
Abstract
Significant Statement
We present a rare case of barotrauma-related complications secondary to transtracheal jet ventilation during endoscopic airway surgery. Severe subglottic stenosis obstructed the ventilatory expiratory pathway, resulting in increased airway and alveolar pressure, subsequent pneumothoraces (tension and conventional), pneumomediastinum, pneumoperitoneum, and head-to-toe subcutaneous emphysema. Heightened awareness of barotrauma-related injuries when using jet ventilation is essential to promptly diagnose and treat these complications.
Case Description
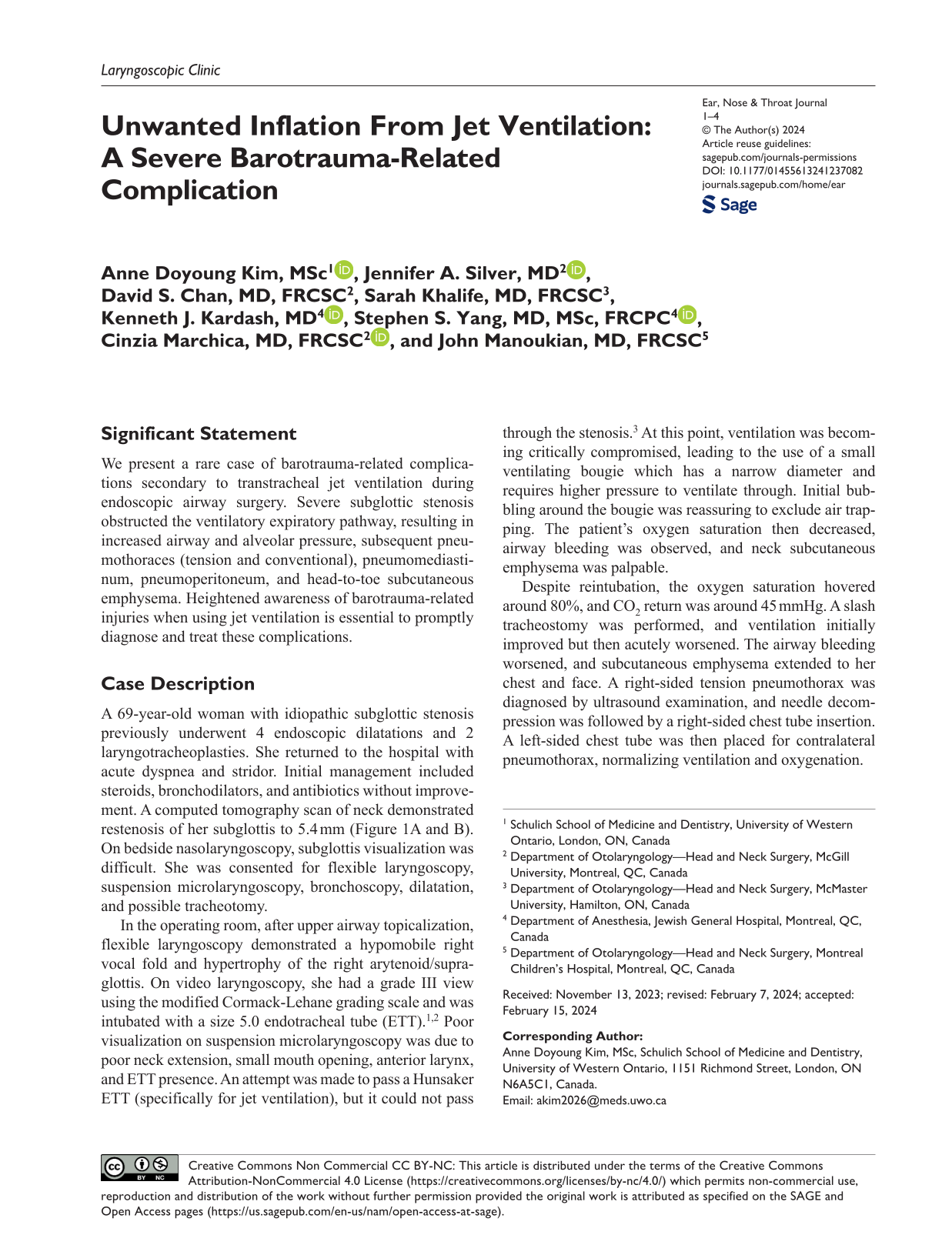
A 69-year-old woman with idiopathic subglottic stenosis previously underwent 4 endoscopic dilatations and 2 laryngotracheoplasties. She returned to the hospital with acute dyspnea and stridor. Initial management included steroids, bronchodilators, and antibiotics without improvement. A computed tomography scan of neck demonstrated restenosis of her subglottis to 5.4 mm (Figure 1A and B). On bedside nasolaryngoscopy, subglottis visualization was difficult. She was consented for flexible laryngoscopy, suspension microlaryngoscopy, bronchoscopy, dilatation, and possible tracheotomy.

