
Abstract

Significant Statement
Spindle cell lipoma (SCL) commonly occurs in the subcutaneous tissue of the upper back, shoulder, and posterior neck, and SCL in the submandibular or parapharyngeal space is extremely rare. Because the radiological characteristics of SCL differ from those of lipoma, SCL should be considered as one of the differential diagnoses of submandibular lesions.
A 27-year-old woman was referred to our department with a painless swelling in the right submandibular region. The patient had no history of trauma, inflammation, or surgery in the submandibular region. The elastic soft mass was mobile. In computed tomography (CT) scan, a well-circumscribed, lobulated, heterogeneous low-density lesion with parapharyngeal extension (53 mm × 44 mm × 41 mm) was located lateral to the right submandibular gland (Figure 1A and B). Magnetic resonance imaging (MRI) showed a 53 mm × 49 mm × 41 mm well-circumscribed, heterogeneous submandibular lesion with low signal intensity in the T1-weighted image, intermediate signal intensity in T2-weighted image and fat-suppressed T2-weighted image, and no enhancement in gadolinium-enhanced T1-weighted image (Figure 1C–F). Ultrasonography revealed a heterogeneous, hypoechoic lesion without blood flow. Fine needle aspiration cytology showed an inadequate sample without a fluid component for the diagnosis. The lesion was clinically and radiologically diagnosed as a benign tumor. The lesion was removed in the submandibular approach under general anesthesia. The pathological diagnosis of the specimen was spindle cell lipoma (SCL) because microscopic images showed mature adipocytes, proliferated spindle cells, rope-like collagen fibers, and mucoid/fibrous stroma, and spindle cells were positive for CD34 in immunostaining (Figure 2). The postoperative course was uneventful without facial nerve palsy.
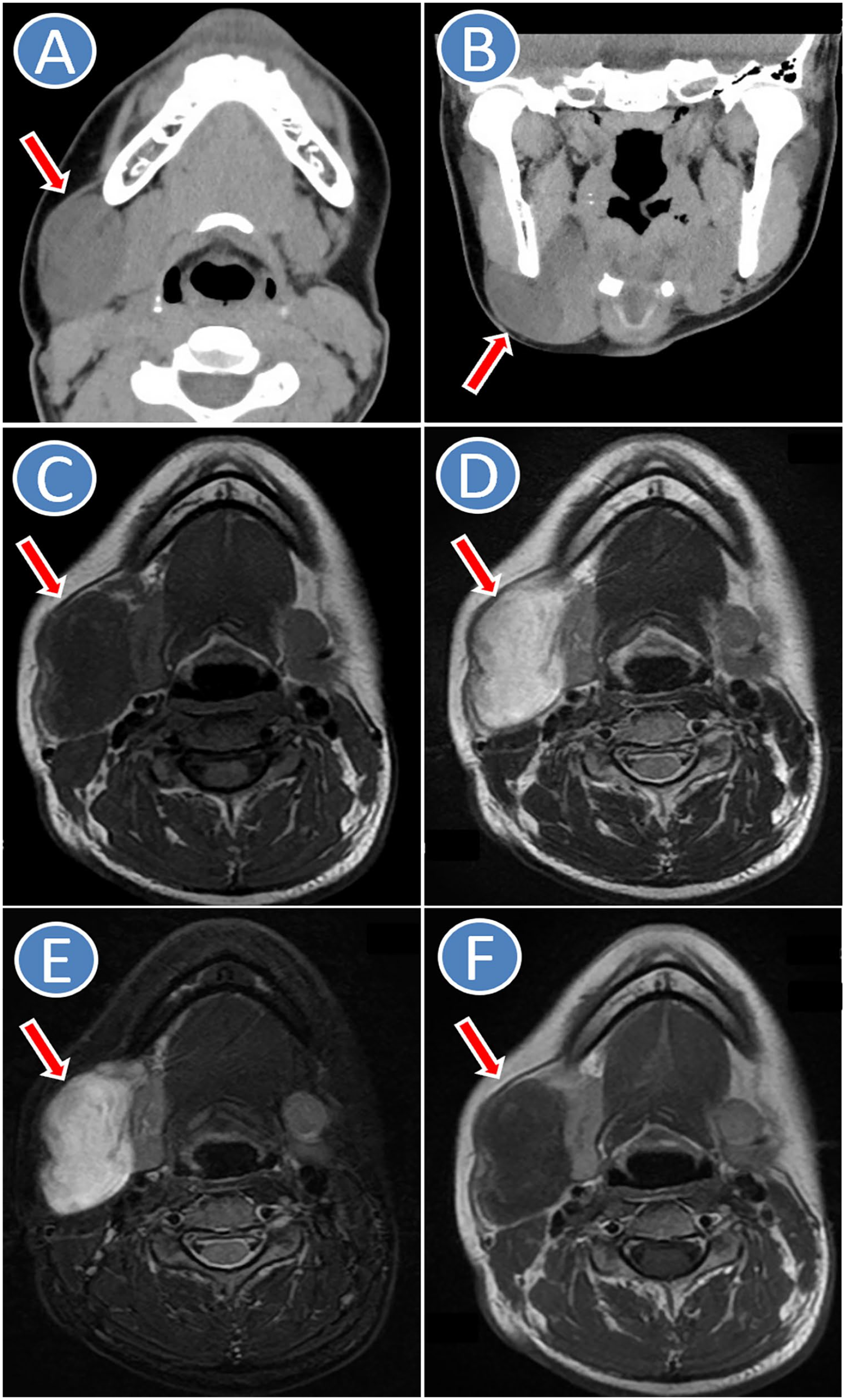
CT and MRI. Arrow indicates a lesion. (A) CT of axial image, (B) CT of coronal image, (C) MRI of T1-weighted axial image, (D) MRI of T2-weighted axial image, (E) MRI of fat-suppressed T2-weighted axial image, (F) MRI of gadolinium-enhanced T1-weighted axial image. CT, computed tomography; MRI, magnetic resonance imaging.
