
Abstract
Background
The Perils of Place report by the Grattan Institute identified 18 rural and remote locations in the States of Queensland and Victoria (Australia), as hotspots for ear, nose, and throat (ENT) conditions. In that they have recorded rates of potentially preventable hospitalizations (PPHs) for ENT conditions at least 50% higher than the state average in every year for a decade. 1
In Australia, between 2020 and 2021, ENT diseases accounted for 7% of all emergency department presentations (by principal diagnosis in ICD-10-AM [International Classification of Diseases 10th Revision] codes). 2 There are 5 broad categories for which ENT hospitalizations are considered to be potentially preventable. These are classified as unspecified otitis media, acute pharyngitis, acute tonsillitis, acute upper respiratory tract infections (URTIs) of multiple and unspecified sites, and chronic pharyngitis.1,3-9 These conditions were further categorized into clinically meaningful subgroups as otitis media, URTIs, and acute tonsillitis; being the main ENT conditions of hospitalization in the rural and remote areas of the State of Victoria.10,11
PPHs are conditions for which hospitalization is considered to be avoidable through preventive care which is usually delivered in the primary health care setting.1,12-28 PPHs are an indication of access to and effectiveness of primary health care services and are of interest to health care service providers and public health research, as they characterize the incidence of avoidable morbidity. Furthermore, PPHs provide an evidence-based understanding from which targeted interventions can be developed.1,13-18
Primary health care prevention strategies are typically categorized into 3 levels as primary, secondary, and tertiary prevention. 29 Primary and secondary prevention aim to prevent disease or injury before it occurs through health promotion initiatives and screening for early disease. Tertiary prevention is the treatment once a disease has been identified (including medication prescriptions, disease monitoring, and liaison with other levels of health care), which aligns with the biomedical model of care.29,30 While tertiary prevention plays an integral role within primary health care, the focus of this systematic review is on the primary and secondary prevention initiatives to improve understandings of community-centered and place-based programs.
