
Abstract
Cochlear implantation (CI) is the most effective solution for patients with severe-to-profound sensorineural hearing loss, especially in children. However, a major postoperative complication, known as chronic suppurative otitis media (CSOM), poses challenges for both doctors and families of the patients, which can affect post-CI hearing outcomes. We present the case of post-CI CSOM in a 15-year-old girl. She had been utilizing a unilateral cochlear implant for 7 years and had been experiencing intermittent earache and discharge in her only audible ear for the past 15 months. After antibiotic treatment failed to resolve her symptoms, we opted for a tympanomastoidectomy, and removed the receiver-stimulator package while keeping the electrode inside her cochlea. Simultaneously, we inserted an irrigation and drainage tube into the mastoid and middle ear space to discharge the exudate and control infection by applying topical antibiotics. The patient’s ear discharge had resolved within 1 month, and her tympanic membrane healed naturally. Our successful experience shows that antibiotic irrigation and draining have effectively controlled infection and accelerated wound healing in this patient with post-CI CSOM, and it further prompted the patient to undergo bilateral CI 9 months later.
Introduction
Cochlear implantation (CI) is the most effective solution for severe-to-profound hearing loss, generating electronic hearing through an electrode inserted into the cochlea by creating an opening in the inner ear. Furthermore, this surgery alters the structure of both the middle and inner ear. Deaf children are recommended to receive CI and restore hearing as early as less than age of 1 year, to avoid missing the critical period of language learning and social development. 1 Nevertheless, young age adds additional risks of complications during and after surgery, not to mention that a large portion of congenital deaf children also present with abnormalities in ear morphology.
Chronic suppurative otitis media (CSOM) is one of the major complications in children after CI, 2 presenting as recurrent infection and discharge in the middle ear. Without prompt treatment, the patient’s condition can deteriorate or become life-threatening. Middle ear infections can spread along the electrodes of cochlear implants, leading to labyrinthitis and meningitis. To date, to our knowledge, the post-CI CSOM management strategy remains a challenging issue. Antibiotic treatment is widely accepted globally and may necessitate surgical interventions in severe cases.3,4 If necessary, surgeons should consider removing the implant to control infection. However, due to economic and policy reasons, many children with bilateral deafness have chosen for unilateral CI in the past. Consequently, these patients have received auditory stimulation on only one side for years, making this their only audible ear. When performing implant on such children, surgeons would try to preserve their equipment or retain the electrode cable in situ for potential future ipsilateral reimplantation.
A cortical mastoidectomy procedure has decades of history in achieving long-term resolution of middle ear infection and otorrhea. 5 In addition to the standard cortical mastoidectomy, modern methods include the placement of a tube in the tympanic cavity to allow draining of necrotic tissue and secretions, and antibiotic irrigations. Topical irrigation ensures that a higher concentration or dosage of antibiotics acts specifically on the affected area. 6 However, this approach has not been previously reported in children with CI. We hypothesize that this method could be effective in clearing infections and preserving the electrode array in extreme cases. The following case introduced the use of an irrigation and drainage tube for post-CI CSOM management in a teenage girl.
Case Presentation
A 15-year-old girl presented with intermittent left earache and discharge for 15 months, occurring 7 years after undergoing left CI. The patient was diagnosed with bilateral sensorineural hearing loss when 1 year old. Both cochleae exhibit normal morphology, and there was also no evidence of a narrow internal auditory meatus. She had worn hearing aids until compensation became inadequate for school life. Due to financial constraints, the family chose to get a single CI. Fifteen months before, the patient had the first episode of otitis media on the left side, which was induced by an upper respiratory infection. She was diagnosed with “acute otitis media (left)” and treated with oral cephalosporins at a local hospital. Twelve months before, her symptoms recurred, which were managed similarly to previous episodes and eventually resolved. Seven months prior, she was diagnosed with CSOM and received treatment comprising intravenous cephalosporins and levofloxacin hydrochloride ear drops. However, her symptoms did not fully resolve, and she continued to experience intermittent ear discharge, sometimes purulent and sometimes containing blood. The family visited our clinic 2 weeks ago.
