
Abstract
Background
Benign paroxysmal positional vertigo (BPPV) is one of the most common vestibular vertigo disorders in clinical practice. It is suggested to be caused by otoconia that are dislodged from the otolith macula beds and are trapped in a semicircular canal, 1 often leading to balance problems and increased risk of falls. It is characterized by brief episodes of vertigo (generally less than 1 minute), often induced by changes in head position such as turning over in bed, bending forward, or tilting the head back. 2 According to the semicircular canal involved, BPPV can be divided into canalolithiasis of posterior canal (pc-BPPV), canalolithiasis of the horizontal canal (hc-BPPV), cupulolithiasis of the horizontal canal (hc-BPPV-cu), canalolithiasis of the anteriorcanal (ac-BPPV), and lithiasis of multiple canals (mc-BPPV). Canal repositioning is used for the restorative treatment of most BPPV patients. 3 However, refractory BPPV is mostly caused by repeated ineffective canalith repositioning procedure and persistent positional vertigo symptoms.
At present, there is no global unified diagnostic standard for refractory BPPV.4-6 The present study defined BPPV with recurrent vertigo and nystagmus lasting for 3 months or more and no curative effect after more than 2 reduction treatments as refractory BPPV.
One study found that the automatic vestibular function therapy system (SRM-IV) vestibular function diagnosis and treatment system has realized the full automation and standardization of the conventional manual induction reset procedure in terms of positioning, quantification, and constant speed, and 66 of 67 patients had complete resolution of positional vertigo and no positional nystagmus within 3 to 14 days. 7
The objective of this study was to observe the SRM system in the treatment of refractory BPPV, analyze its clinical characteristics, and evaluate its clinical efficacy. We analyzed the included cases in an attempt to provide a basis for clinical diagnosis and treatment.
Data and Methods
General Data
The clinical data of 39 patients with refractory BPPV who were admitted to the vertigo examination room of our hospital’s department of neurology from January 2020 to May 2022 were analyzed retrospectively. The diagnostic criteria were developed based on the 2007 diagnostic criteria of the Chinese Academy of Otolaryngology 4 and met the criteria for refractory BPPV. A total of 39 cases were enrolled, including 20 males and 19 females, aged 35 to 70 years, with an average age of 48 ± 11 years. There were 10 cases of pc-BPPV, 13 cases of hc-BPPV, 12 cases of hc-BPPV-cu, and 4 cases of mc-BPPV. The interval from onset to the first visit of doctor was <1 week in 10 cases, between 1 week and 1 month in 8 cases, and longer than 1 month in 21 cases. There were 8 cases with a first onset, 12 cases with a second onset, 15 cases with a third onset, and the remaining 4 cases had more than 5 onsets.
Case Screening Criteria
The inclusion criteria were as follows: (1) According to the BPPV treatment standard formulated at the Guiyang Conference in 2006, 5 all cases had the typical clinical symptoms of paroxysmal vertigo accompanied by nystagmus on postural changes, such as raising/lowering the head, touching a pillow, or lying down and turning over. (2) Refractory BPPV with recurrent vertigo and nystagmus lasting for more than 3 months and ineffective after more than 2 reduction treatments. (3)The result of a Dix-Hallpike test or a roll test was positive. 6 (4) After undergoing head computed tomography scan or magnetic resonance imaging, no obvious abnormality was found. (5) Central nervous system diseases, tympanitis, Ménière’s disease, and vestibular migraine were excluded. The horizontal semicircular canal refers to recurrent positional dizziness or positional dizziness, induced by lying down or flipping over on the back; the roll test induces brief positional nystagmus, which can have a latent period or no latent period; when the head turns to either side, it induces nystagmus horizontally facing the lower ear lasting less than 1 minute. The horizontal semicircular canal cap stones refer to positional vertigo that occurs repeatedly when lying down or flipping over in bed. The roll test induces positional nystagmus, and when the head is turned to both sides, it induces horizontal nystagmus facing the upper ear. This nystagmus can have no latent period or a brief latent period lasting more than 1 minute.
