
Abstract
Significant Statement
This case study presents a rare instance of Gradenigo syndrome caused by Mycobacterium abscessus, traditionally managed with surgery, being successfully treated with antibiotics alone, challenging conventional treatment paradigms, and highlighting the potential for nonsurgical management in specific cases.
Case Report
In 1907, Dr Gradenigo identified a clinical triad characteristic of a rare complication of otitis media, known as Gradenigo syndrome. This condition, resulting in petrous apicitis and subsequent inflammation of cranial nerves, is typically marked by persistent otorrhea, retro-orbital pain over the trigeminal territory, and diplopia due to abducens palsy. 1 However, the full manifestation of this triad has become infrequent in modern clinical settings due to advancements in antibiotic treatments. 2 Additional symptoms can include other cranial nerve involvements, fever, and otalgia. Common risk factors for the syndrome include a well-pneumatized petrous part of the temporal bone, cholesteatomas, diabetes mellitus, and immunocompromised states. It is generally caused by pyogenic bacteria such as Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas. 3
Given the rarity of Gradenigo syndrome, no standard treatment guidelines exist. The primary approach usually involves surgery, especially when key structures are at risk, necessitating decompression. Surgical procedures like mastoidectomy, petrosectomy, and myringotomy, accompanied by long-term antibiotic use, are often recommended. 4 Timely treatment usually results in the improvement of neurological symptoms.
Nontuberculous mycobacteria (NTM), common environmental bacteria, rarely infect humans. However, the diagnosis rate has increased with the rising prevalence of acquired immunodeficiency syndrome (AIDS) and advancements in culture techniques. NTM infections typically present as lymphadenitis, pneumonia, or soft tissue infections, with otitis media being a rare manifestation. Mycobacterium abscessus, a rapidly growing NTM known for its multidrug resistance, is the most commonly cultured bacterium in NTM otitis media cases. 5 Among the fewer than 100 documented cases of NTM otitis media, 47 have been attributed to M. abscessus, of which 5 have been associated with Gradenigo syndrome. 6
In this case, a 66-year-old male patient with a history of left-sided chronic otitis media and hearing impairment, who also had a smoking habit, presented with persistent otorrhea, retro-orbital pain, double vision, facial palsy, and dysphagia. A physical examination revealed difficulty in left eye abduction, lingual deviation to the left, and left-sided facial palsy. Laboratory findings revealed white blood cell count of 9480 cells/μL, C-reactive protein of 2.34 mg/dL, and an erythrocyte sedimentation rate of 47 mm/hour. Otoscopic examination showed a perforation of the left eardrum with granulation and otorrhea in the external auditory canal (Figure 1).
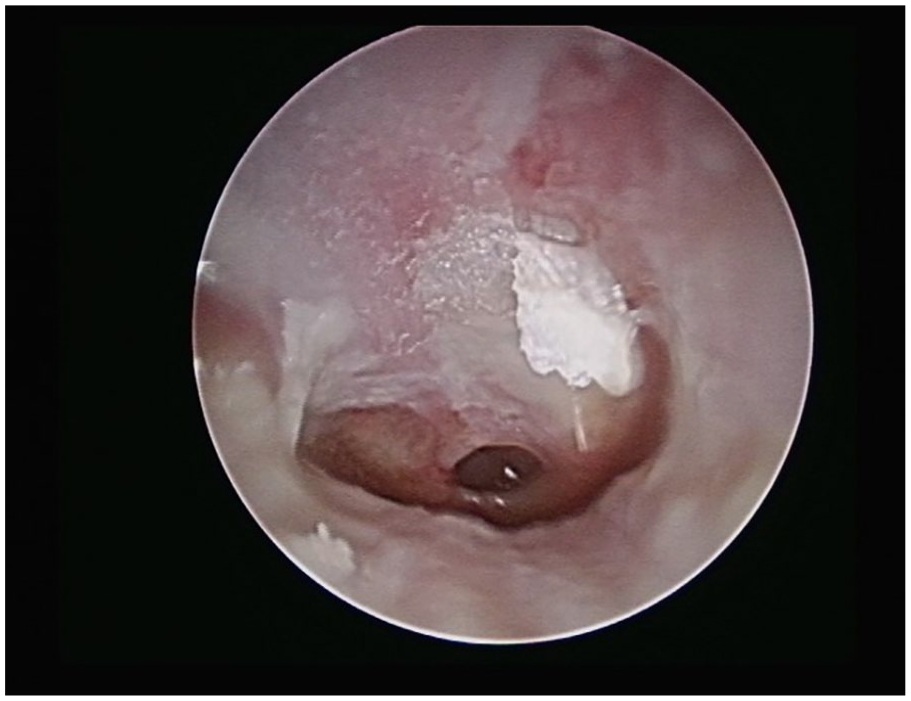
Otoscopic view of the left tympanic membrane exhibiting a 25% perforation and otorrhea, accompanied by granulation tissue.