The girl was using a Cochlear Nucleus CI512 implant in the left ear, with an aided-4FPTA of 28 dB hearing level (HL); no residual hearing was detected in the unaided condition. The right ear was not fitted with any auxiliary hearing device and there was no response to maximum output in unaided condition. Using Mandarin speech test materials, the speech recognition score was 65% at 70 dB HL in quiet. Physical examination showed no redness or tumidness at the incision site or over the receiver-stimulator. We found purulent secretion and skin irritation in the left external auditory canal through otoscopic examination (Figure 1A). A large perforation existed on the tympanic membrane. Temporal bone computed tomography (CT) scan showed soft tissue shadows in the left mastoid cavity, the tympanic cavity, and the external auditory canal (Figure 2). The results of the bacterial culture indicated a methicillin-resistant Staphylococcus aureus infection.
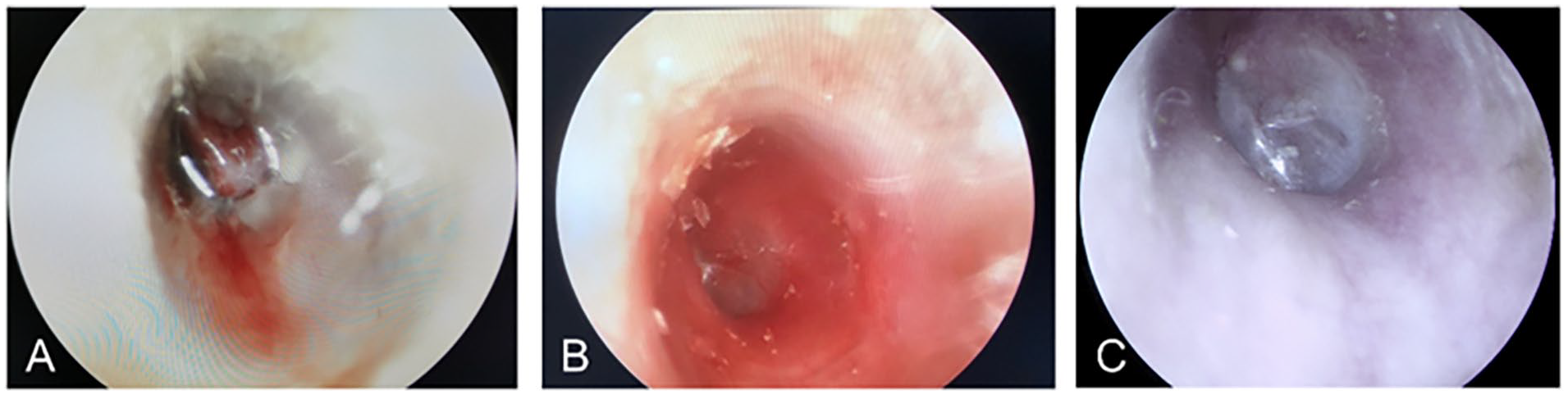
Otoscopic examinations. (A) Preoperative otoscopic examination showed a large perforation on the tympanic membrane. (B) Healed tympanic membrane at 1 month of follow-up after surgery. (C) Intact left tympanic membrane, no signs of inflammation at 9 months after surgery.
