
Abstract
Vestibular neurectomy is an effective method eliminating vertigo attacks in patients suffering from disabling Meniere’s disease with no clinical improvement despite conservative and intratympanic therapy. Magnetic resonance imaging allows in vivo evaluation of changes manifesting in the inner ear after treatment; however, downgrading of the endolymphatic hydrops after vestibular neurectomy had not been previously described in the literature. In the present article, a case of a patient with unilateral severe Meniere’s disease treated with selective vestibular nerve section from middle fossa approach was described. Clinical symptoms and audiovestibular tests were evaluated before and 13 months after the surgery. Complete resolution of vertigo episodes and hearing preservation was achieved. Magnetic resonance imaging was performed before and after the surgery using a 3 Tesla scanner with dedicated protocol after intravenous administration of gadolinium contrast agent. In the follow-up examination, regression of the cochlear and vestibular endolymphatic hydrops was visualized, which may suggest processes occurring in the labyrinth as a result of the vestibular efferent fibers section.
Introduction
Meniere’s disease (MD) is a chronic inner ear disorder characterized by recurrent episodes of vertigo accompanied by tinnitus, aural fullness, and hearing loss. According to the American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNS) guidelines, 1 diagnosis is based on clinical manifestation and pure-tone audiometry. Nevertheless, recent development of magnetic resonance imaging (MRI) created an opportunity to visualize in vivo endolymphatic hydrops (EH) considered as the underlying pathological hallmark of MD. Gadolinium contrast agent delivered intratympanic or intravenous accumulates in the perilymph, while the endolymphatic space is visualized as partial loss of contrast enhancement. Several protocols and grading scales were established and high sensitivity of that method was demonstrated in the literature.2-4 Moreover, repeated MRI examinations enable evaluation of changes in degree of EH during the natural course of MD and after treatment as well.5-12 Therefore, the protocol of repeated MRI was scheduled in our department to visualize potential changes after the surgery. Nevertheless, to our best knowledge, downgrading of the EH after vestibular neurectomy had not been previously described in the literature.
Case Report
A 53-year-old male with a 21 year history of MD was admitted to the tertiary hospital for comprehensive audiovestibular diagnostic evaluation. The patient reported recurrent episodes of spontaneous spinning vertigo accompanied by tinnitus, aural fullness, and hearing loss in the right ear. Initially, conservative treatment with betahistine 48 mg/day was implemented with satisfactory clinical improvement for 10 years. Subsequently, attacks became more frequent, with tinnitus and hearing loss persisted during the interattack periods. Despite intensified conservative treatment with hydrochlorothiazide 25 mg/day and 2 series of intratympanic steroid therapy (dexamethasone 4 mg, 4 injections in a course, repeated every 6 months), patient suffered from disabling MD attacks. During diagnostic hospitalization, he self-assessed the intensity of main symptoms over the past 6 months as follows: vertigo episodes on average 5.83 times per month, tinnitus at 3, aural fulness at 4, balance problems at 4 on the scale of 0 to 6 proposed by Arenberg and Stahle. 13 Functional level was assessed according to the AAO-HNS 1 to 6 scale to grade 4. Pure-tone audiometry revealed pantonal sensorineural hearing loss in the right ear with the pure-tone average (PTA) of 46.25 dB hearing level (HL) and characteristic audiogram pattern with elevated thresholds for low-frequency tones (Figure 1a). Auditory brainstem response test indicated cochlear hearing loss in the right ear. Transtympanic electrocochleography showed an elevated summating potential to action potential ratio (SP/AP amplitude ratio 0.93). Unilateral vestibular weakness (asymmetry >25%) was confirmed using bithermal caloric test during videonystagmography.
