
Abstract
Introduction
Endoscopic endonasal skull base surgery (EESBS) is widely used for accessing anterior skull base and sellar/parasellar lesions. 1 As the role of endoscopic surgery in skull base surgery increases, interest in postoperative olfactory function has also increased. Benign or malignant skull base tumor removal requires surgical corridor for endoscopy and instruments. Creating this passage damages normal structures around the olfactory cleft, causing olfaction issues. 2
Considering these problems, appropriate olfactory evaluation should be performed before and after surgery. Several olfactory function tests are available to evaluate the patients.
Psychophysical tests, including the University of Pennsylvania Smell Identification Test, 3 , Sniffin’ Sticks, 4 Toyoda and Takagi’s perfumist’s strip method 5 (T&T olfactometry), the butanol threshold test 6 (BTT), and the Cross-Cultural Smell Identification Test 7 (CCSIT), are widely used to evaluate olfactory function. However, studies have shown that the results of psychophysical tests differ from subjective reports of patients.8,9
The authors developed the olfactory questionnaire (OQ) for Koreans and demonstrated its effectiveness by comparing it with the CCSIT and BTT. 9 However, it has not been validated that OQ can quantitatively measure perioperative olfactory changes.
Therefore, in this study, we evaluated the usefulness of the OQ in Koreans for olfactory assessment in patients who underwent EESBS.
Methods
Participants
We retrospectively reviewed patients who underwent EESBS for skull base tumors in the sellar or parasellar areas between 2012 and 2018 at a single institution.
Based on the self-olfactory function assessment, only patients with preoperative normosmia (“I can always smell”) were analyzed. Other inclusion criteria were as follows: (1) full assessment of olfactory function composed of both OQ and psychophysical tests preoperatively and at least 6 months postoperatively, and (2) no previous history of other sinonasal surgery or disease, which may have an impact on patients’ olfactory function.
Patients who underwent revision surgery because of disease recurrence or cerebrospinal fluid (CSF) leak were excluded. Patients who underwent transcribriform approach for removal of skull base pathologies such as olfactory groove meningioma or olfactory neuroblastoma were also excluded.
Tumor characteristics, including surgical pathology and size, were reviewed. Preoperative sellar magnetic resonance imaging (MRI) was performed for all subjects using a 3 T MRI system with 1 mm thin slices. The tumor size was measured using contrast-enhanced T1-weighted coronal images. The maximum area of the dimensional phase was determined by measuring the lengths of the horizontal and vertical major axes. Other clinical parameters, such as age, sex, and nasoseptal flap utilization, were also reviewed.
Surgical Technique
The surgery begins with a gentle lateralization of all the turbinates. Generally, a hemitransfixation incision is made at the left nasal septum, followed by submucoperichondrial and submucoperiosteal dissection up to the anterior wall of the sphenoid sinus. After separating the bony cartilaginous junction, the bony septum is carefully removed. Subsequently, an incision is made at the right nostril using a monopolar cautery 6 inch needle tip (ConMed). This incision begins at the level of the sphenoid natural ostium and extends caudally to the lower level of the superior turbinate, presumably below the olfactory fibers. The incision is continued in the right nasal septal mucosa until the anterior end of the middle turbinate. Bilateral wide sphenoidotomies are then performed. In most cases, the sellar floor is laterally exposed to the bilateral medial wall of the cavernous sinus. Ethmoidectomy or middle turbinectomy was not a routine process; however, it was performed if a wider exposure was necessary. After tumor removal, in cases of high-flow CSF leakage, the septal mucosal incision initially made on the right nostril was extended anteriorly to create a nasoseptal flap. This was followed by multilayer reconstruction.
Patient Categorization Based on Subjective Olfactory Assessment
Patients were classified into 5 olfactory function categories based on the self-olfactory function assessment: (1) normosmia (“I can always smell”); (2) mild hyposmia (“I can often smell”); (3) moderate hyposmia (“I can sometimes smell”); (4) severe hyposmia (“I can seldomly smell”); and (5) anosmia (“I can never smell”). 9 After exclusively including patients who responded “I can always smell” before surgery, the same questions were repeated postoperatively to classify the patient population.
Olfactory Function Tests
Olfactory function was quantified using the BTT, 4 the CCSIT 7 (Sensonics), and the OQ at the same time period. In the BTT, 13 dilutions of n-butanol (Sigma-Aldrich) in odorless mineral oil were prepared. Each level was serially diluted 3-fold with 100% n-butanol to test both trigeminal and olfactory perception. The patients were given 2 bottles: 1 bottle contained mineral oil alone, and the other contained diluted butanol. The patients were asked to identify the bottle containing the butanol odor. According to the outcome, the threshold test proceeded to a higher concentration than the most diluted concentration (level 12). The olfactory threshold was determined based on the dilution level at which butanol was correctly identified in 5 consecutive trials.