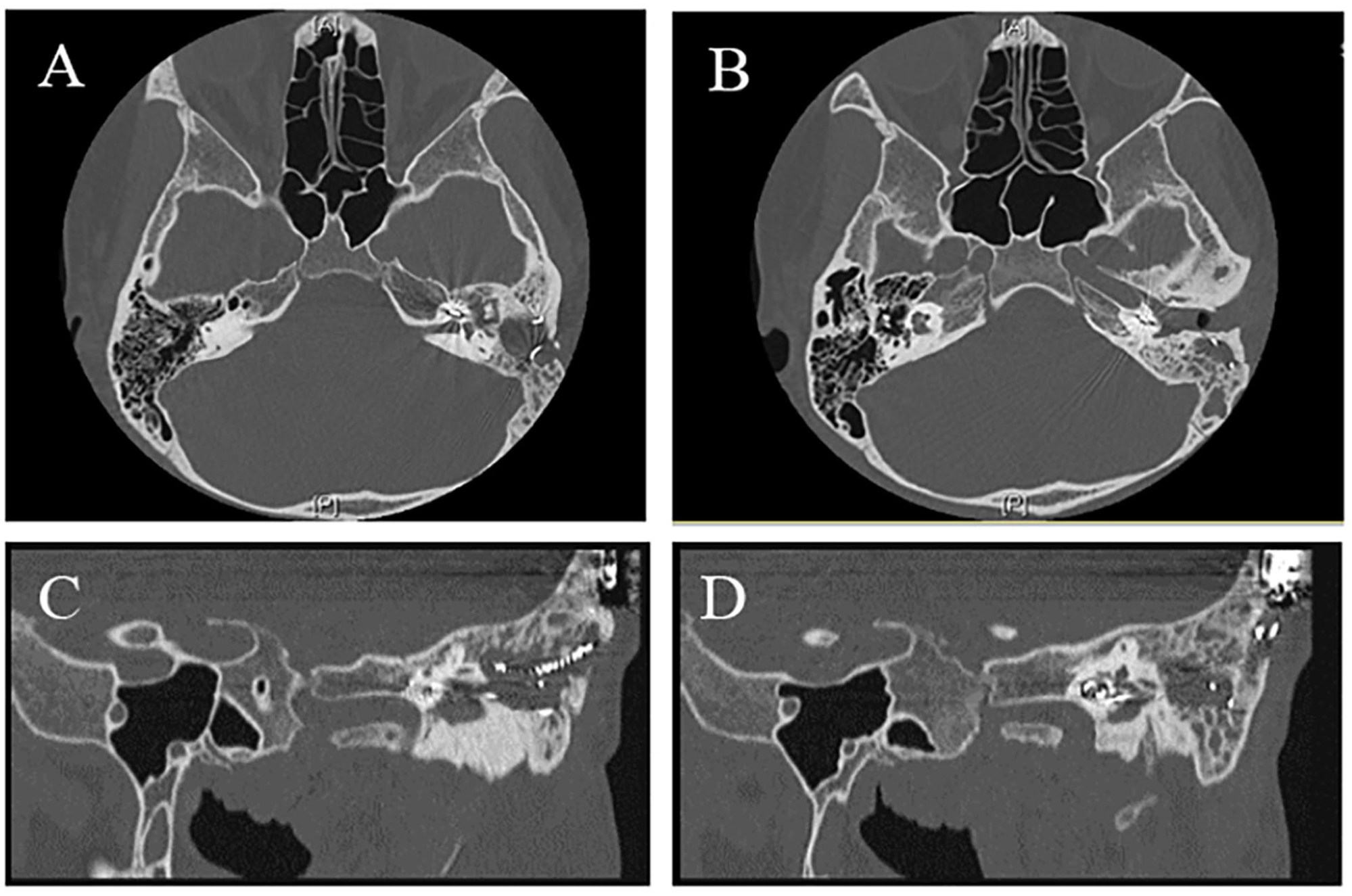
Preoperative temporal bone CT showed soft tissue shadow in the left mastoid cavity, tympanic cavity, and external auditory canal. (A and B) axial view; (C and D) oblique view on the left anterior. CT, computed tomography.
During the debridement surgery, we observed granulation tissue adhesion tightly to the electrode cable, as well as biofilm formation on the implant surface, which posed a challenge in retaining the implant. Since the implanted side had been her sole functional ear for years, part of the electrode was retained in the cochlea to prevent ossification and create an opportunity for reimplantation. We tried to minimize operations near the facial recess and the round window, but this could block the Eustachian tube drainage route. Thus, we placed a silicone catheter (outside diameter = 3.3 ± 0.33 mm) in her surgical cavity for irrigation and drainage.
After surgery, we gave the patient sulfamethoxazole compound tablets orally and levofloxacin hydrochloride ear drops for irrigation of the surgical cavity according to the results of the susceptible test. The catheter was used for local drug delivery and drainage every 2 days during the initial 2 weeks. The quantity and texture of drainage were monitored and assessed daily during rounding. The patient also received a 2-week course of oral antibiotics. The drainage volume gradually decreased and became almost clear in texture. The patient exhibited stable vital signs and no indications of middle ear or intracranial infection. However, there continued to be a daily discharge of 1 to 2 ml of secretion in the drainage tube, occasionally accompanied by flocculent tissue. We placed the tube with appropriate dressings and discharged the patient. Her condition was closely monitored. One month after surgery, the tube was removed during a follow-up visit. On removal of the tube (Figure 3B), the perforation of her tympanic membrane had naturally healed without surgical repair (Figure 1B), demonstrating a favorable healing process. The patient reported no discomfort with the procedure.