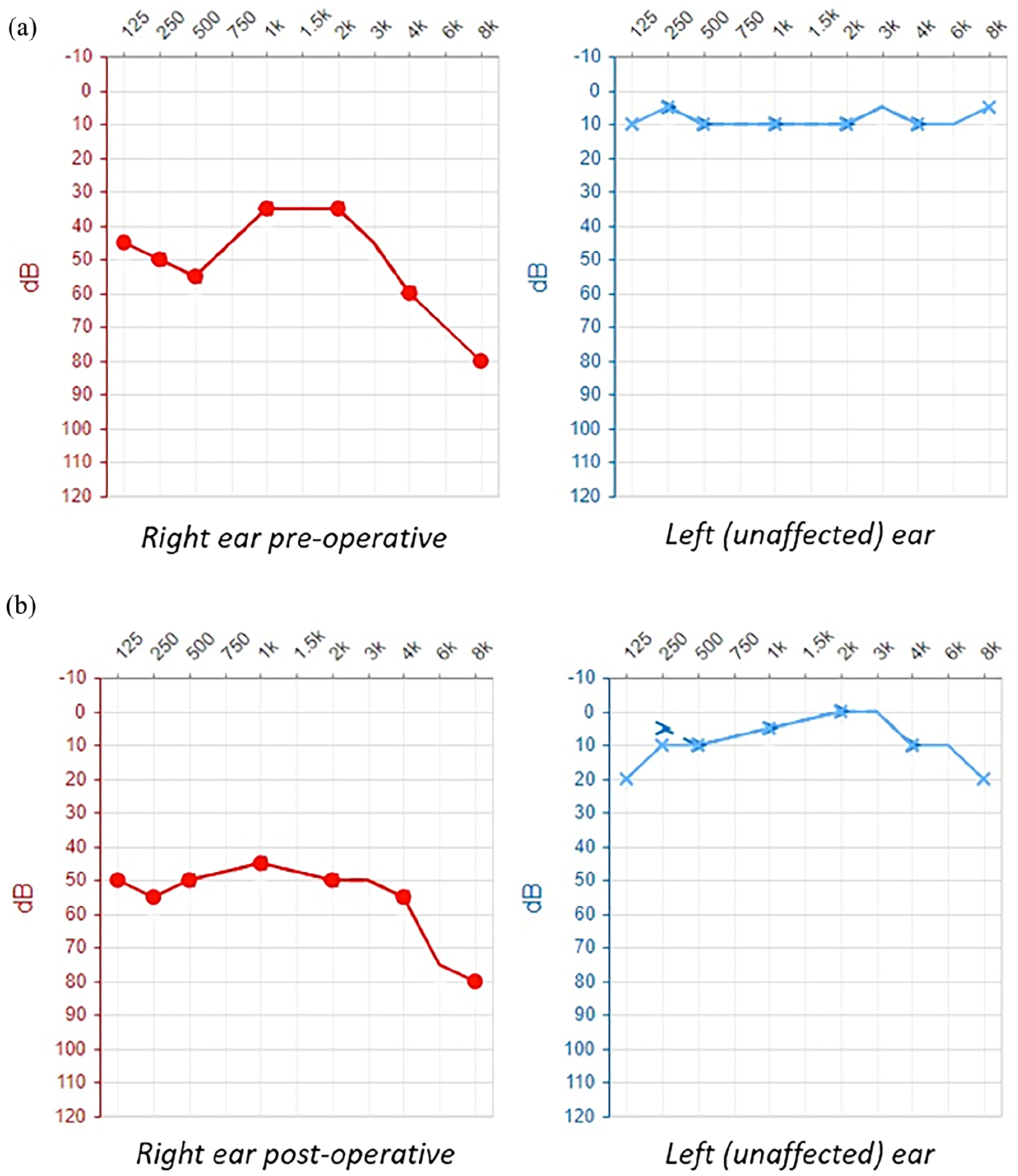
Pure-tone audiometry test results. (a) Preoperative examination—pantonal sensorineural hearing loss in the right ear with the PTA of 46.25 dB HL. (b) Postoperative examination performed 13 months after the vestibular nerve section—stable level of hearing with the PTA of 50 dB HL in the right ear. PTA, pure-tone average; dB HL, decibels hearing level.
Radiologic examination was performed using a 3 Tesla MRI scanner with dedicated protocol 4 hours after intravenous administration of a double dose of gadolinium contrast agent as reported in previous studies.14,15 Endolymphatic space of the cochlea and the vestibule were evaluated separately according to the Barath scale modified by Bernaerts.3,4 In the right cochlea, partial obstruction of the scala vestibuli by dilated endolymphatic duct was visualized indicating grade 1 cochlear EH (Figure 2c). Dilated and confluent saccule and utricle with circular enhancing perilymphatic space in the right vestibule corresponded to grade 2 vestibular EH (Figure 2d). The perilymphatic enhancement of the cochlea in the right ear was symmetrical with the asymptomatic left ear.
