
Abstract

Significant Statement
Laryngeal paragangliomas are space-occupying lesions usually presenting as submucosal masses in the supraglottis. The treatment of choice for this condition is surgery. In this article, we present a case of a surgically removed laryngeal paraganglioma, measuring 51 mm × 43 mm × 31 mm. Despite its large size, we have been able to completely remove the tumor, while preserving the laryngeal framework. To our knowledge, this is the largest laryngeal paraganglioma reported in the literature.
Case Presentation
A 76-year-old otherwise healthy female patient presented to our clinic with a 2 year history of gradually progressive solid-food dysphagia and a more recent onset of hoarseness and inspiratory stridor. A flexible laryngoscopy revealed a large submucosal tumor affecting the right hemilarynx, completely immobilizing the right vocal fold and significantly reducing the airway. Tracheotomy was performed immediately after admission and subsequent microlaryngoscopy was consistent with the initial clinical finding. During the biopsy, extensive bleeding occurred, suggesting the vascular nature of the tumor and preventing adequate collection of material for histopathological analysis.
Computed tomography with angiography revealed a highly vascularized tumor, measuring 53 mm × 44 mm × 33 mm. It was predominantly localized in the supraglottic larynx, extending submucosally and obliterating the right pyriform sinus, with arterial supply from the right superior laryngeal artery (Figure 1A). Consequently, supraselective embolization of the right superior laryngeal artery was performed.
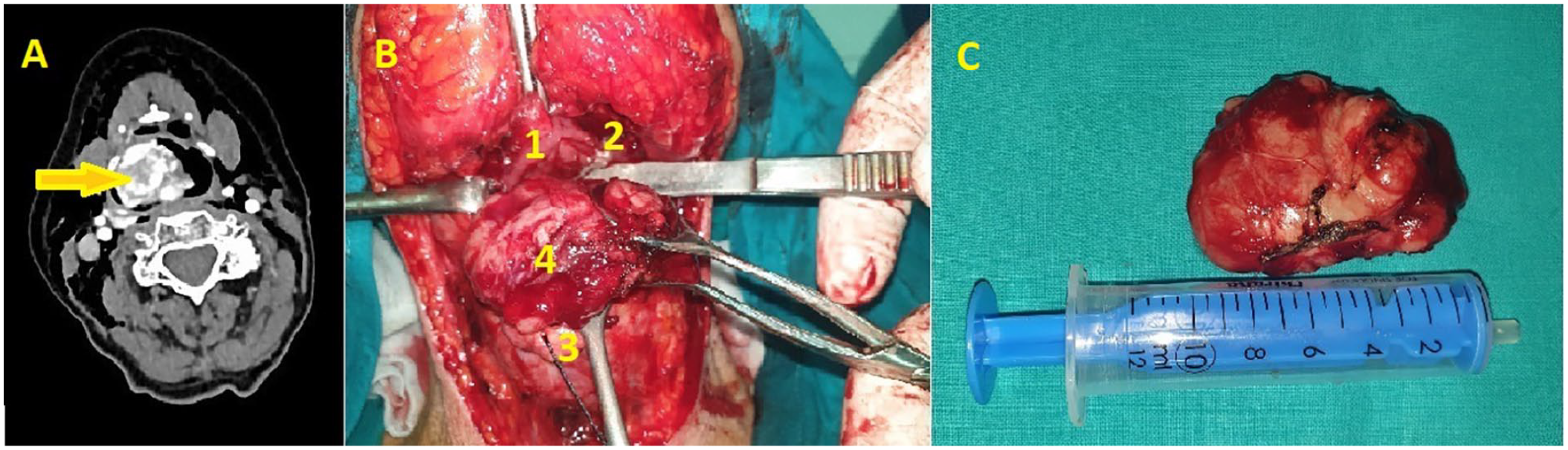
(A) Axial contrast-enhanced neck CT scan. Arrow indicates an expansive lesion of the right hemilarynx with intensive contrast accumulation, measuring 6 cm × 5 cm. (B) Intraoperative view (1—tongue base; 2—hypopharynx; 3—epiglottis; 4—tumor). (C) Macroscopic appearance of the excised tumor. CT, computed tomography.