Early detection and timely management of potentially preventable ENT hospitalizations are fundamental to preventing downstream impacts on health, social, and educational outcomes.31-35 The aim of this systematic review is to (a) identify and synthesize the evidence of primary health care interventions for detection and management of otitis media, URTI, and acute tonsillitis in rural and remote areas, and (b) evaluate the quality of the research and effectiveness of the identified interventions.
Methods
The review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO; https://www.crd.york.ac.uk/prospero/, registration number CRD42022329903). The review is reported according to the PRISMA statement, which includes the eligibility criteria (Figure 1). 36
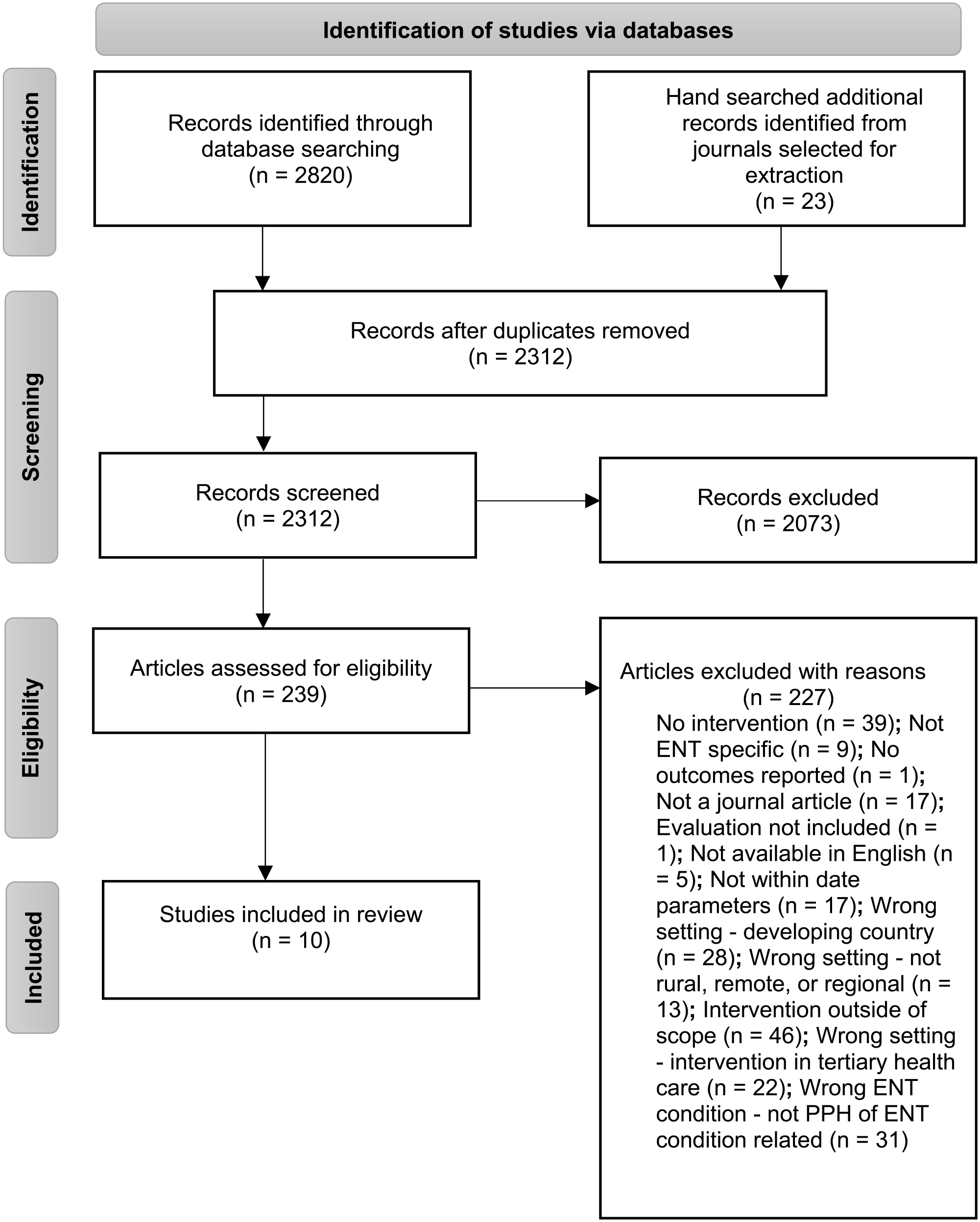
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram.
Search Strategy and Data Extraction
The research team conducted searches of the following electronic bibliographic databases on February 3, 2023: MEDLINE, Embase, CINAHL, Web of Science, PsycINFO, and Cochrane. A preliminary search of MEDLINE was conducted to identify additional keywords, index terms, and subject headings. The search strategy was developed in consultation with a university librarian. An example of the search strategy in MEDLINE is presented in supplementary file 1, using MeSH terms and synonyms. A date filter was applied to ensure the inclusion of up-to-date interventions (2012-2022).
The primary researcher and a second member of the team reviewed the titles and abstracts retrieved from the search strategy. The full texts were retrieved for studies identified as potentially eligible. These were then assessed by 1 team member for eligibility based on the inclusion and exclusion criteria (Table 1). The final screening of texts was reviewed by all team members, with any disagreement resolved by discussion. The reference lists of journals chosen for extraction were hand searched for the inclusion of additional articles, which identified a further 23 studies for screening.
Inclusion Exclusion Criteria.