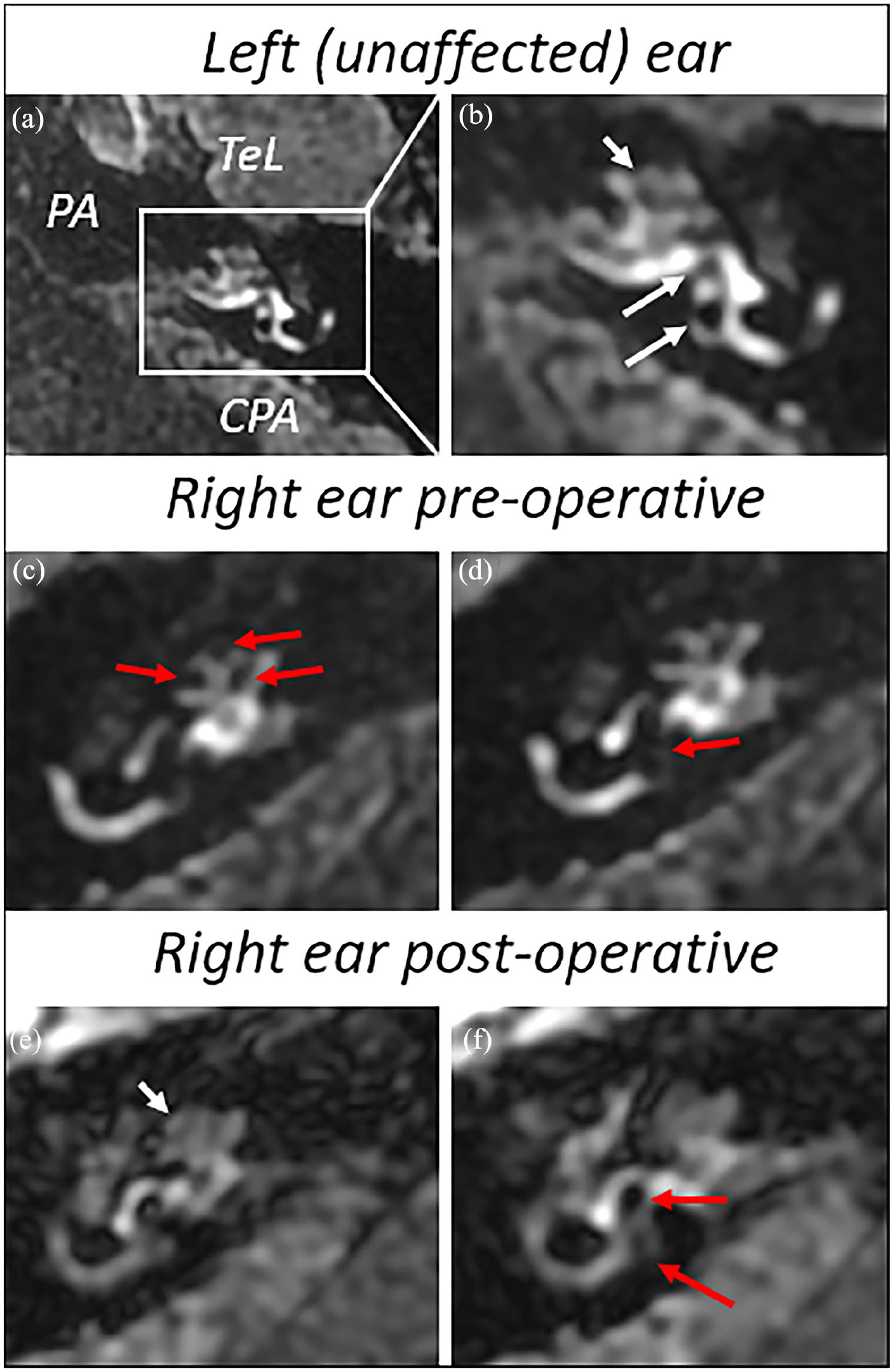
MRI 3D-FLAIR sequences compared between the ears—the cochlea’s endolymphatic space and the vestibule were evaluated separately using the Barath scale modified by Bernaerts. According to the Bernaerts classification, the contrast enhancement of the cochlea in the affected ear was assessed and compared to the asymptomatic opposite side. (a) General view of left (unaffected) ear. (b) Detailed view of left labyrinth shows normal enhancement of perilymph in the cochlea (short white arrow) and around saccule (upper long white arrow) and utricle (lower long white arrow). (c) Detailed view of right cochlea shows preoperative cochlear EH grade 1 (nodular nonenhancing regions pointed with red arrows). (d) Detailed view of right vestibule shows preoperative vestibular EH grade 2 (red arrow points dilatation of saccule and utricle with circular enhancing perilymphatic space). (e) Detailed view of postoperative status shows regression of cochlear EH to grade 0 (white arrow). (f) Detailed view of postoperative status shows downgrading of vestibular EH to grade 1 (red arrows). MRI, magnetic resonance imaging; 3D-FLAIR, 3D fluid-attenuated inversion recovery; TeL, temporal lobe; PA, petrous apex; CPA, cerebellopontine angle; EH, endolymphatic hydrops.