The exclusion criteria were as follows: (1) Patients with severe heart disease, tumor, severe cervical and lumbar lesions, or with a new fracture history and a surgical history within the previous 3 months. (2) Patients with mental diseases. In this study, all the enrolled cases were treated with the canalith repositioning procedure method more than twice before they were cured or eventually deemed incurable by the canalith repositioning procedure method.
Reduction Method
All patients underwent reduction using the SRM BPPV reduction system. Patients with pc-BPPV were treated with the Epley method, patients with hc-BPPV were treated with the barbeque method, and patients with hc-BPPV-cu were treated with the Gufoni method.
SRM Operation Process
First, the displacement test including Dix-Hallpike and/or Roll Test was performed, and the corresponding reduction treatment was given after the positioning was clear. Taking the right posterior semicircular canal as an example, the patient was first allowed to lie on the right side, the head was in a backward extension position for 1 minute, and then lay on the left side, the head was in a backward extension position. After 1 minute, the patient continued to rotate the body to the left side, in a lateral position, equivalent to 270° of rotation, and sat up after 1 minute.
The horizontal semicircular canal also has a corresponding reset method. The position angle and other parameter instruments have been built in. During the operation, the operator can complete the operation according to the prompt on the operating table. The reset chair can complete each precise action according to the operation steps to achieve the reset effect. For the operation process, the patient cannot tolerate or vomiting and other phenomena, can stop.
We evaluated once a week during the experiment. By asking whether the patient’s vertigo symptoms improved, the displacement test observed whether the nystagmus disappeared.
Evaluation of Curative Effects
The evaluation criteria of the curative effects were as follows 4 : (1) cured: positional vertigo disappeared, and the Dix-Hallpike test and/or roll test were negative. (2) Improved: positional vertigo and/or positional nystagmus were alleviated but not completely, or there was induced nystagmus in the Dix-Hallpike test and/or roll test. (3) Ineffective: positional vertigo and/or positional nystagmus were not alleviated and may have even been exacerbated.
Results
Among the 39 patients with refractory BPPV, 18, 14, and 5 patients were cured after 3, 4, and 5 SRM-IV canalith repositioning procedure, respectively. Two other patients were unable to recover through canalith repositioning procedure but improved after alternating between manual repositioning and Brandt-Daroff habituation training. 7 There were 10 cases of pc-BPPV, 13 cases of hc-BPPV, 12 cases of hc-BPPV-cu, and 4 cases of mc-BPPV. There were 19 patients with anxiety and insomnia, 7 of whom were treated with psychological counseling, 5 were treated with sedation to improve sleep, and 7 were treated with antianxiety therapy (Table 1).
Analysis of Results of 39 Cases of Refractory BPPV.