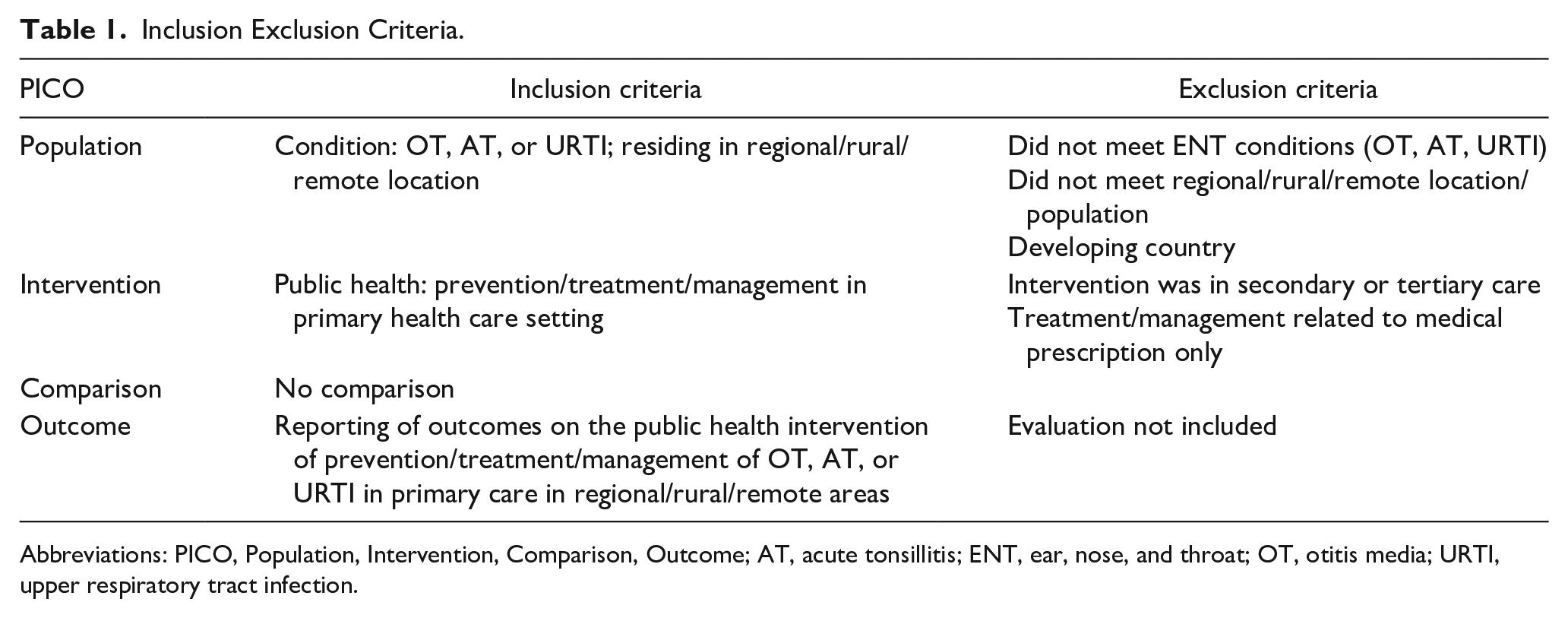
Abbreviations: PICO, Population, Intervention, Comparison, Outcome; AT, acute tonsillitis; ENT, ear, nose, and throat; OT, otitis media; URTI, upper respiratory tract infection.
Inclusion Criteria
Articles were included if they were original research, published in academic peer-reviewed journals. The inclusion and exclusion criteria are outlined in Table 1. Only studies conducted in rural and remote areas were included. The intervention was required to take place in association with a primary health care setting (and excluded tertiary prevention interventions). No comparison was required and all study designs were included. Articles were excluded if they were unavailable in English, due to time and cost limitations. Given the differences in health service delivery and settings between developed and developing countries, this review was limited to developed nations; as defined by the Organisation for Economic Co-operation and Development (OECD) at the time the search was conducted. 37
The terms rural, remote, and regional areas are defined here to encompass all areas outside major urban cities.38-40 In Australia, Canada, and the United States, these areas are geographically classified as inner regional, outer regional, and remote or very remote.38-40
Quality Assessment
The quality appraisal of studies was evaluated using the Mixed Methods Appraisal Tool (MMAT, 2018 Version; Supplemental File 2). 41 The MMAT has been designed for appraising research studies of various designs; it has been pilot tested for efficiency, content validity, and reliability, and has been used in over 100 systematic reviews.42-44 Each criterion is assessed as either met (“Yes”), not met (“No”) or insufficient information for judgment (“Can’t tell”). 41
Data Synthesis
Hsieh and Shannon’s content analysis approach was used for the data synthesis. 45 This inductive approach involved an understanding of the included articles, exploration and description of the emerging themes, and categorization as relevant to the research questions.45,46 Tabulation of the categories identified from the data allowed for exploration of the themes, such as outcomes measured and study population (Supplemental File 3).