After infrahyoid pharyngotomy and incision of the mucosa of the left aryepiglottic fold, the smooth and reddish surface of the tumor was identified (Figure 1B). The tumor was well-demarcated and firm, which allowed for blunt dissection of the surrounding tissues with minimal bleeding and adequate reconstruction of the laryngeal mucosa. The patient underwent a nasogastric feeding tube and tracheotomy for 7 days postoperatively and was discharged from the hospital with no breathing difficulties, mild dysphonia, and occasional swallowing difficulties with liquids without aspiration.
In its gross appearance, the tumor was nodular and surrounded by a thin pseudocapsule, measuring 51 mm × 43 mm × 31 mm (Figure 1C). Microscopically, the tumor consisted of trabeculae and nests of epithelioid cells. The cells were uniform in appearance, with an eosinophilic cytoplasm and small nuclei, without signs of atypia or pathological mitoses. The vascular network within the tumor was pronounced and located between the cell groups (Figure 2A). Immunohistochemically, the tumor was positive for synaptophysin, chromogranin, neuron-specific enolase, and S-100 on the periphery of cell groups, CD34 in blood vessels, and Ki-67 in less than 20% of cells (Figure 2B–D). Tumor tissue was immunohistochemically negative for PanCK, CK 5/6, CK7, CK20, p63, TTF1, and melan A. The final histopathological report confirmed the diagnosis of paraganglioma.
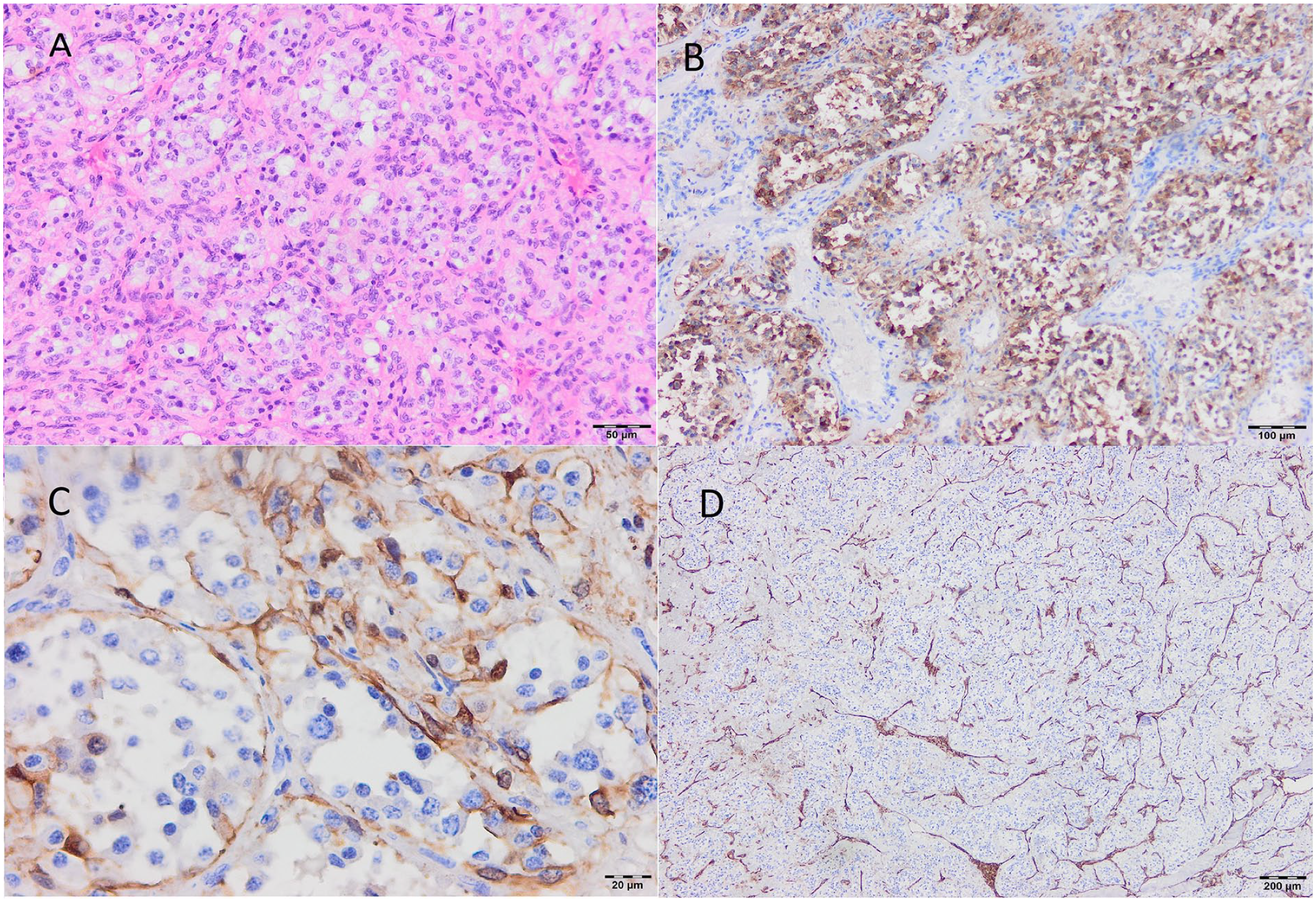
Histopathology of the excised paraganglioma. (A) Hematoxylin & eosin, ×20. (B) Positive immunohistochemical staining for chromogranin, ×10. (C) Positive immunohistochemical staining for S-100, ×20. (D) Positive immunohistochemical staining for CD-34, ×10.
No recurrence, respiratory, or swallowing problems were observed during the 2 year follow-up.
Discussion
Paragangliomas of the head and neck arise from chromaffin tissue distributed along vascular and nerve structures from the level of the skull base to the upper mediastinum. 1 Head and neck paraganglioma usually has a benign clinical course, although malignant paraganglioma can occur. 2
Laryngeal paragangliomas are extremely rare and arise from neuroendocrine cells of the parasympathetic branches of the vagus nerve, most frequently from the paraganglia of the superior laryngeal nerve (90%). 3 Although about 3% of head and neck paragangliomas have secretory activity and may present with symptoms related to elevated catecholamine production, no laryngeal paragangliomas with secretory activity have yet been confirmed.1,4,5