The OQ was composed of 11 questions, with 1 question on odor occurring in daily life, 7 on specific odors familiar to Koreans, and 3 on trigeminal nerve-related odors (Figure 1). Each question consisted of a maximum of 4 points, with a total maximum score of 44 points. Originally, 14 questions were first developed; however, 11 questions with a κ value of 0.6 or higher were finally selected through a test-retest reliability analysis. The correlation between the questionnaire and BTT and CCSIT scores was proven in a large-scale study of 2273 subjects. 9
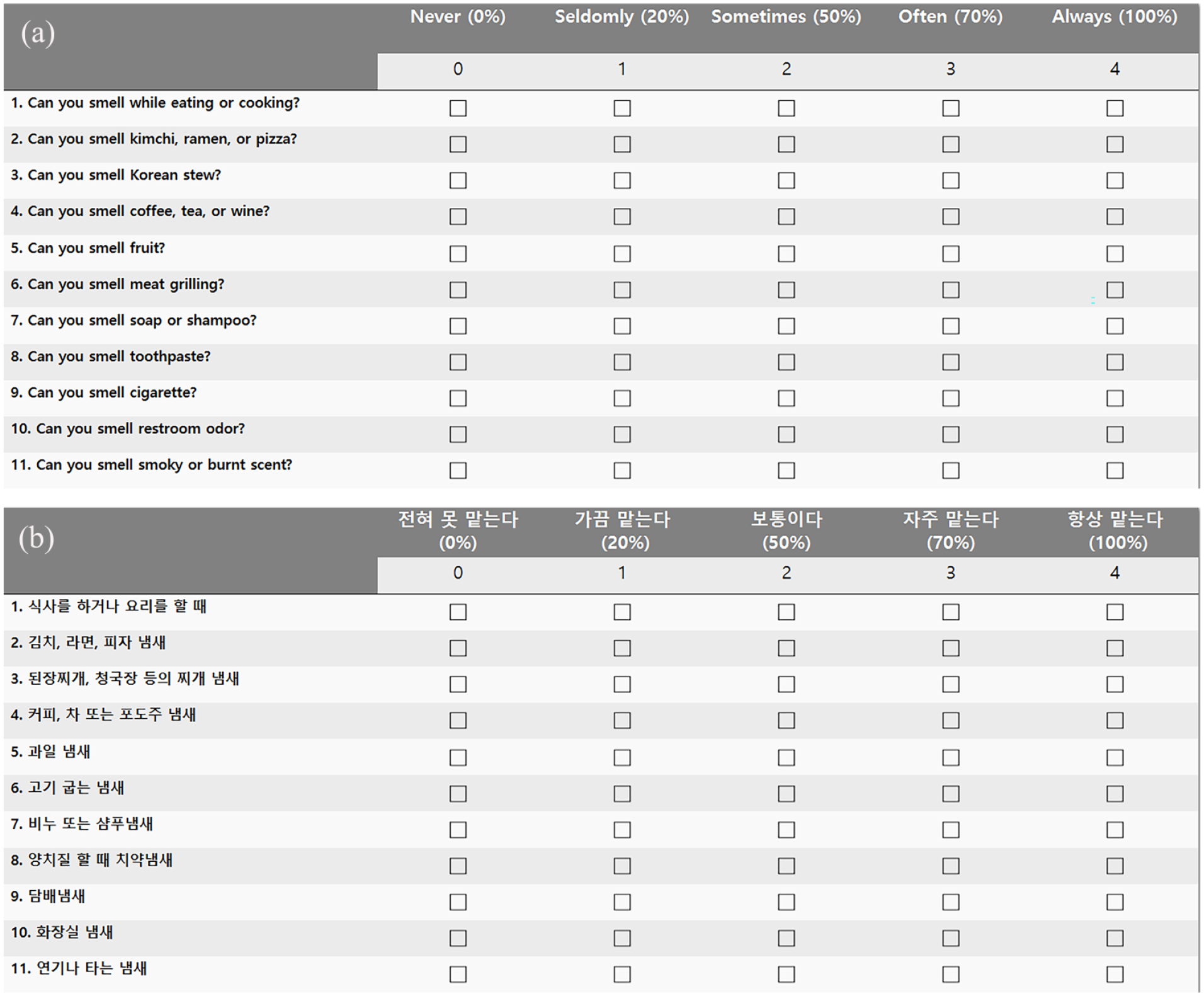
Olfactory questionnaire with 11 items. (a) English version, (b) Korean version.
