
Abstract

Significant Statement
Epineurial pseudocysts of the facial nerve are benign, usually asymptomatic lesions. Radiologic detection and recognition of these lesions, which may also be bilateral, are important both in terms of informing the surgeon, especially in cases of cochlear implantation, and preventing unnecessary surgery and follow-up.
A 26-year-old male patient presented to the otolaryngology clinic with bilateral hearing loss. The patient had no history of trauma, surgery, or known medical conditions. Otoscopic examination and audiometric testing were normal. A noncontrast temporal computed tomography (CT) scan showed a hypodense image in the mastoid segment of the bilateral facial nerves, measuring 7 mm × 5 mm on the right and 6 mm × 5 mm on the left. The lesions were posterolateral to the facial nerve and well circumscribed (Figure 1). There were no other findings. A contrast-enhanced temporal magnetic resonance imaging (MRI) scan was performed with a preliminary diagnosis of a possible mass of the facial nerve. The lesions were heterogeneously hypointense on T1-weighted images and heterogeneously hyperintense on T2-weighted images. There was no diffusion restriction in the lesions and no contrast enhancement was observed on post-contrast sections (Figure 2). On the basis of the available images, bilateral epineurial pseudocysts were diagnosed and the patient was kept under clinical observation.
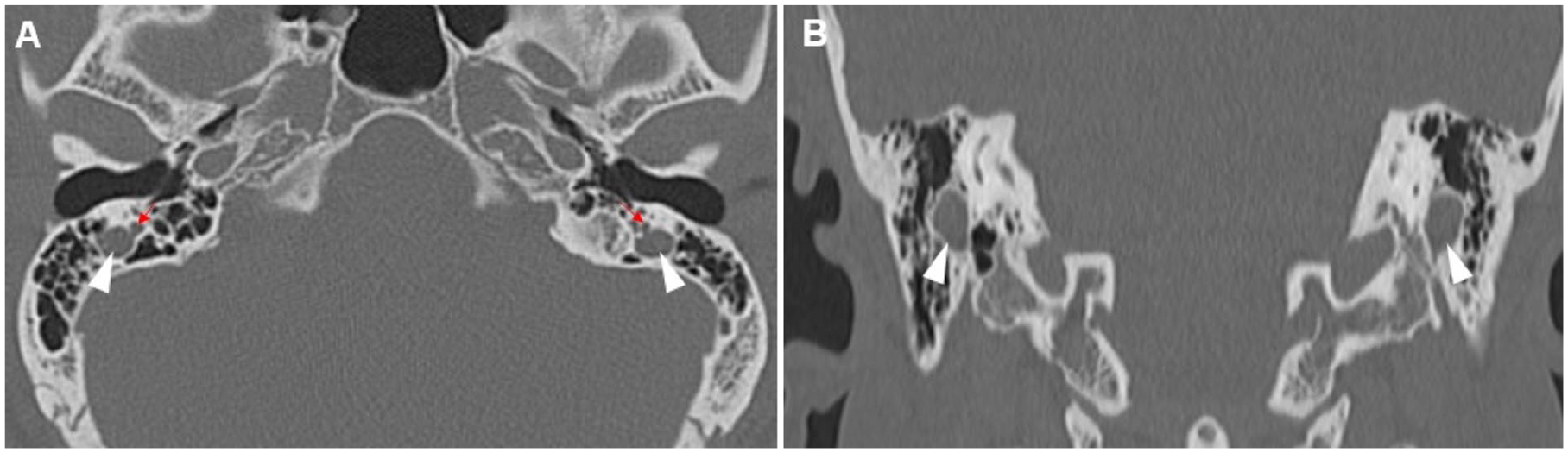
Axial (A) and coronal (B) noncontrast temporal CT images show smoothly circumscribed soft tissue dense lesions (arrowheads) posterior-lateral to the mastoid segment of bilateral facial nerve (red arrows). CT, computed tomography.