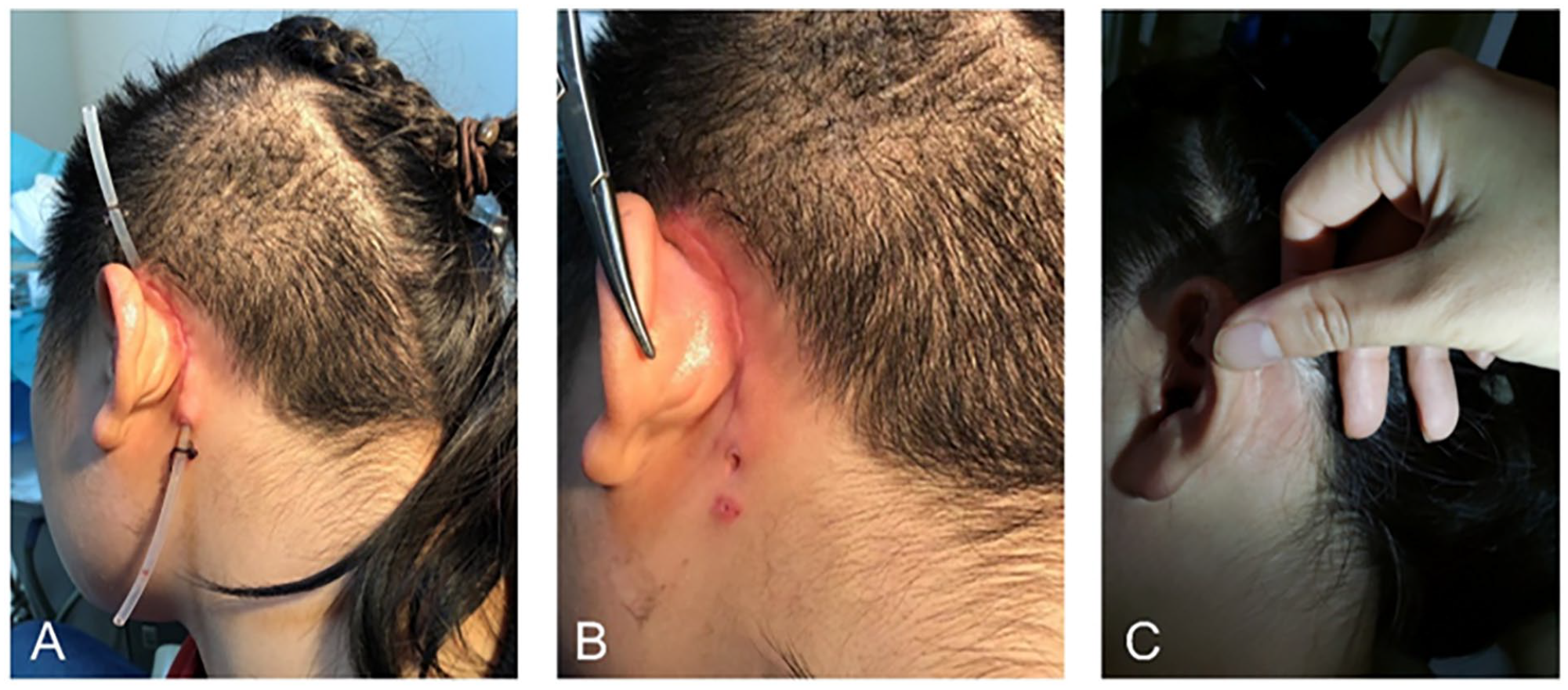
Photos of the incision area. (A) The irrigation and drainage tube for topical antibiotic treatment. (B) The incision after extubation. (C) The incision at 9 months of follow-up after surgery.
Nine months later, there was no recurrence of her ear symptoms. The girl was not fitted with any auxiliary hearing devices during the audiometric test and showed no response to the maximum output. Physical examination showed a healed incision site, no fistula formation (Figure 3C), an intact left tympanic membrane, and no signs of inflammation (Figure 1C). The temporal bone CT scan (Figure 4) showed the status of the implanted cochlear electrodes, the cleared tympanic cavity, and the improved mastoid situation (than before). Despite the girl typically reporting no difficulty in communicating with others using 1 ear, her academic performance and socialization lagged behind her peers as she grew older. Consequently, the family had contemplated bilateral CI. Her family was fully aware of the risks and agreed to the surgery.