Preoperative CT scan demonstrating critical subglottic stenosis in the (A) axial plane and (B) coronal plane. CT, computed tomography.
In the operating room, after upper airway topicalization, flexible laryngoscopy demonstrated a hypomobile right vocal fold and hypertrophy of the right arytenoid/supraglottis. On video laryngoscopy, she had a grade III view using the modified Cormack-Lehane grading scale and was intubated with a size 5.0 endotracheal tube (ETT).1,2 Poor visualization on suspension microlaryngoscopy was due to poor neck extension, small mouth opening, anterior larynx, and ETT presence. An attempt was made to pass a Hunsaker ETT (specifically for jet ventilation), but it could not pass through the stenosis. 3 At this point, ventilation was becoming critically compromised, leading to the use of a small ventilating bougie which has a narrow diameter and requires higher pressure to ventilate through. Initial bubbling around the bougie was reassuring to exclude air trapping. The patient’s oxygen saturation then decreased, airway bleeding was observed, and neck subcutaneous emphysema was palpable.
Despite reintubation, the oxygen saturation hovered around 80%, and CO2 return was around 45 mmHg. A slash tracheostomy was performed, and ventilation initially improved but then acutely worsened. The airway bleeding worsened, and subcutaneous emphysema extended to her chest and face. A right-sided tension pneumothorax was diagnosed by ultrasound examination, and needle decompression was followed by a right-sided chest tube insertion. A left-sided chest tube was then placed for contralateral pneumothorax, normalizing ventilation and oxygenation.
She was transferred to the intensive care unit to assess her barotrauma-related complications. She had significant head-to-toe subcutaneous emphysema (Figure 2A), pneumomediastinum, and pneumoperitoneum with no intraabdominal cause identified (Figure 2B).
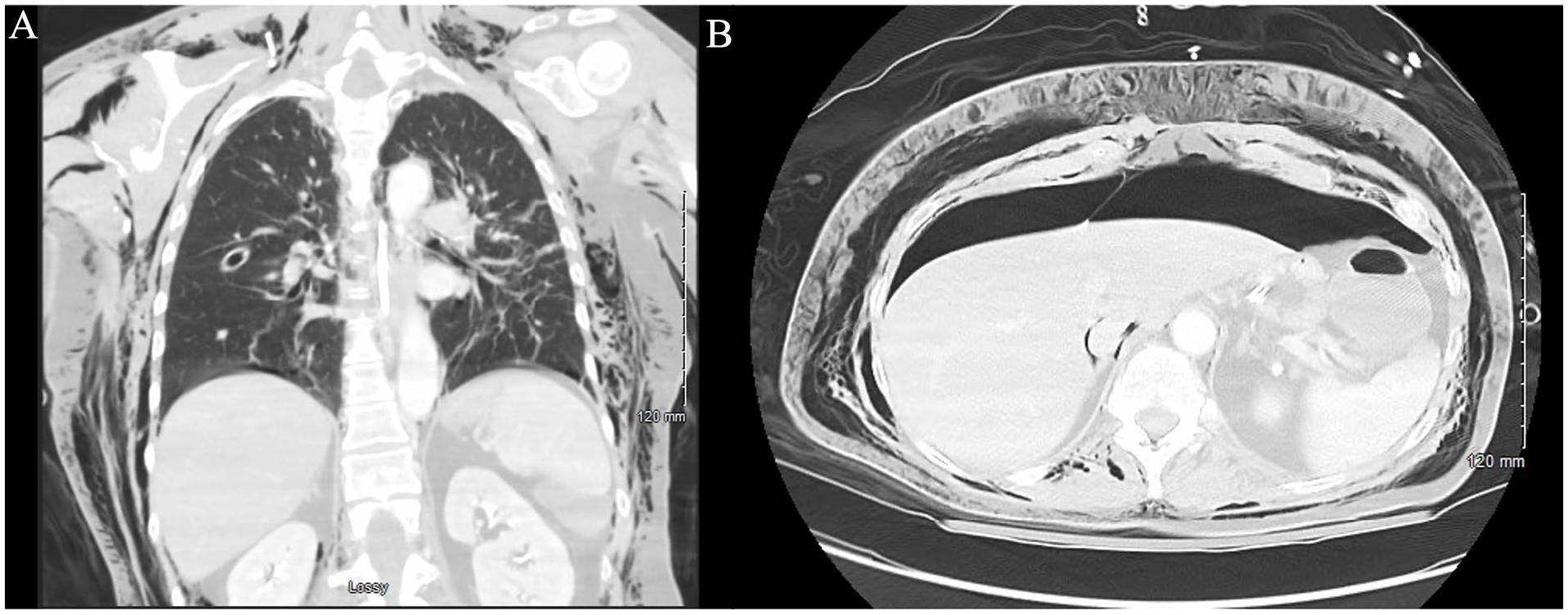
Postoperative evidence of significant (A) subcutaneous emphysema and (B) pneumoperitoneum.
Her clinical status quickly improved, transitioning to tracheotomy collar on postoperative day (POD) 1. Chest tubes were removed on POD3 and POD5. She was discharged on POD11 with a speaking valve on her tracheotomy. Her tracheotomy tube was downsized 2 weeks post discharge, and she was decannulated 3 months later as her subglottis improved to a transverse lumen of 7 mm, sufficient for comfortable breathing. Her airway was stable for 15 months until dyspnea and stridor recurred with gradual restenosis. She underwent an awake tracheotomy, her postoperative course was uneventful, and she has been stable for 18 months.
Discussion