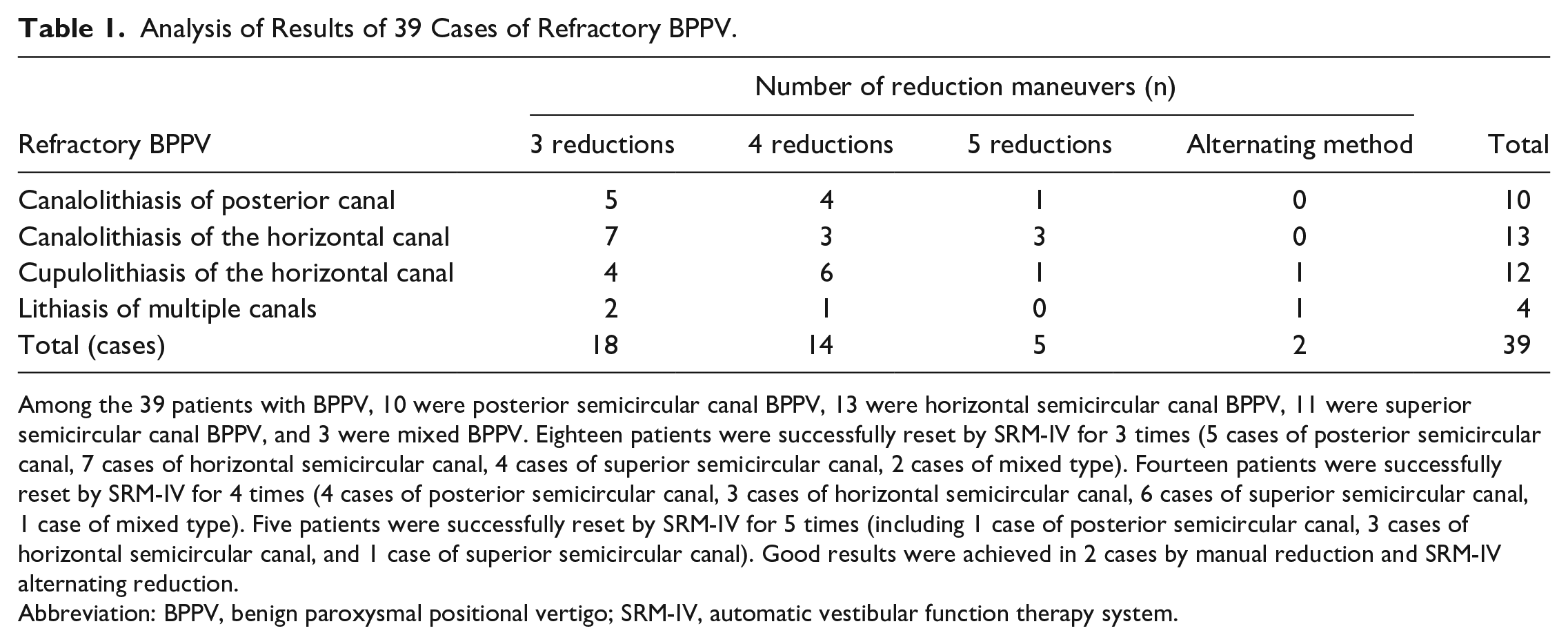
Among the 39 patients with BPPV, 10 were posterior semicircular canal BPPV, 13 were horizontal semicircular canal BPPV, 11 were superior semicircular canal BPPV, and 3 were mixed BPPV. Eighteen patients were successfully reset by SRM-IV for 3 times (5 cases of posterior semicircular canal, 7 cases of horizontal semicircular canal, 4 cases of superior semicircular canal, 2 cases of mixed type). Fourteen patients were successfully reset by SRM-IV for 4 times (4 cases of posterior semicircular canal, 3 cases of horizontal semicircular canal, 6 cases of superior semicircular canal, 1 case of mixed type). Five patients were successfully reset by SRM-IV for 5 times (including 1 case of posterior semicircular canal, 3 cases of horizontal semicircular canal, and 1 case of superior semicircular canal). Good results were achieved in 2 cases by manual reduction and SRM-IV alternating reduction.
Abbreviation: BPPV, benign paroxysmal positional vertigo; SRM-IV, automatic vestibular function therapy system.
