
Abstract
Significance Statement
Ulcerative vocal fold lesions occupy the vibratory margins of the musculomembranous portion of the vocal folds and cause dysphonia. Symptoms may exist for several weeks to months before improvement occurs. Lesions observed on strobovideolaryngoscopy may resemble malignant leukoplakia and tempt physicians to obtain biopsy. Biopsy can cause permanent dysphonia and should be performed only when necessary. Therefore, it is important to identify prolonged ulcerative laryngitis and provide appropriate management.
A 73-year-old female presented to our office with dysphonia that had progressed to aphonia. The patient reported having had flu 2 weeks prior to her visit with loss of voice approximately 1 week into the illness. She had fever, dry cough with occasional white mucus, postnasal drip nightly, odynophagia, and muscle aches which had been treated with Mucinex and Tylenol. Covid testing had been negative twice. Her dysphonia developed gradually over a few days during the illness. Pantoprazole 80 mg in the morning and famotidine 40 mg at bedtime had been prescribed, but had been taking only 40 mg of pantoprazole in the morning. She was following a low-acid diet, although she was not completely adherent.
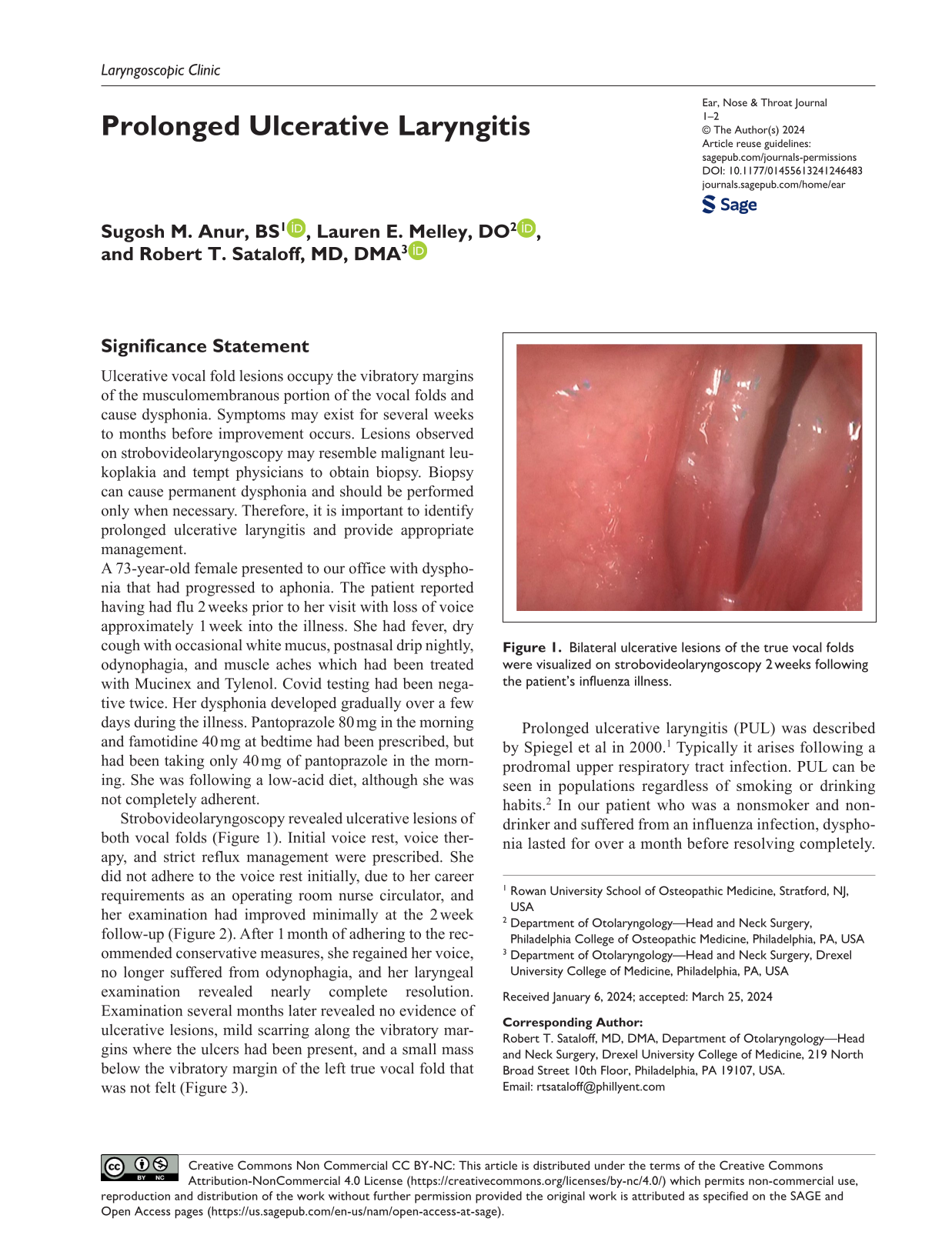
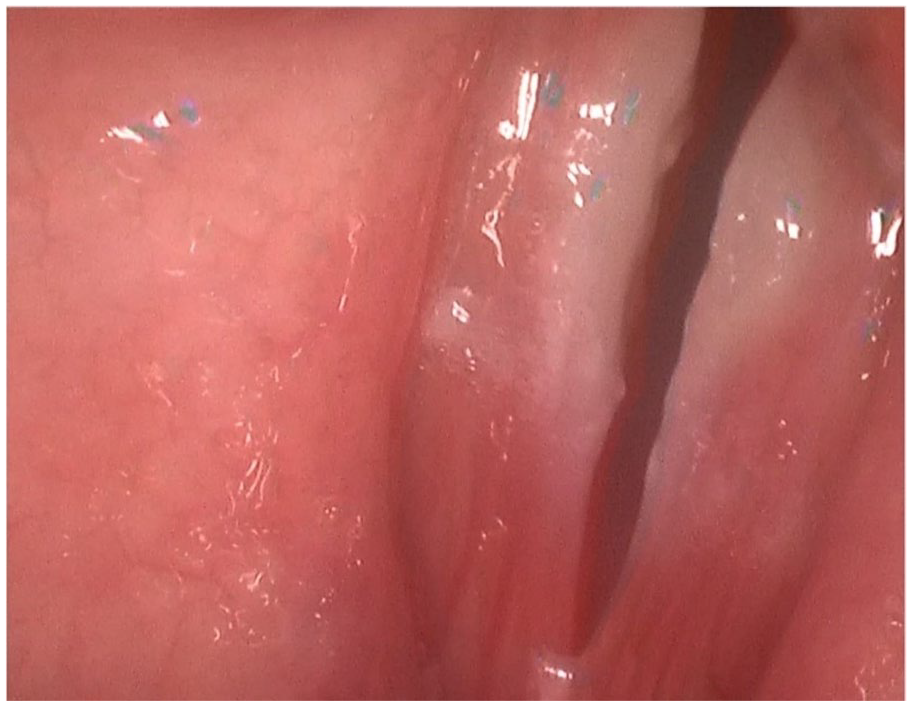
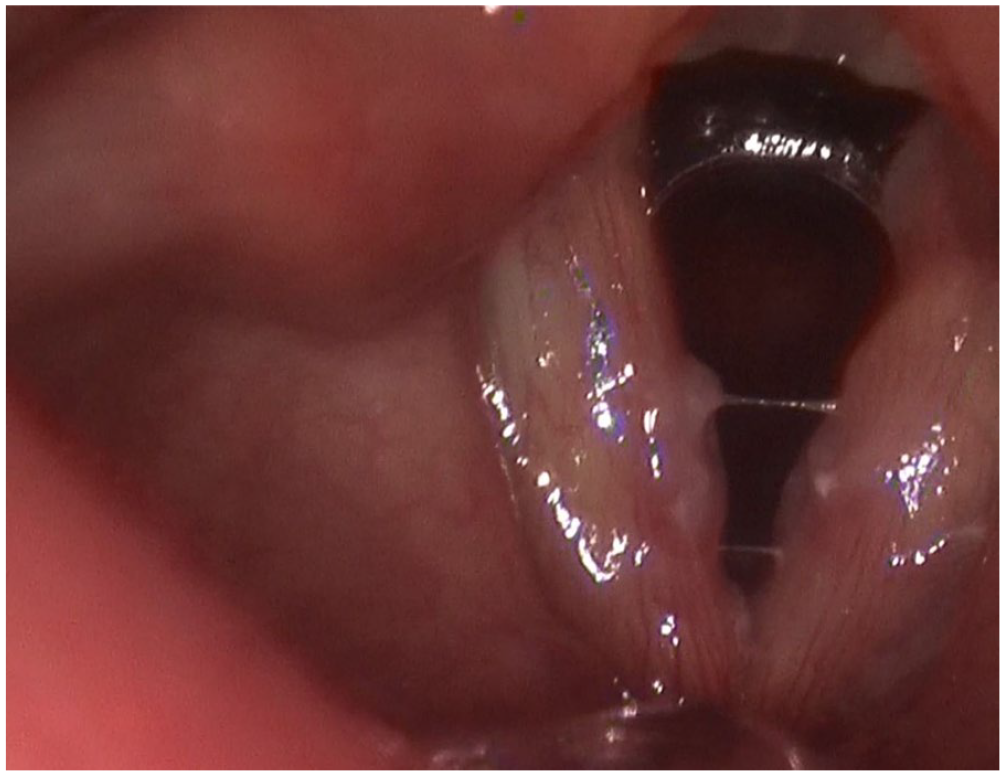
Strobovideolaryngoscopy revealed ulcerative lesions of both vocal folds (Figure 1). Initial voice rest, voice therapy, and strict reflux management were prescribed. She did not adhere to the voice rest initially, due to her career requirements as an operating room nurse circulator, and her examination had improved minimally at the 2 week follow-up (Figure 2). After 1 month of adhering to the recommended conservative measures, she regained her voice, no longer suffered from odynophagia, and her laryngeal examination revealed nearly complete resolution. Examination several months later revealed no evidence of ulcerative lesions, mild scarring along the vibratory margins where the ulcers had been present, and a small mass below the vibratory margin of the left true vocal fold that was not felt (Figure 3).