Imaging studies, including computed tomography scans, showed bony destruction at the petrous apex, mastoid, and inner ear, suggestive of Gradenigo syndrome with involvement of the 5th, 6th, 7th, and 12th cranial nerves. In addition, infection affecting the CP angle and mastoid bone, as well as hypoglossal canal bone destruction affecting tongue movement, were observed (Figure 2). Magnetic resonance imaging (MRI) revealed evidence of petrous apicitis affecting the trigeminal nerve’s Meckel cave and the abducens nerve’s Dorello canal (Figure 3).
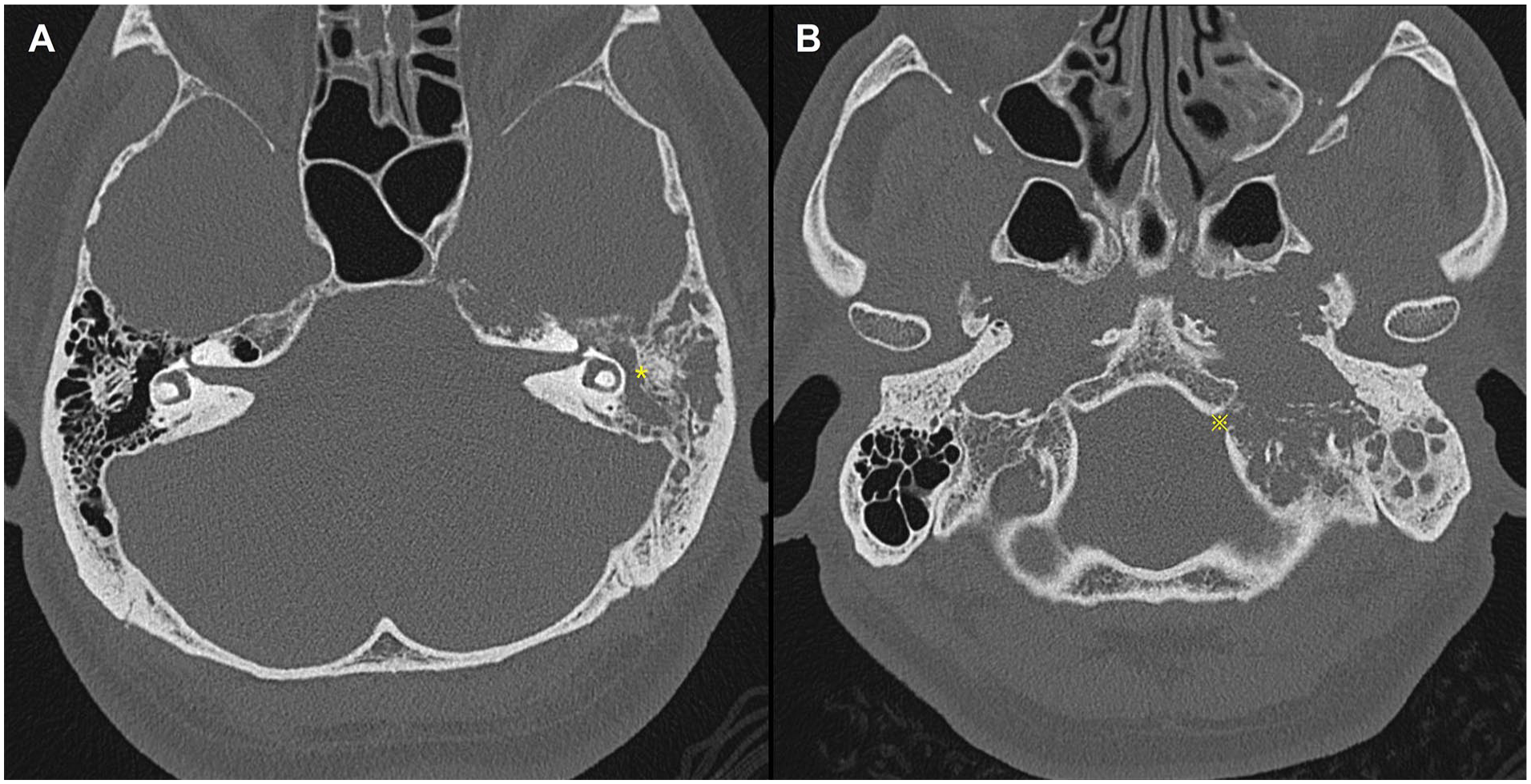
CT scan demonstrating pathological alterations in the left temporal bone. (A) Notable bony erosion within the left inner ear structures, petrous apex, and mastoid area is highlighted by a yellow asterisk (*), denoting the extensive spread of the infection. (B) The hypoglossal canal on the left side shows cortical destruction marked by a yellow cross (※), suggesting involvement in the infectious process. CT, computed tomography.
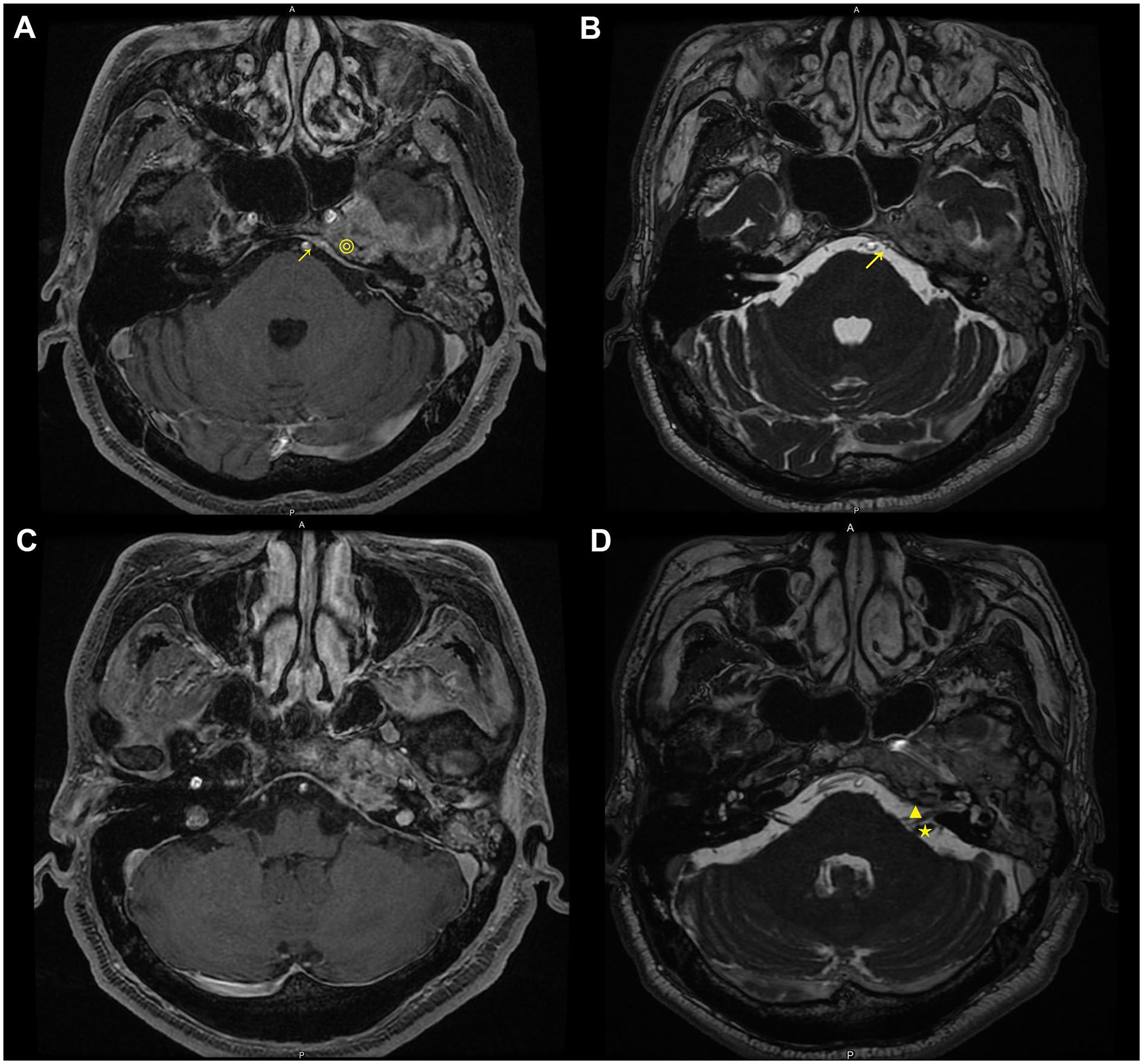