Results
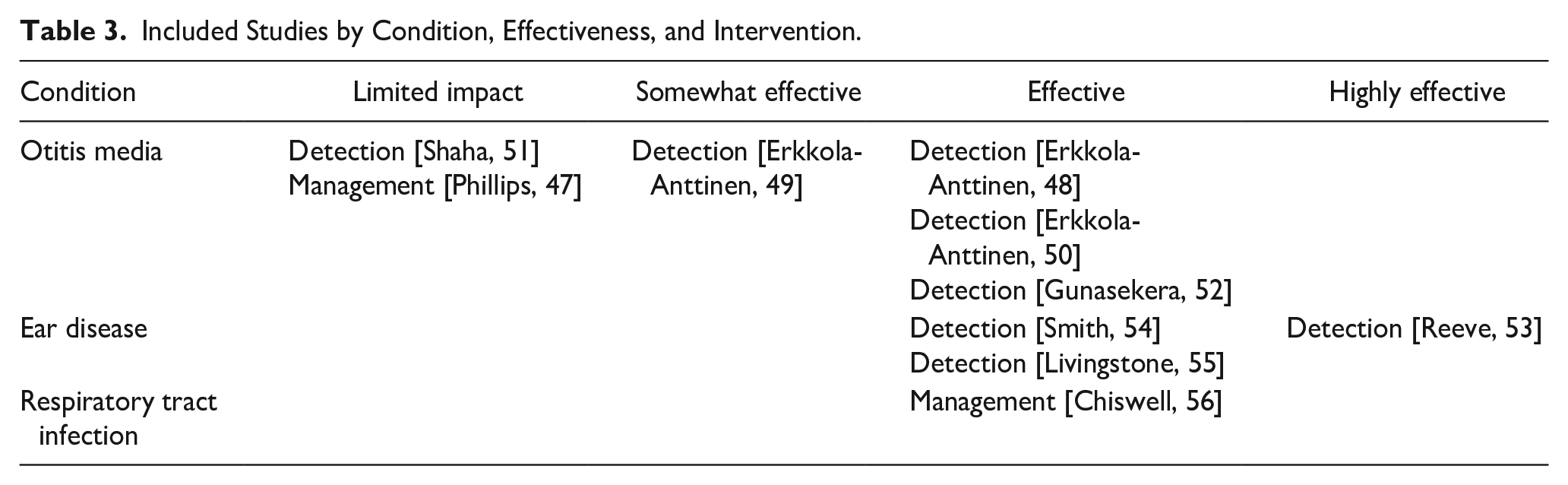
The 10 included articles were randomized and nonrandomized quantitative studies. Four of the studies were conducted in Australia, 3 were in Finland, 2 in the United States, and 1 was in Canada (Table 2). The majority of the interventions addressed otitis media,47-52 3 were more broadly based on ear diseases,53-55 and 1 on respiratory tract infections (RTIs). 56 No included studies were of interventions for acute tonsillitis. The included studies address the detection and management care pathways, effectiveness of interventions and quality of evidence. Here, “detection” refers to interventions that focused on detecting ENT conditions including screening, and “management” refers to how ENT conditions are managed, such as the care provided (Table 3).
Key Study Characteristics.
