or not recorded (n = 1). Notably, the study by Kim et al had a longer average LOS of 5.25 days compared with the other studies which never exceeded 2 days. Time to resuming a regular diet was recorded in select patients, with 92% (n = 11) resuming their diet on POD 1 with 8% (n = 1) resuming on POD 2.
When assessing the quality of these nonrandomized surgical studies, the average MINORS score was 7 (out of 16) for the noncomparative studies and 16 (out of 24) for the comparative study. These scores indicate a risk of moderate bias.
Discussion
Eagle syndrome is an elongation of the styloid process that sometimes requires surgical intervention, previously with cervical and intraoral approaches. With the increasing utilization of robotic surgery, TORS for the treatment of Eagle syndrome has been introduced and described in the literature. This systematic review includes 4 studies with 19 patients who underwent TORS for Eagle syndrome. Based on the review, TORS may be an effective surgical approach to manage Eagle syndrome. A total of 100% of patients had a successful surgery with 84% having complete symptom resolution and 16% with partial symptom resolution. Comparatively, prior systematic review of non-TORS approaches found a surgical success rate of 95.8% with a cervical approach and 89.1% with an intraoral approach. 21 Fitzpatrick et al even found a slight trend toward more meaningful improvement with TORS compared to a cervical approach. 20
Ensuring patient safety is vital when evaluating a surgical technique. TORS as a general technique is often associated with lower complication rates.9,12 This review supports a low complication rate, with only 1 out of the 19 cases having had a postoperative complication (5.3%). The complication profile of surgically treated Eagle syndrome is different depending on the approach. Prior studies have shown minimal risk of complications with a transoral approach. 21 However, the risk of facial nerve injury may be more prominent with a cervical approach, which has been reported to be around 1.2%.2,8,21 The risk of other neurovascular injury, while extremely rare, might be reduced with a TORS approach due to improved visualization and precision.2,8,15,18,19 There were no reports of damage to neurovascular structures in the review. General risks of bleeding and infection are possible with all approaches.2,8 EBL is generally reported to be lower with the use of TORS. 13 In this review, EBL averaged around 12.5 mL with no significant postoperative bleeding mentioned in any study. Fitzpatrick et al also described a trend toward lower blood loss and fewer complications in TORS patients as compared to a cervical approach. 20
Besides patient safety, TORS may also provide additional benefits. Compared to a cervical approach, TORS offers a scarless option which may be a significant concern for patients.2,8 In an intraoral approach, patients often require a tonsillectomy for visualization.2,8 The need for this may be reduced with the use of TORS.18,19 This saves additional operative time and morbidity that comes along with the addition of a tonsillectomy. TORS is also generally associated with shorter length of hospital stays and quicker recoveries, as compared to open techniques. 13 In the treatment of Eagle syndrome, TORS may minimize the physical defect of the tonsillar fossa and parapharyngeal space which could decrease the amount of secondary healing necessary and thus reduce recovery time. 18 The average LOS seen in this review was 2.1 days. Fitzpatrick et al also described a trend toward a shorter LOS in TORS patients as compared to a cervical approach. 20 Aside from LOS, patients may also have decreased pain and quicker resolution of symptoms. 18 A total of 92% of patients in this review were able to resume their regular diet by POD 1.
There are clear benefits of TORS, but the potential drawbacks must also be discussed. Given the need for a robotic surgery system, there is a clear financial and access barrier. However, cost may be offset but decreased length of hospital stays and a large initial cost can be better distributed with increasing caseloads. 13 Further cost-benefit analysis is warranted to better elucidate. TORS also requires additional training and may create a learning curve for surgeons, which must be considered. 9 Operative time may vary depending on the experience level, so TORS may be associated with increased or decreased operative times. 13 This review found operative time to vary substantially between studies, ranging from an average 37 minutes to 98 minutes.
Understanding the general benefits and drawbacks of TORS, it is also important to recognize that the decision of surgical technique should be tailored to the individual patient. Reviewing imaging and the size and angulation of the styloid process is an important consideration when determining the feasibility of TORS. A more medially deflected styloid is likely better suited for TORS. 20 In addition, patient presentation, risk factors, previous tonsillectomy, and patient preferences all should be considered when deciding on an approach.
Limitations of this systematic review should be considered. Given the limited literature and studies that met inclusion criteria, a small sample size of 4 studies with 19 patients were reviewed. The studies are limited to case series and a retrospective cohort study, inherently limiting the quality of evidence. All studies demonstrated a moderate risk of bias based on MINORS criteria. The common reasons included lack of randomization and blinding, risk of selection bias, and the retrospective nature of the studies. The studies by Kadakia and Jategaonkar and Rizzo-Riera et al additionally had an insufficient follow-up period. Also all case series articles do not describe inclusion criteria. Furthermore, each study reported different outcomes, so the data were not all standardized and some outcomes analyzed were not recorded in all studies. Though this review results suggest TORS may be a safe and effective technique with promising advantages, the existing data are not sufficient to make strong conclusions. Surgeons interested in using TORS for Eagle syndrome may use these reports to recognize this approach as a potential option for treatment, although the decision to use TORS should be an individualized decision on part of the patient and surgeon, as well as available resources. There is a need for larger prospective studies, including randomized controlled trials. Studies should directly compare TORS to the standard approaches and collect consistent data regarding symptom reduction, surgical bleeding and complications, operative time, and postoperative outcomes including LOS and time to regular diet. It may be of interest to do further analyses to determine if TORS is of unique benefit with different lengths or angulations of the styloid process.
Conclusion
This systematic review suggests that TORS may be a safe and effective surgical approach in the treatment of Eagle syndrome based on limited quality evidence. This review demonstrated frequent surgical success, low complication rates, and appropriate postoperative recovery with TORS. Transoral approach offers patients the option of a “scarless” procedure; however, it remains a recent development that needs to be approached carefully. Due to the low quality of evidence and small sample sizes, future large, prospective multicenter studies including RCTs are warranted and could offer clinical guidance on if and when TORS should be used over traditional approaches in the treatment of Eagle syndrome.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241246587 – Supplemental material for Transoral Robotic Surgery for Eagle Syndrome: A Systematic Review
Supplemental material, sj-docx-1-ear-10.1177_01455613241246587 for Transoral Robotic Surgery for Eagle Syndrome: A Systematic Review by Darby Keirns, Ameya Asarkar, Payam Entezami, Erin Ware, Thomas H. Nagel and Brent A. Chang in Ear, Nose & Throat Journal
Footnotes
Author Contributions
Darby Keirns is credited with design, analysis and interpretation of the data, drafting of the manuscript. Ameya Asarkar is credited with the analysis and interpretation of the data, drafting of the manuscript. Payam Entezami is credited with drafting of the manuscript. Erin Ware is credited with the literature search and drafting of the manuscript. Thomas H. Nagel is credited with drafting of the manuscript. Brent A. Chang is credited with conception, drafting, and final approval of the manuscript. No other acknowledgments.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because all data used were public, published data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.