Jet ventilation is a technique in which a small catheter is placed through the glottis to deliver oxygen directly to the trachea. 4 Jet ventilation during endoscopic airway surgery decreases pressure on the vocal folds and provides surgical access to the larynx and subglottis.4-6 The major disadvantage of jet ventilation is the potential for barotrauma-related injuries and downstream complications, including subcutaneous emphysema, pneumomediastinum, pneumothorax, and more rarely, tension pneumothorax.7,8
Bourgain et al’s 9 multicenter study assessing complications of 643 transtracheal jet ventilation cases identified subcutaneous emphysema and pneumomediastinum as common barotrauma-related complications, while pneumothoraces were rare (7/643). 9 The rate of pneumothoraces during jet ventilation ranges from 0% to 0.4% in the literature.10-12 Pneumothoraces may be secondary to barotrauma for many reasons. 13 These include poor airway exchange, catheter placement causing inappropriate delivery of large gas volumes to distal airway segments, excessively high driving pressures causing hyperinflation, or obstruction of the air outflow tract resulting in “gas trapping” and parenchymal integrity loss due to breath-stacking or auto-positive end-expiratory pressure.13-15 Outflow tract obstruction likely caused the barotrauma in the patient described above.
Anesthesia guidelines recommend maximum driving pressures of jet ventilation at 50 psi. 16 Some literature suggest initial driving pressures of 20 to 25 psi in adults, adjusting pressures according to patient size, predicted lung compliance, and airway resistance.16,17 Better outcomes were achieved when driving pressures were increased gradually until adequate chest rise and fall were maintained (maximum 50 psi). 17
Cases with cascading and critical incidents requiring rapid recognition and action demonstrate the importance of communication and planning. This case reiterates that discussions between the anesthesia and otolaryngology teams about the nature and sequence of airway management during the recommended preoperative surgical safety checklist or “time out” are of utmost importance. 18
Jet ventilation is a well-studied, highly efficient method to maintain airway and allow surgical access during otolaryngology surgeries.5,9,10 Though rare, recognition and management of barotrauma-induced injuries during acute decompensation is crucial, as evidenced by this case in which restoring the ability to ventilate (via tracheotomy) and release of the tension pneumothorax (via chest tube insertion) was imperative.19-21
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The study participant provided informed consent prior to submission of this case.