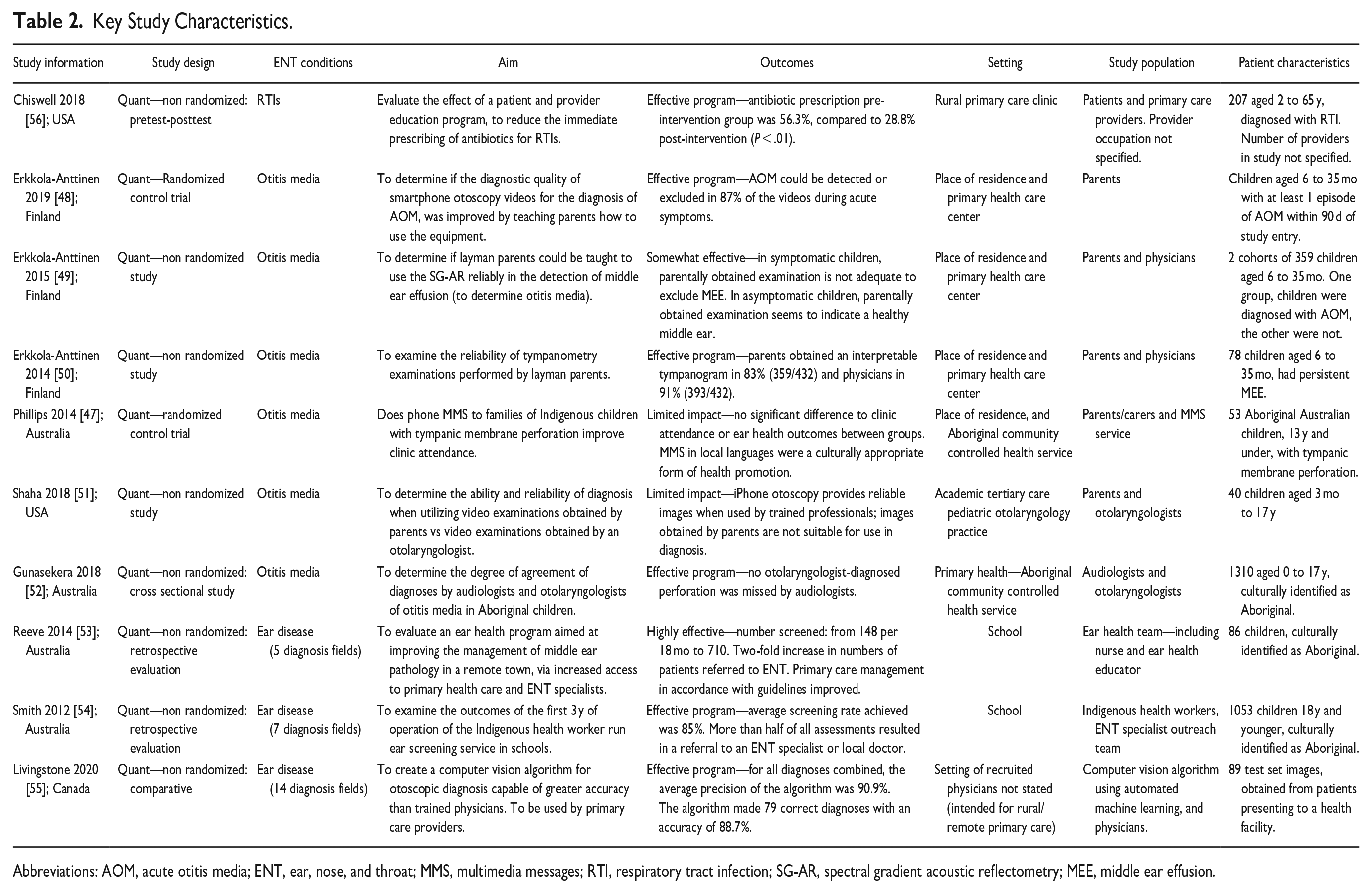
Abbreviations: AOM, acute otitis media; ENT, ear, nose, and throat; MMS, multimedia messages; RTI, respiratory tract infection; SG-AR, spectral gradient acoustic reflectometry; MEE, middle ear effusion.
Included Studies by Condition, Effectiveness, and Intervention.