Biopsy during initial microlaryngoscopy may result in significant bleeding that would be difficult to control endoscopically. 6 Imaging studies reveal the vascular nature of the well-defined lesion. Angiography is recommended for vascular mapping, with embolization of the feeding vessels to minimize bleeding during surgery. 7
Differential diagnoses of laryngeal paraganglioma should include submucosal laryngeal lesions, such as other neuroendocrine tumors, lipomas, cysts, laryngoceles, and Teflon granulomas. 6 Immunohistochemical staining will differentiate paragangliomas from other neuroendocrine tumors such as carcinoid, atypical carcinoid, and medullary thyroid carcinoma, which differ significantly in clinical behavior, treatment, and prognosis. 8
The treatment of choice is surgery. Even in small tumors, preoperative embolization seems prudent, especially if an endoscopic approach is planned. 9 Recurrences after complete tumor removal are rare. The endoscopic approach should be reserved for small lesions with good visualization. However, bleeding may occur. CO2 laser-assisted endoscopic removal of laryngeal paragangliomas has been recommended in conjunction with epiglottectomy for better exposure, as well as the use of titanium clips for hemostasis. 10 Incomplete endoscopic excision will ultimately result in recurrence, requiring additional surgery, usually via external approach.11,12 Open surgery includes midline, lateral, or superolateral thyrotomy, and supraglottic laryngectomy.6,12,13 Total laryngectomy is only reserved for selected cases of thyroid cartilage invasion or massive subglottic tumors. 14
The prognosis after the complete surgical removal of a paraganglioma is excellent. As presented in our case, pharyngotomy with submucosal dissection of the tumor may be a valuable surgical option instead of partial laryngectomy, even in large tumors. A more conservative external approach, which preserves the larynx, can easily be converted into a more radical resection if necessary.
Footnotes
Acknowledgements
The authors sincerely thank Vuk Živanović, whose comments and suggestions greatly improved the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.