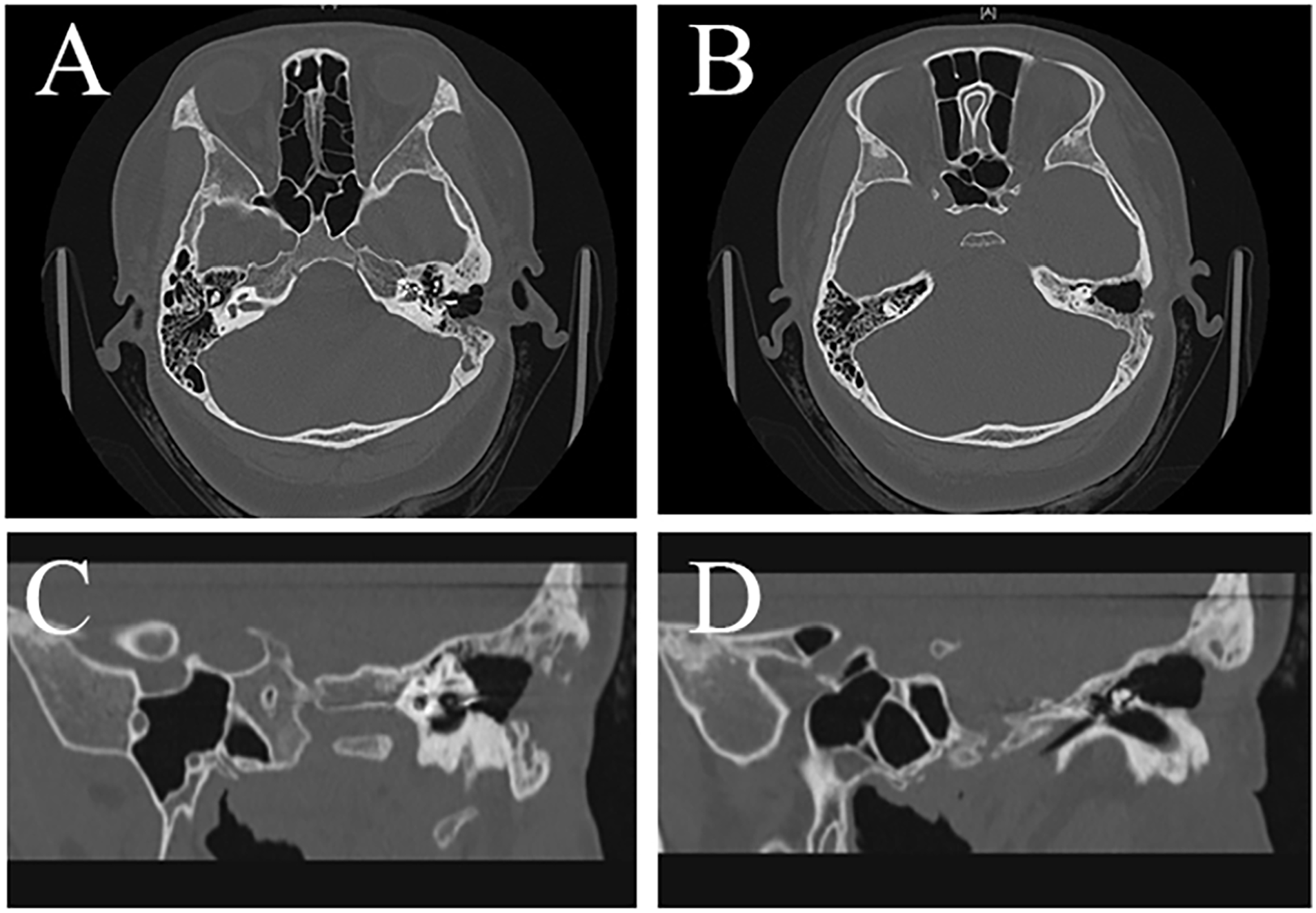
Temporal bone CT (9 months after surgery) showed the status of the implanted cochlear electrodes, the cleared tympanic cavity, and the improved mastoid situation. (A and B) axial view; (C and D) oblique view on the left anterior. CT, computed tomography.