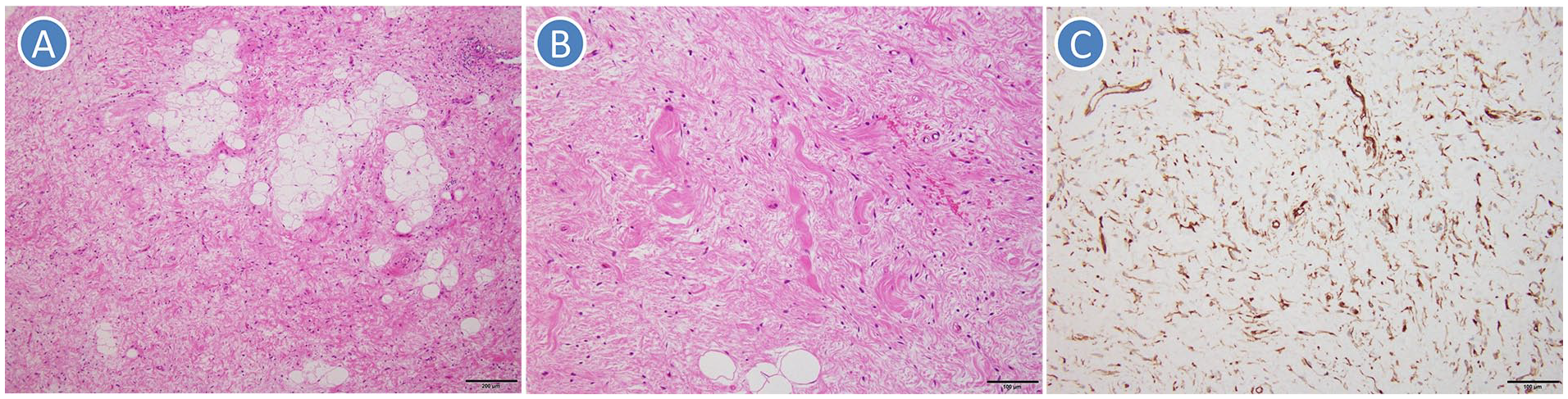
Microscopic pathology. The pathological diagnosis was spindle cell lipoma because microscopic images showed mature adipocytes, proliferated spindle cells, rope-like collagen fibers, and mucoid/fibrous stroma, and spindle cells were positive for CD34 in immunostaining. (A, B) Hematoxylin and eosin staining, (C) immunostaining (CD34).
SCL is an uncommon histological variant of lipoma that accounts for approximately 1.5% of all adipose tumors1,2 and is composed of mature adipocytes, uniformly proliferated spindle cells embedded within rope-like collagen fibers, and mucoid stroma. 3 Grossly, SCLs resemble ordinary lipomas, although they may be somewhat firmer, especially if the spindle cell component predominates. 1 SCLs occur most commonly in middle-aged men1,3,4 and are generally located in the subcutaneous tissue of the upper back, shoulder, and posterior neck.1-4 SCLs in the submandibular or parapharyngeal space are extremely rare,2,4 and the present case was a woman with submandibular SCL with parapharyngeal extension.
The submandibular space includes the submandibular gland, facial artery and vein, hypoglossal nerve, lymph nodes, and fat, 5 and has continuity with the sublingual space and parapharyngeal space. The clinical differential diagnosis of the submandibular lesion includes lipoma, plunging ranula, branchial cyst, dermoid/epidermoid cyst, submandibular gland tumor, vascular (lymphatic or venous) malformation, schwannoma, neurofibroma, lymphadenitis, malignant lymphoma, and lymph node metastasis.2,5 In the present case, the submandibular lesion without a fluid component was located at the lateral side of the submandibular gland and extended into the parapharyngeal space. Therefore, the preoperative diagnosis was a benign tumor such as schwannoma.
Lipomas show a homogeneous appearance with the same density as subcutaneous fat in CT images and show high signal intensity in both T1- and T2-weighted images. In contrast, SCLs have various imaging findings according to the ratio of adipose tissue.3,6 On MRI, SCLs reveal low signal intensity in T1-weighted images and intermediate to high signal intensity in T2-weighted images. 6 Various components of the adipose and nonadipose tissues may cause difficulty differentiating between SCL and other adipocytic tumors including liposarcoma radiologically.3,6 The other radiological differential diagnosis of SCL includes schwannoma and neurofibroma. 6 Although MRI signal characteristics of schwannomas overlap with that of SCLs, schwannomas show high-signal intensity in T2-weighted images. In conclusion, surgeons and radiologists should consider SCL in the differential radiological diagnosis of the submandibular lesion, although submandibular SCLs are very rare.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.