Statistical Analysis
Data were analyzed using SPSS (version 19.0; IBM) and WEKA. 10
Continuous variables, such as olfactory function scores, are presented as mean ± standard deviation. Paired sample t tests were performed to compare olfactory function before and after surgery.
Pearson’s correlation analysis was performed to analyze the correlation between pre- and postoperative changes in olfactory function. Differences of olfactory function between multiple groups were analyzed using the Kruskal-Wallis test with Dunn’s multiple comparisons test after confirmation of a nonparametric distribution.
Using 3 distinct olfactory function tests (BTT, CCSIT, and OQ), we developed multiclass prediction models encompassing categories of normal, mild hyposmia, moderate hyposmia, severe hyposmia, and anosmia. In addition, binary models were constructed, distinguishing between normal olfaction and all other classes. These models were based on postoperative self-olfactory assessments acquired concurrently with the administration of other olfactory tests. Logistic regression with 10-fold cross-validation was employed for model development. Multicollinearity between olfactory function tests was checked and eliminated using tolerance test in SPSS. A multivariate linear regression analysis (using the enter method) was performed to identify factors affecting olfactory function test results. Statistical significance was set at P < .05.
Ethics Statement
This study was approved by the Institutional Review Board of the research institution concerned. Due to the characteristics of simple retrospective study, informed consents were waived on approval by the Institutional Review Board.
Results
Patient Characteristics and Perioperative Olfactory Function Test Results
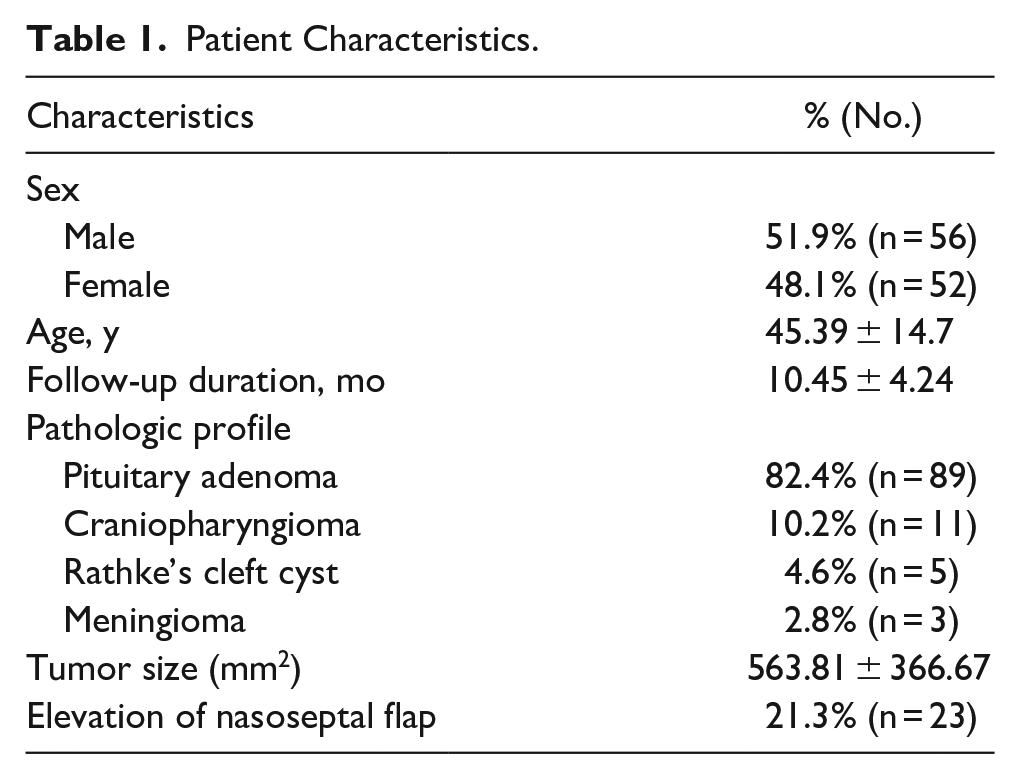
A total of 108 participants were included in the study. The mean age of the patients was 45.39 ± 14.7 years; of them, 56 (51.9%) were males. The average follow-up duration was 10.45 ± 4.24 months.
Pathological analysis revealed that pituitary adenoma accounted for the highest proportion (n = 89, 82.4%). Subsequently, benign tumors, such as craniopharyngioma (n = 11, 10.2%), Rathke’s cleft cyst (n = 5, 4.6%), and meningioma (n = 3, 2.8%), were observed.
The mean tumor size was 563.81 ± 366.67 mm2. For reconstruction, pedicled nasoseptal flaps were used in 23 (21.3%) patients. The patient characteristics are summarized in Table 1.
Patient Characteristics.