MRI images illustrating findings consistent with Gradenigo’s syndrome. (A, C) T1-weighted MRI images reveal indistinct soft tissue involvement at the left petrous apex and Meckel’s cave, marked with a circle (◎). There is notable enhancement of the surrounding meninges. In addition, encasement of the abducens nerve is observed in the left Dorello’s canal, marked with an arrow (↗). (B, D) T2-weighted FIESTA sequence MRI images highlight cranial nerve involvement. Image (B), (D) shows the area of the abducens nerve in Dorello’s canal indicated by an arrow (↗), and the encasement of the facial (CN VII, triangle ▲) and vestibulocochlear (CN VIII, star ★) nerves, with a focus on the region surrounding the left petrous apex. FIESTA, fast imaging employing steady-state acquisition; MRI, magnetic resonance imaging.
Despite the recommendation for surgical intervention, the patient declined surgery and opted for a conservative treatment approach. He was treated with ceftriaxone, moxifloxacin, and clarithromycin following the identification of M. abscessus from ear discharge culture. Remarkably, the patient’s symptoms showed significant improvement following the initiation of antibiotic therapy. All neurological symptoms and ear discharge resolved completely within 3 months. The patient continued antibiotic treatment for 18 months and has been followed up for 5 years with stable MRI images and no recurrence of symptoms.
This case of Gradenigo syndrome, caused by M. abscessus and complicated by the involvement of multiple cranial nerves, challenges the traditional surgical approach combined with long-term antibiotics. It highlights the potential of medical management in selective cases of this rare condition, demonstrating a successful treatment by antibiotics without surgery.
Footnotes
Authors’ Note
The patient’s identity is not identifiable through the figures and research information; patient consent statement is not added.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital.
Ethical Approval
The Institutional Review Board of Tri-Service General Hospital, National Defense Medical Center, had approved this study (case no. B202215195).