
Abstract

Significant Statement
Subcutaneous emphysema resulting from facial trauma is not rare, but its exacerbation due to nose blowing is less frequent. To minimize the risk of exacerbating subcutaneous emphysema, avoiding forceful nose blowing or holding in sneezes is suggested. On the contrary, when encountering subcutaneous emphysema in the head and neck region, it is important to consider the potential for injury to the respiratory tract that could lead to such a sudden condition.
Head and Neck Clinic
An 18-year-old young man, who had been punched by someone, arrived at our emergency displaying diffuse swelling on his left face. Initially, he had not observed any immediate swelling; he only experienced pain and bruising on his left cheek. However, when he attempted to clear nasal passages by blowing his nose, his left face began to swell suddenly (Figure 1). On physical examination, we observed significant swelling in left inferior periorbital area. Notably, when palpating his face, a distinct crepitus sound was discernible. Further nasopharyngoscopy revealed no active bleeding or structural abnormalities except the presence of blood clots in left nostril and nasopharynx. Computed tomography scan of the orbit revealed the presence of multiple pockets of trapped air beneath the skin situated along various regions, including left periorbital area, parapharyngeal space, masticator space, and upper neck (Figure 2A and B). Notably, we identified fractures in anterior wall of left maxillary sinus with fluid accumulation within the sinus (Figure 2C). The condition of clinical subcutaneous emphysema resolved on its own over the course of 2 days. One week later, the patient underwent surgery to realign displaced bones with uneventful recovery.
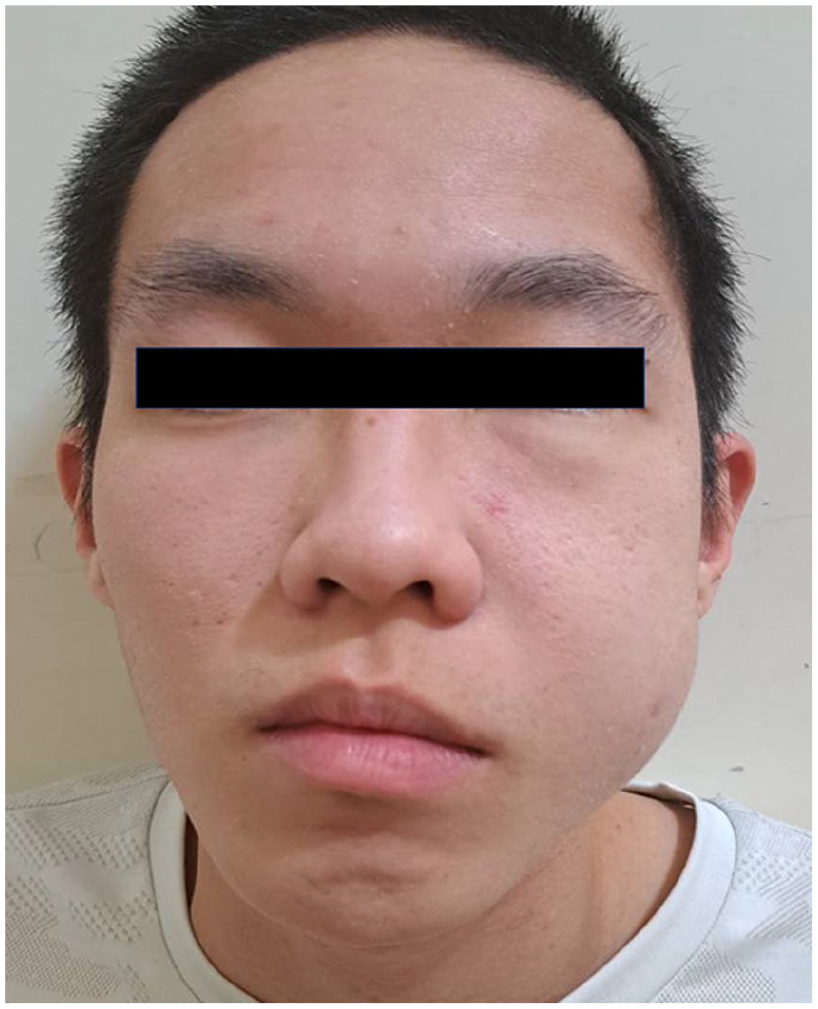
Photograph of the patient in emergent department revealing the left facial swelling.

(A and B) Computed tomography of the orbit showed subcutaneous emphysemas (stars), distributed at left periorbital area, parapharyngeal space, masticator space, and upper neck. (C) Displaced fracture (arrow) of anterior wall of left maxillary sinus seen with fluid accumulation within the sinus.
Subcutaneous emphysema, characterized by the trapping of air beneath the skin, is typically a benign and self-limited condition resulting from an underlying problem. The most common cause of facial subcutaneous emphysema is iatrogenic, often associated with dental procedures, while blunt traumatic injuries are less frequent.1,2 It typically occurs secondary to a facial trauma with fractures of the paranasal sinuses and sometimes involves regions adjacent to the injury including the periorbital (the most common) and cervical areas. 3 According to a previous literature review, subcutaneous emphysema will typically require conservative management and resolve spontaneously within a few days. 3 However, potential severe complications of cervicofacial emphysema including orbital compartment syndrome, airway obstruction, pneumothorax, pneumomediastinum, air emboli, and cranial nerve palsy should necessitate emergent intervention. 3
In our presented case, the patient developed subcutaneous emphysema as a result of being struck by an external force. The injury caused a displaced anterior maxillary sinus wall fracture, leading to the development of subcutaneous emphysema. The dynamics for this condition are that elevated nasal airflow pressure by nose blowing forced air to escape from the crack in the sinus wall into the surrounding tissues, exacerbating his facial swelling. To minimize the risk of exacerbating subcutaneous emphysema, avoiding forceful nose blowing or holding in sneezes is suggested. On the contrary, when encountering subcutaneous emphysema in the head and neck region, it is important to consider the potential for injury to the respiratory tract that could lead to such a sudden condition.
Footnotes
Author Contributions
Ting-Li Hung: first author and preparation of draft. Hsin-Chien Chen: corresponding author and editing of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-113006 to Hsin-Chien Chen).
Informed Consent
The patient consent statement was informed and approved by Tri-Service General Hospital Institutional Review Board.