After surgery, classifications based on subjective olfactory assessment are as follows: 26 patients had normosmia, 17 had mild hyposmia, 20 had moderate hyposmia, 25 had severe hyposmia, and 20 had anosmia. There was a significant change in the olfaction scores. Postoperatively, the mean CCSIT, BTT, and OQ scores decreased from 9.05 ± 1.75 to 6.74 ± 3.1, 9.13 ± 1.55 to 7.63 ± 2.81, and 42.07 ± 4.68 to 20.97 ± 16.76, respectively (P < .001).
Significant correlations were noted between changes in pre- and postoperative olfactory function tests (Table 2). Changes in OQ scores were highly correlated with changes in the psychophysical olfactory tests (r = .685, P < .001 for BTT; r = .646, P < .001 for CCIST).
Correlations Between Changes in Olfactory Function Tests.
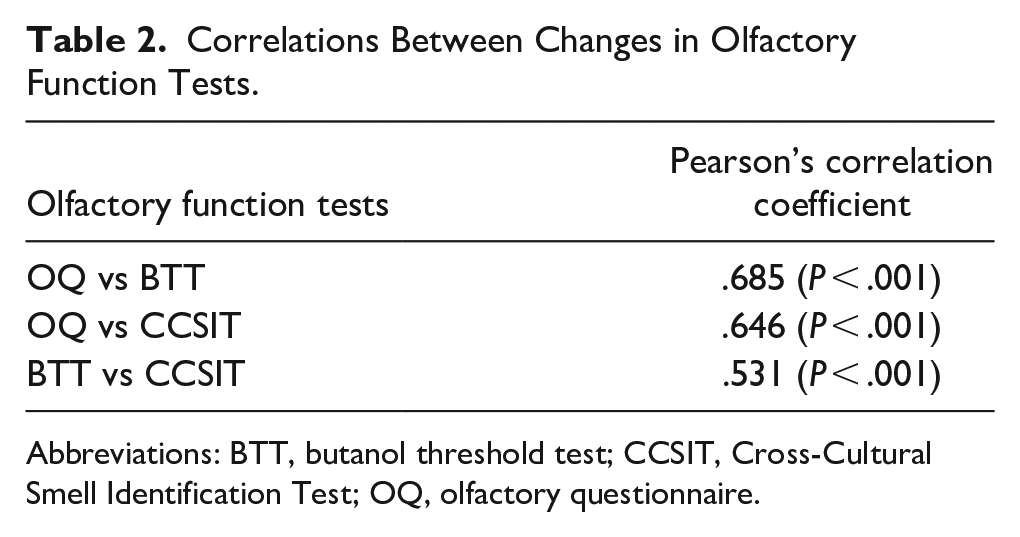
Abbreviations: BTT, butanol threshold test; CCSIT, Cross-Cultural Smell Identification Test; OQ, olfactory questionnaire.
There was a significant correlation between the changes in CCSIT and BTT scores; however, the correlation coefficient was rather low (r = .531, P < .001).
Diagnostic Ability of Olfactory Function Test for Postoperative Self-Olfactory Assessment
The OQ had the highest predictive power in the multiclass model, with an area under the curve (AUC) of 0.894, followed by BTT at 0.767. CCSIT had the lowest predictive power of 0.688.
For the binary prediction model, the same order was evident with AUCs as follows: 0.952, 0.853, and 0.768 for the OQ, BTT, and CCSIT, respectively. The confusion matrix for each class is shown in Figure 2.