One year after bilateral implantation, the patient wore Cochlear Nucleus CI512 implants in both ears. Aided-4FPTA was 28 dB HL in the left ear and 33 dB HL in the right ear. The speech recognition score in silence using both CI was 75% at 70 dB HL. When using the left CI only, the score was 50% at 70 dB HL; when using the right CI only, it was 30% at 70 dB HL. She had returned to school.
Discussion
CSOM is a common otological disease and sometimes appears as a delayed complication after CI. The appearance of symptoms of otitis media usually occurs in the first half year after CI. 7 Common symptoms include recurrent otorrhea, granulation tissue formation around the device, purulent wound breakdown, or fistula formation. 4 Pathogens such as S. aureus, Streptococcus pneumoniae, and Haemophilus influenzae are the most common postimplantation ear infections. 8 Some pathogens can form biofilms on the surface of biomaterials (ie, the receiver-simulator package), causing biomaterial-centered infections, which may be an essential reason for persistent and recurrent infections related to CIs. 9 S. aureus and Pseudomonas aeruginosa are often accompanied by biofilm formation, and the presence of biofilm in the body of the foreground appeared to be associated with a higher risk of explantation.8,10,11 Early application of systematic antibiotic therapy has become a global consensus,3,12 and the treatment with culture directed therapy could be associated with retention of the device and restriction of infection to the middle ear. 8 Frequent ear infections with otorrhea are the most typical symptoms preceding the decision to operate for CSOM, and the use of sensitive antibiotics could reduce the chance of explantation. 8 Cutting and leaving an electrode array in the cochlea may slow ossification of the inner ear and preserve the opportunity to reimplant ipsilaterally, 13 especially for monaural listeners.
While the placement of drainage tubes is widely used in surgical procedures, however, postoperative irrigation and drainage are less common in otological surgeries, especially in patients with CI. Jones et al 6 have confirmed the feasibility of postoperative irrigation and drainage in the management of CSOM adults, suggesting its suitability for challenging cases under conditions of failed tympanoplasty, antibiotic resistance, or an unsuitable middle ear environment. We initially applied this method to children with post-CI CSOM due to the urgent need to preserve the electrode for reimplantation and the presence of significant middle ear scarring, which hindered middle ear drainage and potentially retained infection, necessitating local antibiotic solution irrigation and drainage of secretions. A mastoid intubation introduced a new route for topical antibiotics and drainage of the middle ear, aiming to control infection and minimize electrode detachment. A previous article by Low et al 14 introduced a similar approach in a case of post-CI wound abscess, where a tube was adopted at the incision site for daily topical antibiotic irrigation.
We present this case to share our experience and raise awareness among surgeons. This effective postoperative management approach can be applied to children with cochlear implants, potentially improving prognosis and reducing the occurrence of cochlear implant explantation. Moreover, due to our successful treatment, the family is delighted with the prognosis and has placed great trust in our team. After fully understanding the risks, they have chosen to undergo bilateral cochlear implant reimplantation.
Further evidence is necessary to solidify these findings. In addition, when using an irrigation and drainage tube, surgeons must be careful with evidence of secondary infection, such as cloudy drainage fluid, red and swollen wounds, pain, and fever. If necessary, conduct bacterial culture with secretion regularly. We maintained the tube for 1 month to ensure complete drainage, although the surrounding skin was slightly irritated after extubation, likely caused by foreign body stimulation. Once again, doctors must adjust the plan based on the individual circumstances of the patient.
Conclusions
Our case suggests that in children with post-CI CSOM, irrigation and drainage of mastoid cavity effectively controls infection and expedites wound healing, potentially preventing electrode detachment. We chose this method because the patient’s lesions had spread to the facial recess and the upper tympanum and her implanted side was her only audible ear. Nonetheless, surgeons must be aware of the risk of secondary infection when using drainage tubes and adjust the plan according to the patient’s condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Beijing Hospitals Authority Clinical Medicine Development of Special funding support (grant number: ZLRK202307), the National Natural Science Foundation of China (grant number: 82371943), the Beijing Chao-Yang Hospital Multi-disciplinary Team Program (grant number: CYDXK202201), and the Capital’s Fund for Health Improvement and Research (grant number: 2020-1-2032).