Primary Health Care Interventions for Detection and Management of Otitis Media, RTIs, and Ear Disease in Rural and Remote Areas
Detection
Interventions for the detection of OM were described in 5 of the 10 articles included in this review. Two used a smartphone and iPhone otoscopy to capture video images,48,51 and 2 used the spectral gradient acoustic reflectometry (SG-AR) 49 and a tympanometry device as alternative methods to review the middle ear. 50 In 3 of the studies, the performance of the handheld devices in the hands of parents was measured against that of a physician or specialist.49-51 In one study, the accuracy of use was compared in 2 groups of parents, one of which was provided with teaching assistance prior to use and one which was not. 48 One intervention measured the performance of audiologists in diagnosing OM with or without perforation against the diagnosis of an otolaryngologist. 52
Interventions for the detection of ear disease were described in 3 of the 10 articles.53-55 Detection of ear disease was measured in one study through a computer vision algorithm, 55 and in the other 2 through community-based programs.53,54 Interventions for the 2 rural and remote community-based programs were delivered by allied health workers (AHWs) and community health care services.53,54 The occupations of this group included nurses and ear health educators, 53 First Nations health care workers, 54 and otolaryngologists and ENT specialists. 54 One study implemented a primary care ear health pathway for Indigenous children, and the other utilized a mobile telemedicine screening service for Indigenous children.53,54
Management
An intervention for the management of RTIs was described in 1 of the 10 included articles in this review. 56 This intervention addressed the management of RTIs through parent and provider education to reduce overprescription of antibiotics. 56 This study aimed to change health beliefs, values, and practices through an educational health promotion resource that aimed to improve health literacy. 56 Of the 6 articles included that addressed OM, 1 intervention aligned with the management of OM in primary health care settings. 47 This intervention utilized multimedia messages (MMS) and text messages to support clinic attendance of Aboriginal and Torres Strait Islander children in a remote setting. 47
Effectiveness of Primary Health Care Interventions for Detection and Management of Otitis Media, RTIs, and Ear Disease According to the MMAT Criterion
Detection
The 5 interventions which focused on the detection of OM found variable impact in the effectiveness of interventions.48-52 Two studies by Erkkola-Anttinen et al were found to be effective.48,50 In one study, the post teaching intervention of parents in the use of a smartphone otoscopy found that acute otitis media could be detected or excluded in 87% of videos, 48 and 83% of parents performed an interpretable tympanogram in the other study. 50 In another study by Erkkola-Anttinen et al, the parentally obtained SG-AR examination was not adequate to exclude middle ear effusion. 49 Based on this outcome, the study was classified as somewhat effective. 50 In the study by Shah et al, which compared the ability to diagnose OM from iPhone otoscopy taken by parents against otolaryngologists, it was determined to have limited impact as the images obtained by parents were not suitable for diagnosis. 51 In the study by Gunasekera et al, 52 which utilized audiologist in remote regions, no otolaryngologist diagnosed perforation was missed by audiologists. This intervention was determined to be effective.
The 3 interventions that related to detection of ear diseases were considered effective and highly effective based on the results reported. In the studies by Reeve et al and Smith et al, screening rates for ear disease in First Nations communities was increased by 2-fold, appropriate ENT specialist referrals increased and the wait time for ENT review by telehealth reduced to less than a month in both interventions.53,54 In Livingstone and Chau’s study, the results of a computer vision algorithm were compared against that of 10 trained physicians. 55 For all diagnoses combined, the average precision (positive predictive value) of the algorithm was 90.9%, and the average recall (sensitivity) was 86.1%. 55 This study was determined to be effective.