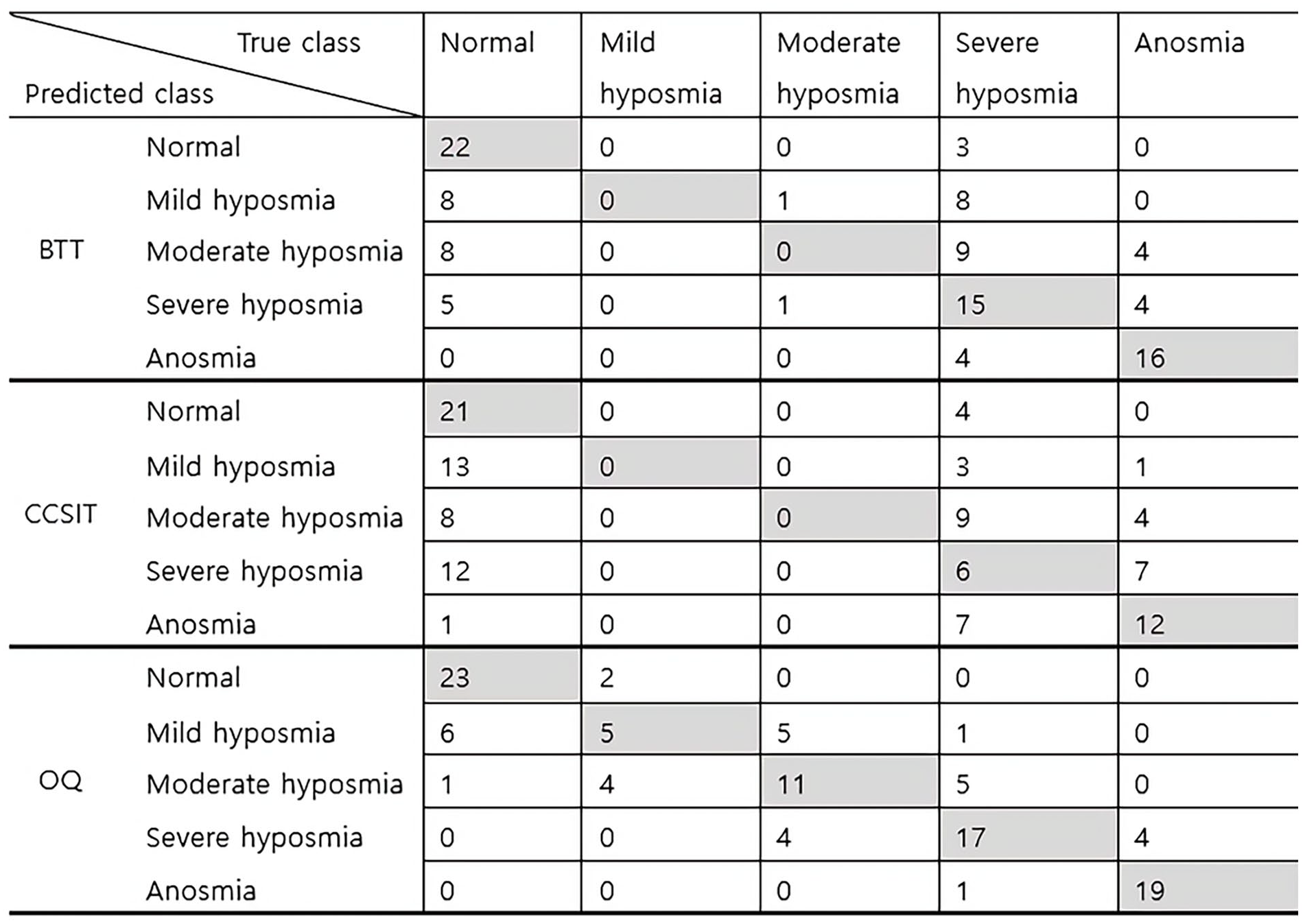
Confusion matrix of the prediction model based on BTT, CCSIT, and OQ for multiclass subjective olfactory function. BTT, butanol threshold test; CCSIT, Cross-Cultural Smell Identification Test; OQ, olfactory questionnaire.
The mean postoperative BTT, CCSIT, and OQ scores were compared among the groups of 5 categories based on subjective self-olfactory assessment (Figure 3). Although there was a significant difference in BTT (P < .001), CCSIT (P < .001), and OQ (P < .001) scores among the groups, post hoc analysis of subgroups revealed that only the OQ scores were significantly different between mild and severe hyposmia (P < .001), suggesting that the OQ may be the best assessment tool for evaluating patients with hyposmia. Detailed P values for the differences between self-olfactory assessment groups are summarized in Supplementary Table 1.
