
Abstract
Significant Statement
Presentation of laryngeal squamous cell carcinoma as a glottic web is rare. Maintaining a high level of suspicion of malignancy is critical to ensure proper management, avoid delayed care, and prevent neoplastic progression. We present a case of a dysphonic patient who was found to have an anterior glottic web, which was later discovered during web excision to contain squamous cell carcinoma.
Laryngoscopic Clinic
A 65-year-old female with a past medical history significant for alcoholism, former tobacco use, asthma, and a family history of esophageal cancer presented to our office for evaluation of dysphonia. She described her voice as severely weak, strained, and raspy. Voice change had started 3 years prior to our initial consultation and had worsened progressively over weeks to months. The patient had been evaluated by numerous otolaryngologists within the 10 months prior to our visit and had been diagnosed with laryngopharyngeal reflux, glottic web, and spasmodic dysphonia. She had had multiple routine intubations during the 3 years before our initial visit, including intubation for functional endoscopic sinus surgery with polypectomy 10 months prior to her first visit with us.
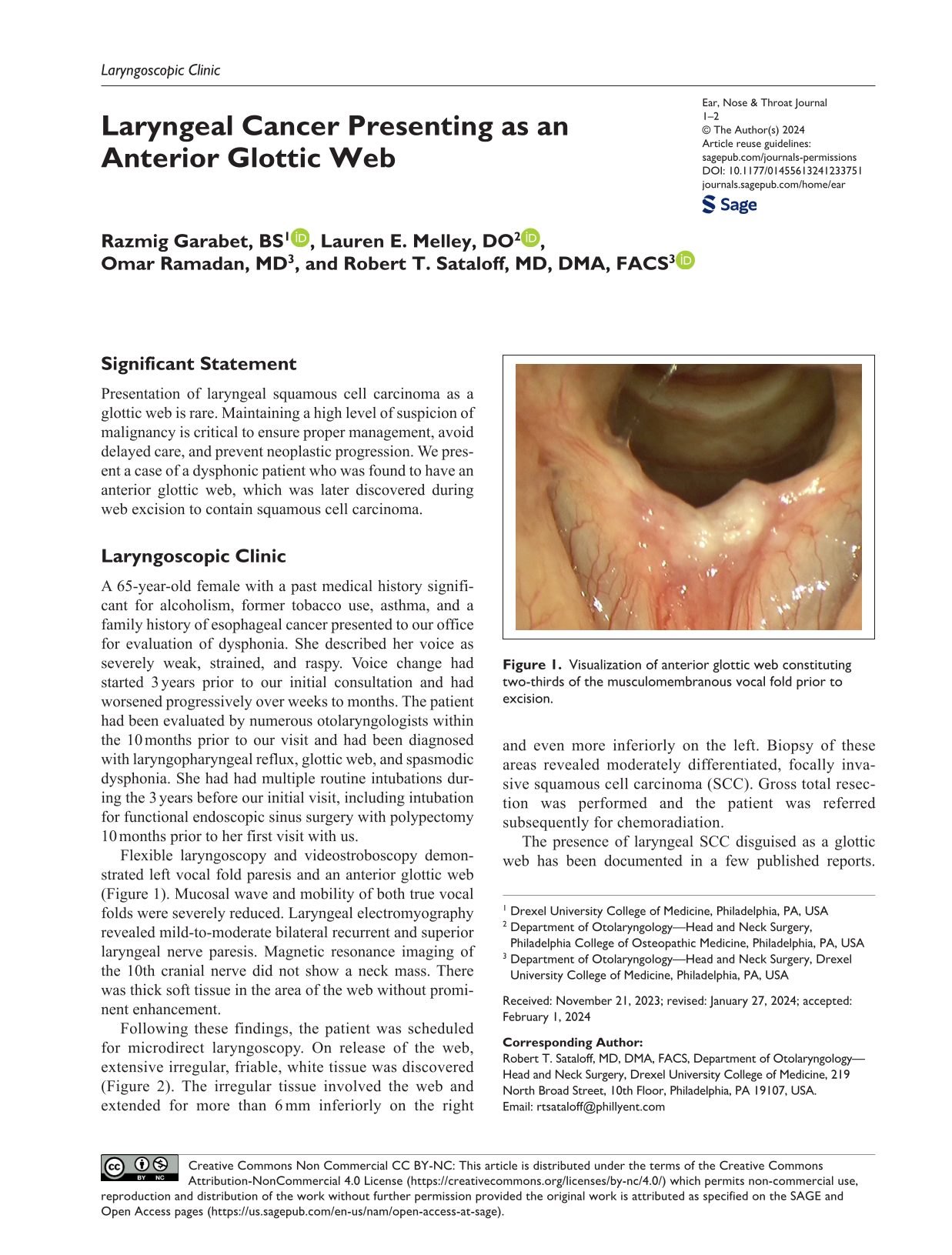
Flexible laryngoscopy and videostroboscopy demonstrated left vocal fold paresis and an anterior glottic web (Figure 1). Mucosal wave and mobility of both true vocal folds were severely reduced. Laryngeal electromyography revealed mild-to-moderate bilateral recurrent and superior laryngeal nerve paresis. Magnetic resonance imaging of the 10th cranial nerve did not show a neck mass. There was thick soft tissue in the area of the web without prominent enhancement.
Visualization of anterior glottic web constituting two-thirds of the musculomembranous vocal fold prior to excision.
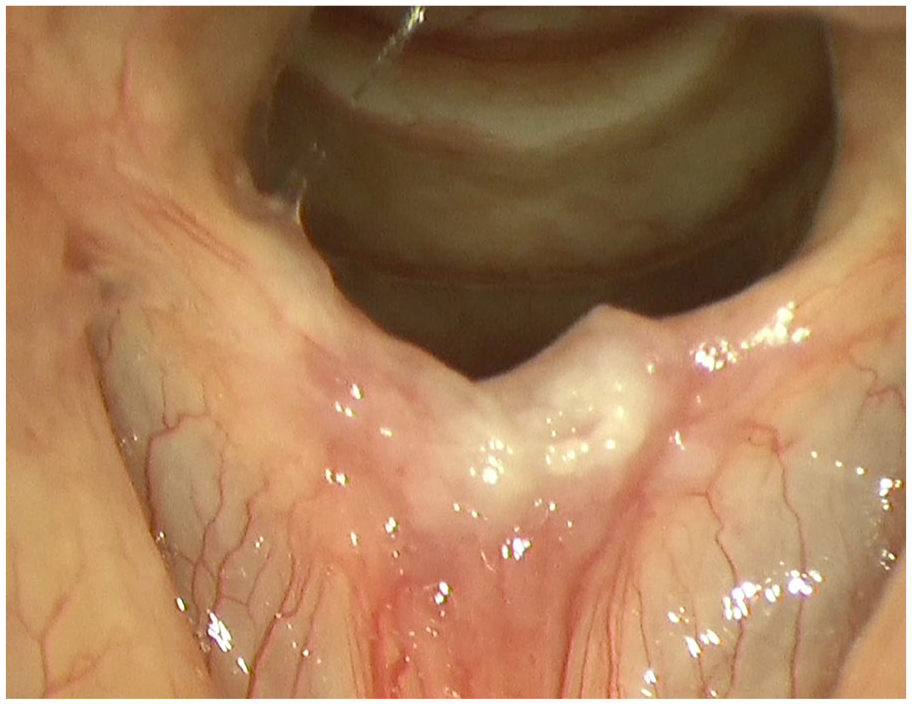
Following these findings, the patient was scheduled for microdirect laryngoscopy. On release of the web, extensive irregular, friable, white tissue was discovered (Figure 2). The irregular tissue involved the web and extended for more than 6 mm inferiorly on the right and even more inferiorly on the left. Biopsy of these areas revealed moderately differentiated, focally invasive squamous cell carcinoma (SCC). Gross total resection was performed and the patient was referred subsequently for chemoradiation.