Management
The 1 patient and provider education intervention by Chiswell for RTI management was considered to be effective. 56 Medical records of patients (pre- and post-intervention) were analyzed, with antibiotic prescription being statistically significant; preintervention of 56.3% compared to 28.8% postintervention (P < .01). 56 The study by Phillips et al, which utilized health promotion information through MMS to First Nations families whose child had tympanic membrane perforation, was described to have limited impact, as there was no difference to clinic attendance or ear health outcomes between the group that received MMS and the group that did not. 47
Quality of Evidence
The MMAT quality assessment table is shown in Supplemental File 2. Only 2 articles satisfied the first screening questions: “Are there clear research questions?” 42 Both research studies were quantitative randomization controlled trials.47,48 These programs generally demonstrated appropriateness in the performance of randomization, comparable groups at baseline, and participants adherence to the assigned intervention. It is unclear from the information in the articles if the outcome data were complete.
The studies by Chiswell et al, 56 Erkkola-Anttinen et al, 49 Erkkola-Anttinen et al, 50 Shah et al, 51 Gunasekera et al, 52 Reeve et al, 53 Smith et al, 54 and Livingstone an Chau 55 were all quantitative nonrandomized studies, and they did not satisfy the initial screening questions. Where study aims were identified,51,52 research questions were not clearly stated. These studies utilized common designs of a quasi-experimental pretest posttest 56 ; cohort study49,55; nonrandomized controlled trials 50 ; cross-sectional study51,52;and case-control study.53,54 The interventions occurred as intended in all of these studies with the participants being described as representative of the target population, and the measurements were appropriate to the intervention.49-56
Discussion
This systematic review aimed to identify and synthesis the evidence of primary health care interventions for detecting and managing OM, URTI, and acute tonsillitis in rural and remote areas, and to ascertain the effectiveness of interventions and the quality of evidence. The 10 included studies addressed interventions for RTIs, OM, and ear disease; no studies were included for acute tonsillitis. The results are discussed which include effective outcomes from community-based programs, the supporting role of AHWs in ENT detection and management, gaps in the published literature, and recommendations for future research.
Community-Based Programs
The results highlight the importance of community-based programs to deliver culturally appropriate preventative care and early disease management.47,53,54,56 The outcomes of the educational programs provided in studies by Reeve et al, Smith et al, and Chiswell et al53,54,56 were described as effective and highly effective and aligns to international best practice frameworks for primary health care by enabling people to increase control over, and to improve their health through self-determination. 57 In the studies by Phillips et al, Reeve et al, and Smith et al,47,53,54 community-based health screening services provided accessible and timely treatment to priority population groups, building resilience and self-determination through locally trained administrators.47,53-55 First Nations Health Workers supported the acceptance and use of community-based programs, providing a link not just for the target population but also for external health care service providers, for the services to be delivered more culturally appropriate to their setting.31-33,47,53,54,58-74
AHWs and Alternative Health Care Models
In this current review, evidence suggests audiologists are appropriately placed in detecting and managing ear conditions. 52 This is due to their exclusive focus on the ear and accessibility within rural areas, filling a gap in primary health care services. 52 Greater support and coordination between AHWs and primary care services would greatly benefit regions lacking ENT access and care. This is supported in other studies which did not meet our inclusion criteria (excluded for reasons pertaining tertiary clinical programs, setting in a developing country, and study protocols), where AHWs have been afforded expanded scope in practice to assist with ENT care.52,74-77 AHWs have been utilized in ENT outpatient clinics to assist with wait times, and access to treatment. 78 Expanded roles for AHWs have gained popularity over the past decade, with a focus on redesigning service delivery, aiming to provide more flexible and patient-focused services, while increasing access to high-value care, at acceptably low costs. Optimizing and extending AHWs’ scope of practice can provide a responsive workforce while maintaining safe quality health care.52,76-84
Alternative models of health care delivery include the advanced care practitioner role or the rural generalist framework, in which the discipline of the professional providing care is less important than the skill set they afford communities.85,86 As identified from the included studies, the key skills required for delivering ENT primary health care interventions were communication to disseminate ENT health education effectively as applicable to the community; knowledge of common ear diseases and the ability to diagnose with handheld devices; computer literacy to remotely collaborate with other health care professional via telehealth; and an understanding of appropriate referrals to support timely care.47,52-56 This may form the basis for a rural generalist ENT preventable hospitalization program in the context of rural communities.