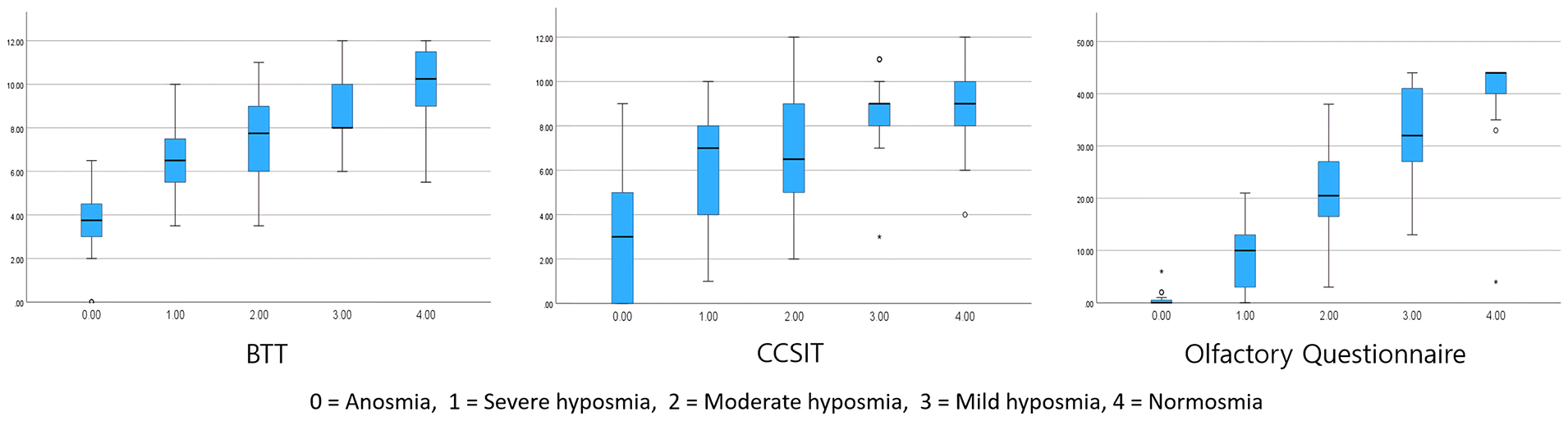
Postoperative scores of BTT, CCSIT, and OQ based on 5 self-assessment categories. BTT, butanol threshold test; CCSIT, Cross-Cultural Smell Identification Test; OQ, olfactory questionnaire.
Factors Related to Olfactory Outcome After EESBS
As the OQ had the highest predictive power for patient classification, a multivariate linear regression was performed to identify factors affecting olfactory outcome based on the OQ score (Table 3).
Multivariate Linear Regression Analysis of Clinical Factors Associated With Postoperative Questionnaire Score.
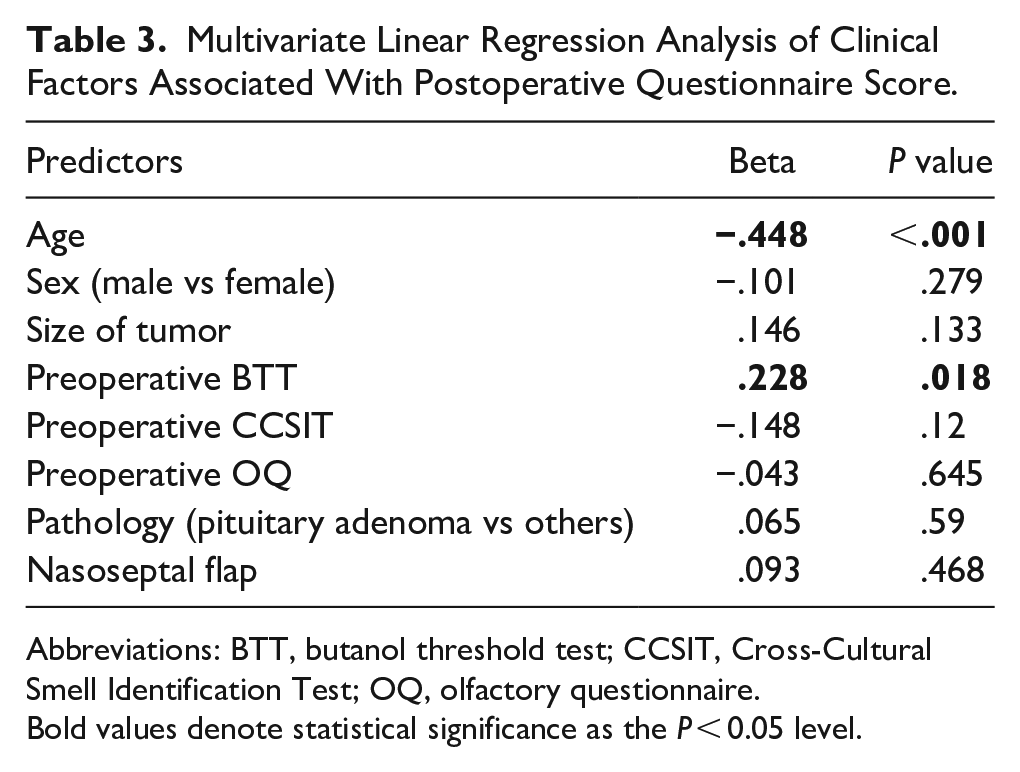
Abbreviations: BTT, butanol threshold test; CCSIT, Cross-Cultural Smell Identification Test; OQ, olfactory questionnaire.
Bold values denote statistical significance as the P < 0.05 level.
Among the clinical variables, the patient’s age at the time of surgery and preoperative BTT score were significantly related to postoperative olfactory outcome. Based on this result, it can be suggested that the younger the age, the higher the preoperative BTT score and the better the olfactory prognosis.