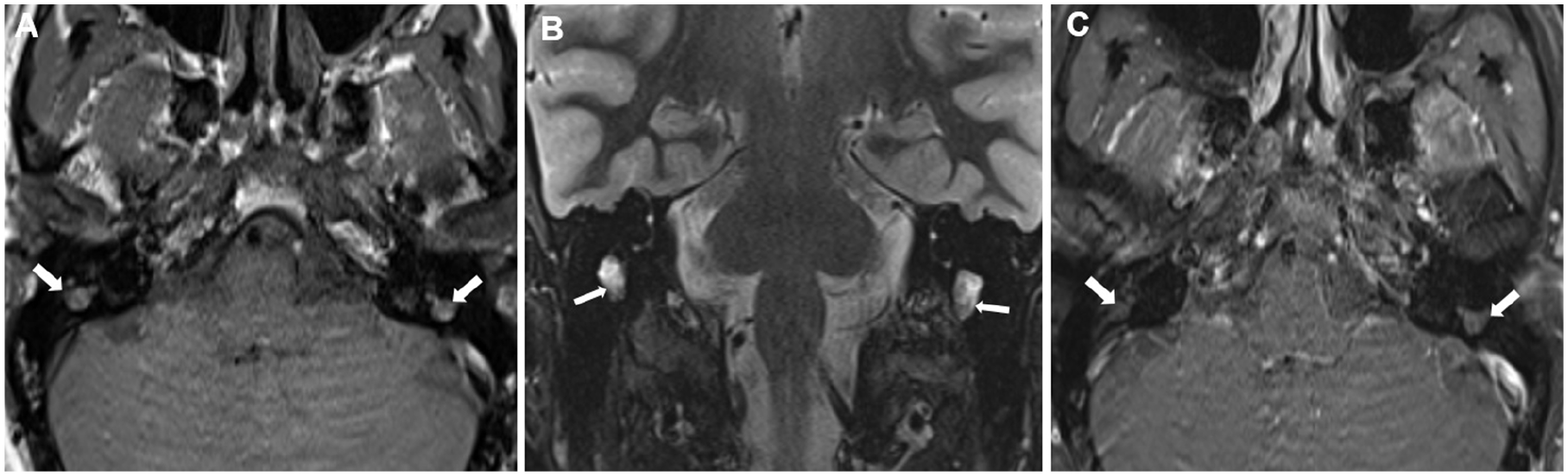
MR imaging shows hypointense lesions (arrows) with hyperintense areas on T1-weighted axial section (A) and heterogeneous hyperechoic lesions (arrows) on coronal section T2-weighted image (B) in the mastoid segment of bilateral facial nerve tracing. Post-contrast T1-weighted axial section (C) shows no contrast enhancement of the lesions. MR, magnetic resonance.
Epineurial pseudocysts of the intratemporal facial nerve were first described by Pertzborn et al in 2003 and there are very few studies in the literature.1-3 These rare benign lesions involving the mastoid segment of the facial nerve are usually discovered incidentally or during surgery. Histopathologically, it has been described as an amorphous stroma containing fibrovascular tissue with no real wall, no neural tissue, and no malignancy. 1 Its embryological origin is not yet known and it occurs bilaterally in 33% to 50% of cases.2,3 Although facial nerve symptoms were found in 3/7 cases when it was first described, no association has been found in subsequent studies. At surgery, it is seen as a soft, balloon-like, pedunculated lesion with a fibrous sheath and continuity with the epineurium, adjacent to the mastoid segment of the facial nerve. On CT, it appears as a well-circumscribed, round-oval area of soft tissue density, often located posterior to the mastoid segment of the facial nerve. On MRI, depending on its content, it is iso-hyperintense on T1-weighted images and hyperintense on T2-weighted images, with increased diffusion. It shows no or minimal rim enhancing enhancement. Differential diagnosis includes cholesteatoma, mastoid cell inflammation, and facial nerve masses (eg, schwannoma, hemangioma). Cholesteatoma can be distinguished by destruction of bone structure and diffusion restriction. In mastoiditis, the mastoid cell is more involved. Mass lesions have a more expansile and irregular border and contrast enhancement on postcontrast series. Calcification may be present in hemangiomas.2-5 As it is found to be stable on follow-up, it does not require treatment unless symptomatic. Symptomatic cases are treated with surgery.1-3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.