Bilateral ulcerative lesions of the true vocal folds were visualized on strobovideolaryngoscopy 2 weeks following the patient’s influenza illness.
Bilateral ulcerative lesions of the true vocal folds were mildly decreased in size after 2 weeks of incomplete adherence to voice rest and reflux therapy.
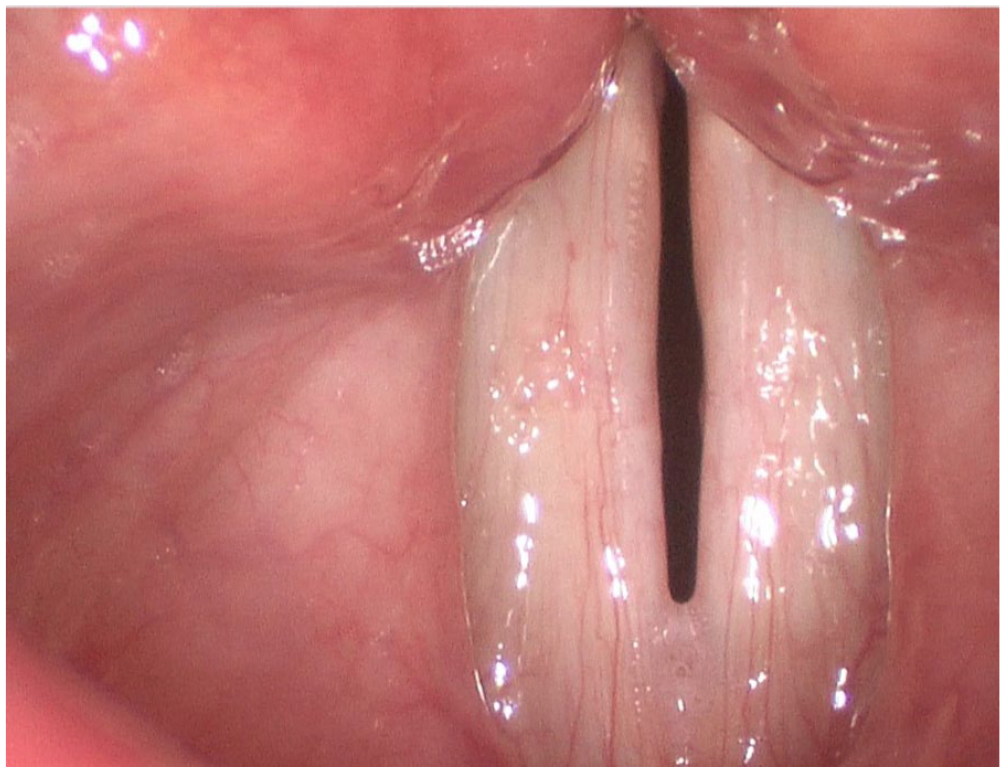
Strobovideolaryngoscopy 10 months following the patient’s initial illness revealed resolution of the ulcerative lesions with evidence of mild scarring along the vibratory margins of the true vocal folds and a small fibrotic mass below the vibratory margin of the left true vocal fold.
Prolonged ulcerative laryngitis (PUL) was described by Spiegel et al in 2000. 1 Typically it arises following a prodromal upper respiratory tract infection. PUL can be seen in populations regardless of smoking or drinking habits. 2 In our patient who was a nonsmoker and nondrinker and suffered from an influenza infection, dysphonia lasted for over a month before resolving completely. A multimodal noninvasive treatment approach proved adequate for resolution and symptom improvement. A combination of voice rest, voice therapy, anti-reflux medication, and symptom monitoring often is adequate to treat PUL.
Complete voice rest was prescribed initially for almost 1 week. Our findings are analogous to other studies showing complete voice rest promoting healing of ulcerative laryngitis.3,4 This is most likely due to promotion of wound healing by decreasing vibratory trauma of vocal fold margins. In addition, adhering to an anti-reflux regimen appears to aid recovery from PUL in patients who have laryngopharyngeal reflux (LPR). Our patient’s adherence to a proton pump inhibitor and a H2 blocker helped decrease inflammation from LPR and thus may have helped healing of the PUL.4,5 This patient has a scar that was present 10 months after presentation. PUL ordinarily resolves without scar; and the scar in our patient might have been unrelated to her PUL.
Diligent surveillance and repeated strobovideolaryngoscopy examinations helped guide management without unnecessary escalation to biopsy. Exacerbation of ulceration, history of smoking, or nonadherence to follow-up appointments would be reasons to consider biopsy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.