Discussion
In this study, the OQ showed the highest predictive ability for changes in subjective olfactory function after EESBS. Based on the multiclass prediction model, the prediction performance of hyposmia severity (mild/moderate/severe) was rather low for BTT and CCSIT, suggesting a limitation of conventional psychophysical tests in evaluation of postoperative hyposmia patients (partial loss of olfactory function).
As psychophysical tests utilize suprathreshold stimulation, there is a risk of false-negative results for olfactory loss. This may result in underestimating the degree of hyposmia, and discrimination against the severity of olfactory stimulation in real-life scenarios may be limited.
In addition, culture can affect smell identification familiarity, potentially reducing predictive accuracy. It is known that the percentages of correct answers to olfactory stimuli such as turpentine, thinner, and lemons, which are somewhat unfamiliar to Koreans, are lower than those of other stimuli among people with normosmia. 11 In addition, olfactory changes based on psychophysical testing do not measure changes that can actually affect olfactory-related quality of life. On the other hand, the OQ is derived from questions that Koreans are more likely to encounter subjectively in their daily lives. This characteristic appears to contribute to a higher AUC value in OQ for predicting postoperative self-olfactory assessment.
Similarities can be reflected in the questionnaire and patient classification based on subjective olfactory function assessment (normosmia; mild, moderate, or severe hyposmia; and anosmia) or assessment of patients using a visual analog scale (VAS). However, we consider it important to quantitatively measure with multiple questionnaires since patients’ intuitions may fluctuate. Based on a similar study of 285 patients with subjective olfactory dysfunction, it was confirmed that the questionnaire’s ability to predict and discriminate quantified olfactory function was superior to that of a simple VAS evaluation. 12
Mattos et al validated questionnaires, such as Questionnaire of Olfactory Disorders-Negative Statements (QOD-NS) and investigated changes in quality of life related to olfaction before and after endoscopic sinus surgery for patients with chronic rhinosinusitis. 13
QOD-NS comprises 4 distinct domains; eating-related questions, social-related questions such as impairment of interpersonal relationship, questions related to mental stress, and questions regarding how bothersome the changes can be to the patients. They found that eating-related domains had the greatest improvement after endoscopic sinus surgery.
The OQ used in the current study also contains different subdomains: questions on (1) odors occurring in daily life, (2) specific odors familiar to Koreans, (3) trigeminal nerve-related odors, and (4) olfactory status evaluated by people around the subject. Our study did not further evaluate changes in each subdomain; therefore, it would be interesting to determine which specific domain is mostly affected and to understand how other domains, besides eating, change after EESBS.
There are diverse locoregional questionnaires, and studies about their performance are being conducted, even until recently. As an illustration, the Italian version on short form of the Questionnaire of Olfactory Disorders-Negative Statements has exhibited high internal consistency and test-retest reliability, establishing notable correlations with widely utilized clinical questionnaires. 14 A study conducted in France, which compared individuals with olfactory disorders to a control group, revealed significant correlation between the French version of the Olfactory Disorders Questionnaire and both the Sinonasal Outcome Test 22 (SNOT-22) and TDI scores (the sum of olfactory threshold score, odor discrimination score, and odor identification score). 15
In these comparable studies, regional questionnaires feature items related to quality of life. In contrast, our questionnaire quantifies the degree of olfaction specifically in the scents that Koreans commonly encounter in their daily lives. In addition, the strength of this study lies in thorough pre- and postsurgery olfactory assessment using psychophysical tests and questionnaires, and the homogeneity of patients with similar etiology of olfactory loss as it is known that patterns of olfactory impairment may depend on the etiology of olfactory loss. 16
In addition, EESBS may pose a higher risk of postoperative olfactory changes compared to conventional nasal or sinus surgery, which makes it a good patient pool for comparative analysis of olfactory function testing.17,18
Studies on the discrepancy between subjective and psychophysical olfactory assessment in various conditions have been continuously reported. This dissociation can be influenced by other factors, including demographic factors such as age, ethnicity, or comorbidities. Based on the differences in subjective and psychophysical testing, old age and Black ethnicity correlated with underreporting olfactory impairment, while persistent cold symptoms or a history of COVID-19 were associated with overreporting.19-21 Therefore, when interpreting subjective olfactory assessment, the possibility of under- or overreporting olfactory impairment should be considered. In addition, the timing of assessment is recognized as a factor influencing the dissociation between subjective and psychophysical olfactory assessments, especially following nasal surgery. 22 It is known that in the short term, the correlation between subjective and psychophysical olfactory assessments is less significant compared to the long term. This observation may be attributed to the presence of confounding factors, including difficulties in nasal breathing.