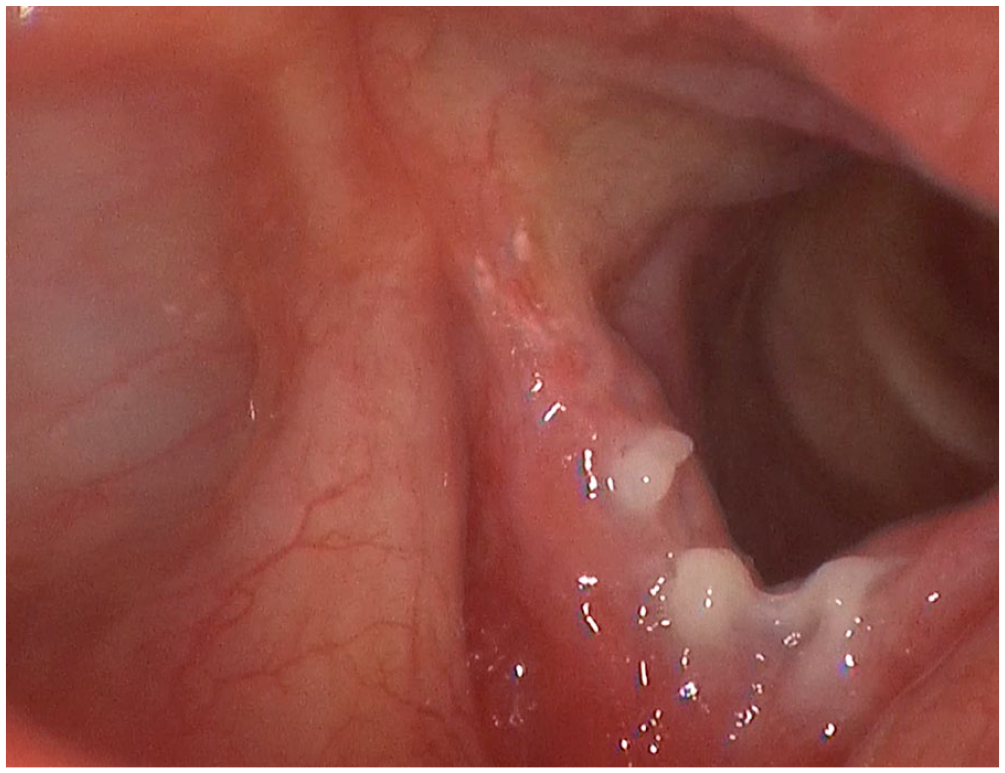
Visualization of vocal fold SCC following surgical release of glottic web. SCC, squamous cell carcinoma.
The presence of laryngeal SCC disguised as a glottic web has been documented in a few published reports. Ramaswamy et al 1 presented a case series of 6 patients who were found to have laryngeal SCC after initial diagnosis of an idiopathic anterior glottic web, of which 3 were former smokers, 3 had a history of intubation, 1 had a history of laryngeal surgery, and 5 had achieved complete remission. In another case report, the patient demonstrated milky-appearing tumorous lesions on both vocal folds adjacent to a glottic web, and both the masses and the tissue of the web were identified to be laryngeal SCC. 2 Charaklias et al 3 described a patient with a glottic web that had recurred 7 times. Initial biopsies consisted of noncancerous tissue. However, the eighth specimen revealed laryngeal SCC, which was managed subsequently by total laryngectomy. 3 Thus, possible laryngeal SCC should be considered in patients presenting with a glottic web.
The suspicion for laryngeal SCC in a patient with a glottic web should be higher when established risk factors are present. These risk factors include tobacco smoking, alcohol consumption, exposure to occupational carcinogens, vitamin deficiency, radiation exposure, Epstein-Barr virus and human papillomavirus infections, and laryngopharyngeal reflux. 4 Presenting symptoms of benign glottic webs and laryngeal SCC may be similar. Symptoms and signs that may increase the likelihood of laryngeal SCC include dysphagia, odynophagia, otalgia, cervical adenopathy, and weight loss, although our patient had none of these. 5 Therefore, a comprehensive understanding of patient history is critical to guide the diagnostic process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.