Discussion
In this study, all the enrolled patients were treated with the canalith repositioning procedure method more than twice before they were deemed cured or eventually incurable by the canalith repositioning procedure. Analyzing the reasons for its refractory, in addition to being related to the blood supply disorder of the inner ear, 8 it may be multifaceted, as follows: first, due to the congenital abnormality of the anatomical structure of the semicircular canal on the affected side, the particles or fragments cannot be completely discharged in the expected direction during postural change. 9 Second, in the process of migration to the vestibulum, some particles or fragments adhere to the membranous semicircular canal, especially at the common foot, causing the stenosis of the membranous semicircular canal and further hindering the discharge of the remaining particles or fragments. Third, in the process of canalith repositioning procedure, the flow rate of particles is slow, the mobility is poor, and the waiting time after the change of body position is long; however, some otolith particles cannot be restored to the utricle. Fourth, the incorrect positioning of the affected side often occurs during the diagnosis of BPPV. In the horizontal semicircular canal, vertigo and horizontal nystagmus can be induced on both sides during the roll test; the symptoms and signs on both sides are the same, and the patient feels no difference; therefore, nystagmus is not obvious during the lying-down test, often leading to inconsistencies in measurement and analysis. 10 Finally, anxiety and depression are important causes of refractory BPPV.
Fifteen of the patients enrolled in this study had nystagmus lasting more than 1 minute. During treatment, the duration of each new position after each postural change was extended appropriately (2-4 minutes) to achieve recovery. Among the enrolled patients, 2 could not be cured by canalith repositioning procedure; in these 2 cases, the interval from onset to the first visit of doctor was more than 6 months, and one of the patients had as many as 15 attacks. The 2 patients were treated alternately with instrument reduction and manual repositioning, followed by Brandt-Daroff habituation training to improve symptoms after returning home. It can be seen from these results that the longer the interval from the onset of BPPV to the first visit of doctor, the worse the treatment effect, and the higher the onset frequency. In addition, in the process of canalith repositioning procedure for the aforementioned 2 cases, the duration of each position was extended after each head position change.
In this study, 4 patients had mixed BPPV, all of whom had mixed BPPV of the posterior semicircular canal and horizontal semicircular canal. Two patients were treated with Epley reduction for the first 3 times and barbeque reduction for the fourth time. The 2 other patients were treated with the barbeque reduction method for hc-BPPV, followed by the Epley method for pc-BPPV. All the patients were cured. However, the sample size of this study was small, and a larger sample size is required to investigate and improve the structure.
In addition, 3 patients with simple pc-BPPV were treated with the Epley method; their vertigo did not decrease, and while their torsional nystagmus disappeared, horizontal nystagmus occurred. The reason may be that after pc-BPPV reduction treatment, the otolith particles mistakenly entered the horizontal semicircular canal when they moved out of the common foot of the semicircular canal. The patients were cured after barbeque treatment. Therefore, for patients with PC-BPPV, to prevent the repositioned otolith from detaching and entering the horizontal semicircular canal and causing displacement, after treatment with the Epley method, verification should not be performed immediately. We recommended that the patient rests for half an hour before verification is performed. For patients with mixed BPPV, we recommended that they rest for half an hour after a reduction of the most severely affected semicircular canal and the other semicircular canal.
It is worth mentioning that after being evaluated by the anxiety scale, 19 patients were found to have a comorbid anxiety disorder. A previous survey revealed that the incidence of mental disorders in patients with vertigo and balance disorders was between 30% and 50%. Therefore, psychological assessment and monitoring should be conducted for patients with refractory BPPV. 11
There are some limitations in this study. For example, in elderly patients, when the position changes and the head is down, they are worried about accidents caused by elevated blood pressure. So strict screening of basic diseases. In addition, the sample size of this study is small and the observation time is short. There are still many limitations in the research results, and it is hoped that a larger sample size will be obtained in the future to obtain more reliable results (has been added in the discussion section).
Conclusion
Currently, BPPV is the most common peripheral vertigo disease in clinical practice. Typical BPPV can be treated effectively with conventional reduction methods; however, the efficacy of routine reduction in treatment-refractory BPPV is suboptimal. As current domestic and international research data on refractory BPPV are scarce, there is a lack of corresponding guidance for clinical treatment.
In this study, most patients could be cured by SRM system. For patients with failed treatment by the SRM system, manual repositioning maneuvers can be attempted.
Footnotes
Data Availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was conducted with approval from the Ethics Committee of our hospital. This study was conducted in accordance with the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all participants.