This study confirmed that older patients had poor olfactory outcomes after surgery. Many studies have reported that olfactory function decreases with age.23,24 When the olfactory epithelium is damaged, stem cells are activated to replace damaged cells that contain olfactory sensory neurons.25-27
As age increases, decreased regeneration of olfactory receptor neurons results in a decrease in the total number of olfactory receptor neurons.28,29 It has been reported that aging and recovery of olfactory function are negatively correlated in cases of olfactory damage after upper respiratory tract infection. 30 Similarly, in mouse model experiments, it was confirmed that the proliferative activity of olfactory neuroepithelium decreased with older age after damage to the olfactory mucosa, resulting in incomplete reconstitution of the olfactory neuroepithelium. 31 In contrast, a higher preoperative BTT was associated with better olfactory outcomes. A higher preoperative BTT score may also indicate a larger abundance of high olfactory reserve, suggesting a better recovery. Similarly, it was reported that the higher the Sniffin’ Sticks score before endoscopic sinus surgery, the higher the postoperative olfactory preservation rate. 32 These physiological mechanisms explain why the nasal mucosa and olfactory epithelium of older adults or patients initially presenting with lower BTT become more vulnerable to damage and that the chance of recovery also decreases.
In this study, unlike others, 33 factors like nasoseptal flap, tumor size, or disease pathology were not linked to postoperative olfactory outcomes. This discrepancy might be due to a higher olfactory loss rate in this study. Olfactory function issues after EESBS are reported at 20%, 34 but over 50% of subjects here had decreased sensation after 6 months. Excessive manipulation of the olfactory strip in past surgeries might be a cause. Now, surgery aims to preserve the olfactory strip.
The OQ is a simple alternative for olfactory assessment, but we recommend combining it with psychophysical tests for preoperative evaluation, as preoperative BTT is a prognostic factor for olfactory recovery after EESBS. For simplicity and reliability, the OQ may be the first choice for olfactory evaluation during the postoperative period followed by psychophysical tests whenever necessary.
Moreover, OQ’s ability to differentiate normosmia from hyposmia makes it valuable for future research on factors associated with olfactory outcomes after EESBS.
This study had several limitations. First, we used a self-rating scale as a criterion for patient selection and evaluation of olfactory function tests. Unlike our study, studies that validated olfactory function tests tended to use other classifications of olfactory status based on psychophysical tests.4,35 However, this may vary among cultures or countries. 36 There are several studies from Korea that described diagnostic cutoff values of various psychophysical tests for normosmia, hyposmia, and anosmia.37,38 However, these too were based on patient-reported outcomes. Second, the number of subjects is limited, and it has simple retrospective study design. Third, the questionnaire items were specifically designed to align with the lifestyle of Korean people, which may limit their global applicability. In addition, due to the study’s design constraints, we did not address or validate the potential influence of ethnicity or socioeconomic status on subjective olfaction.
Therefore, a large-scale study considering various demographic factors will be needed for better demonstration in the future.
The convenience of OQ can facilitate large-scale follow-up studies through multicenter survey. The OQ, based on feasibility in reflecting subjective olfactory function, is considered to be widely applicable for researches on factors influencing olfactory function and for perioperative follow-up for olfaction.
Conclusion
In this article, we confirmed the predictive ability of the OQ in evaluating the self-assessed olfactory function in daily life after EESBS. Although the OQ score best predicted the current self-assessed olfactory function compared to other psychophysical tests, patient age and baseline BTT were associated with postoperative olfactory outcomes. Therefore, comprehensive evaluation of patient demographics and psychophysical olfactory tests along with a questionnaire is important for assessing and predicting olfactory outcomes.
Supplemental Material
sj-rtf-1-ear-10.1177_01455613241234818 – Supplemental material for Validation of Korean Olfactory Questionnaire for Perioperative Olfactory Assessment in Endoscopic Endonasal Skull Base Surgery
Supplemental material, sj-rtf-1-ear-10.1177_01455613241234818 for Validation of Korean Olfactory Questionnaire for Perioperative Olfactory Assessment in Endoscopic Endonasal Skull Base Surgery by Young-Chang Sim, Seung Koo Yang, Sun A. Han, Young-Hoon Kim, Kihwan Hwang, Jin-Deok Joo, Sung-Woo Cho, Tae-Bin Won, Chae-Seo Rhee, Chae-Yong Kim and Jeong-Whun Kim in Ear, Nose & Throat Journal
Footnotes
Data Availability
The data that support the findings of this study are available from the corresponding author, Sung-Woo Cho, on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. NRF-2022R1C1C1011966).
Ethics Approval
This study was approved by the Institutional Review Board (IRB) of the Seoul National University Bundang Hospital (IRB No. B-2208-775-101). Due to the characteristics of simple retrospective study, informed consents were waived on approval by the IRB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.