
Abstract

Significant Statement
Laryngeal granulomas are caused by trauma. Typical treatment strategies range from anti-reflux medications, voice therapy, and botulinum toxin injection to surgical excision. In the setting of obstructing laryngeal granulomas, airway preservation and safety are paramount. Short-term high-dose oral steroids may cause regression of even obstructing granulomas.
The patient was a 73-year-old male who described his voice as hoarse, breathy, coarse, raspy, weak, and with occasional stridor. He had undergone numerous procedures to improve his voice, most recently microdirect medialization laryngoplasty with abdominal fat harvest and bilateral true vocal fold injection, 3 months prior to this visit. His most recent surgery had been upper esophagogastroduodenoscopy (EGD) with dilation of distal esophageal strictures 2 months prior to his current visit. On strobovideolaryngoscopy, he was found to have a subglottic granuloma occupying nearly 50% of his subglottis (Figure 1). The etiology of the granuloma is unknown. Surgery for fat injection can cause granuloma, but they usually occur within a week of surgery and at the injection site. He had no granuloma during 1 week and 6 weeks postoperative assessments. They can also be caused by laryngopharyngeal reflux, but those granulomas usually are supraglottic. He was not intubated for his EGD. Because the patient and his wife planned to travel during the next 2 weeks, the decision was made to treat with high-dose steroids. Prednisone 60 mg PO daily was prescribed for 7 days and to be followed by reexamination.
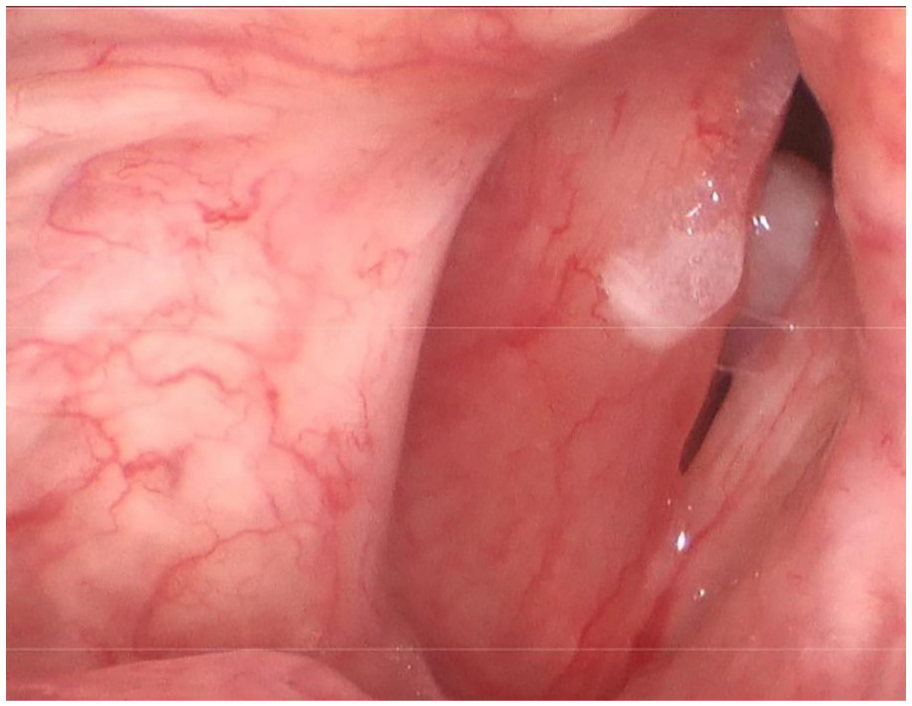
Laryngeal stroboscopy prior to treatment demonstrated a large subglottic granuloma occupying nearly 50% of the glottic airway. Also noted is an endolaryngeal secretion seen on the right true vocal fold.
At follow-up 7 days later, the subglottic granuloma had decreased in size (Figure 2) from nearly 50% to <10% obstruction. The patient reported less stridor and was felt to have an airway safe enough to permit his planned travel. If he had not responded, in-office resection or vaporization would have been considered.

Laryngeal stroboscopy 1 week after treatment with high-dose oral prednisone demonstrated a widely patent glottic inlet.
A laryngeal granuloma is not a true granuloma as seen in tuberculosis or sarcoidosis. 1 Histologically, they consist of granulation tissue, accompanying edema, “inflammatory infiltration with neovascularization,” and fibrosis with a top layer of squamous epithelium. 2
Therefore, they are a visual manifestation of inflammatory changes. Granulomas found in the larynx may be unilateral or bilateral and variable in color ranging from white to dark red. The granuloma is generally pedicled, may have an irregular or smooth appearance, and typically is found on the medial or superior edge of the vocal folds.2,3 Granulomas are sequelae of laryngeal trauma including endotracheal intubation, infections, reflux, phonotrauma, and idiopathic causes.3-6 The incidence of subglottic granuloma formation is said to range from 0.01% to 3.5%. 5
Predisposing factors include having a short neck, obesity, female sex, and other congenital airway abnormalities. 7 Laryngeal granulomas may threaten a patient’s airway safety and may cause severe respiratory symptoms. Symptoms may include cough, shortness of breath, chest discomfort, stridor, and may cause airway obstruction. They may also be asymptomatic. Because our patient had plans to travel in the near future, acute noninvasive treatment was attempted to eliminate airway compromise and permit the patient’s travels as atraumatically as possible.
The treatment options for laryngeal granulomas range from conservative management consisting of voice therapy, smoking cessation, corticosteroids, antibiotics, botulinum toxin, anti-reflux therapies, as well as surgical removal if needed. 5 For granulomas that recur, repeated excision may be necessary 8 but controlling underlying etiologies often voids recurrences and repeated surgery.
First-line standard therapy for laryngeal granulomas may include oral corticosteroids. 9 Steroids have well-established anti-inflammatory and immunosuppressive effects. 10 Despite the promising anti-inflammatory effects of steroids as well as clinical experience, research data and the efficacy of these medicines are not well established for treatment of laryngeal granulomas.11,12
The successful reduction of the size of this patient’s laryngeal granuloma with short-term treatment of oral corticosteroids demonstrates a conservative option for the treatment of even large laryngeal granulomas. More research on the treatment of laryngeal granulomas is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.