As the patient suffered from uncontrollable MD, defined as persistent vertigo attacks with no clinical improvement after 6 months of conservative treatment, a selective vestibular neurectomy through the middle fossa approach was performed. The postoperative period was uncomplicated and the patient was discharged home on the eighth day after the surgery.
At the follow-up visit, 13 months after the surgery, patient reported complete resolution of vertigo. Tinnitus, aural fulness, and balance problems decreased to levels 2, 0, and 1, respectively, on the aforementioned scale. Hearing in the operated ear was preserved with PTA level of 50 dB HL (Figure 1b). Total vestibular neurectomy was confirmed using bithermal caloric test and video head impulse test. In the postoperative MRI scans, complete regression of the cochlear EH (Figure 2e) and downgrading of the vestibular EH to extra-low grade 1 was visualized (Figure 2f).
Discussion
Selective vestibular neurectomy is known to be an effective treatment in patients with disabling MD presenting no clinical improvement despite conservative and intratympanic therapy. Complete resolution of vertigo attacks is reported in over 90% of patients.16-18 Furthermore, it allows for hearing preservation in 76% to 98% patients with postoperative hearing deterioration not exceeding 10 dB.16,17 Although the clinical outcome remains the most important in assessing the treatment effectiveness, possibility of inner ear in vivo visualization may help the follow-up evaluation. Changes in EH after various conservative and surgical treatment was described over the past few years.5-12 Gürkov et al 6 analyzed MRI examinations of patients treated with standard-dose betahistine and visualized no regression of EH in that population. Still, a regression of EH in 3 out of 20 symptomatic ears in the group of 12 patients with MD treated conservatively for at least 1 year was described by Suga et al. 7 Recently, a case of EH withdrawal was visualized in a patient treated with intratympanic steroids. 8 Fiorino et al 9 investigated changes in EH after intratympanic gentamicin injections in 8 patients with definite MD. In 4 patients, no change in the EH degree was observed, while the remaining 4 showed a progression endolymphatic space dilatation. Numerous studies have analyzed follow-up MRI examinations after endolymphatic sac drainage. Ito et al 10 reported volumetric changes in the endolymphatic space in patients with vertigo resolution after endolymphatic sac drainage with steroid application. Meanwhile, Liu et al 11 examined the endolymphatic space in 4 patients experiencing persistent vertigo despite the surgical intervention and revealed the persistence of EH in these patients. The results discussed above may suggest a correlation between vertigo control and regression of EH in patients after endolymphatic sac drainage. In the recent study analyzing 4 patients 8 months after vestibular neurectomy, no changes in EH severity was visualized; however, regression of asymmetrical perilymphatic enhancement was found postoperatively. 12 That phenomenon may suggest processes occurring after labyrinth denervation resulting from the section of the vestibular efferent fibers. Regression of EH visualized in the present study may indicate that exceeded follow-up period and repeated MRI examinations would be essential to observe changes in endolymphatic space after vestibular denervation. Nevertheless, further studies with larger patient groups are needed to investigate this issue comprehensively.
Conclusion
The treatment of MD follows an escalating strategy, starting with dietary and pharmacological recommendations and culminating in surgical methods. While clinical outcomes remain crucial in assessing treatment effectiveness, in vivo visualization of the endolymphatic space may be helpful in follow-up assessment. In the present case report, regression of the EH after vestibular neurectomy was described for the first time. Further studies analyzing changes in the inner ear occurring after vestibular denervation would be essential for understanding the pathogenesis of MD.
Footnotes
Authors’ Note
The authors declare that this article has not been published elsewhere and is not under consideration by another journal. The authors declare that the study complies with the current law in Poland.
Data Availability
Please contact authors for data requests (Tomasz Wojciechowski, MD, PhD— email:
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This retrospective study abides by the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from the patient for publication of this case report.