Gaps in the Research Literature
Only 2 studies were included on ENT management in primary health care settings where the scope of the review was limited to primary and secondary prevention and excluded tertiary prevention. This might suggest an underexplored area for practice for prevention-focused care by a physician and multidisciplinary health care team, which provides care beyond the scope of the biomedical model. The studies which met the search criteria in our analysis were predominantly aimed at otitis media and ear disease.47,48-46 There is a potential gap in the literature for prevention-focused detection and management of acute tonsillitis. Included studies of URTI broadly groups together all conditions affecting the upper respiratory tract region, and will include otitis media, tonsillitis, pharyngitis, and the common cold, which could be relevant.86-88 Journal articles that focused exclusively on tonsillitis were identified in searches, but were excluded because they related to tertiary preventative care, such as the appropriateness of antibiotics in preventing further complications of tonsillitis.88-92
Last, only 10 studies were included overall which could reflect a lack of investment in rural primary health care research. In Australia, authors have argued that the underinvestment in rural health research is contributing to the inequity in health outcomes. There are calls for greater investment in rural health research and research capacity including clinician researchers to address this gap and need.93-95
Study Limitations
This research was focused on interventions in rural and remote primary health care settings in developed countries. The findings should be interpreted with caution as only 10 studies were located and included, with the majority being from Finland and Australia, and only one article from Canada, and 2 from the United States. Rural regions and communities are diverse within and across nations and the lack of research limits the translation of research to practice and policy. This may have been due to the terminology used in the search terms and different terminology used internationally; however, a comprehensive search strategy was applied (Supplemental File 1). The review was also limited to studies published in English language which could have prevented inclusion of additional relevant studies.
Conclusion
The aim of this systematic literature review was to review and synthesize the range and quality of evidence, and to determine the effectiveness of interventions. Of the ENT conditions included in the literature search, none met the criteria for tonsillitis. This requires further exploration in the context of what is considered to be a potentially preventable ENT hospitalization. From this study’s findings, the role of community-based programs and AHWs in the detection and management of ear conditions was found to be effective. These findings may be used to inform future programs developed to address primary health care ENT services in rural and remote regions.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241245198 – Supplemental material for Primary Health Care Interventions for Potentially Preventable Ear, Nose, and Throat Conditions in Rural and Remote Areas: A Systematic Review
Supplemental material, sj-docx-1-ear-10.1177_01455613241245198 for Primary Health Care Interventions for Potentially Preventable Ear, Nose, and Throat Conditions in Rural and Remote Areas: A Systematic Review by Susan O’Neill, Stephen Begg, Nerida Hyett and Evelien Spelten in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-2-ear-10.1177_01455613241245198 – Supplemental material for Primary Health Care Interventions for Potentially Preventable Ear, Nose, and Throat Conditions in Rural and Remote Areas: A Systematic Review
Supplemental material, sj-docx-2-ear-10.1177_01455613241245198 for Primary Health Care Interventions for Potentially Preventable Ear, Nose, and Throat Conditions in Rural and Remote Areas: A Systematic Review by Susan O’Neill, Stephen Begg, Nerida Hyett and Evelien Spelten in Ear, Nose & Throat Journal
Supplemental Material
sj-xlsx-3-ear-10.1177_01455613241245198 – Supplemental material for Primary Health Care Interventions for Potentially Preventable Ear, Nose, and Throat Conditions in Rural and Remote Areas: A Systematic Review
Supplemental material, sj-xlsx-3-ear-10.1177_01455613241245198 for Primary Health Care Interventions for Potentially Preventable Ear, Nose, and Throat Conditions in Rural and Remote Areas: A Systematic Review by Susan O’Neill, Stephen Begg, Nerida Hyett and Evelien Spelten in Ear, Nose & Throat Journal
Footnotes
Data Availability
The authors declare all included articles in this review are publicly available from the listed publication database sites.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors declare ethical approval was not applicable as this research is a review.
Grant Number
The authors declare no grant number was applicable as this research is a review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.