
Abstract
Introduction
Salivary gland tumors are a diverse group that account for nearly 3% to 8% of all head and neck neoplasms.1-5 These lesions are variable in pathology with up to 40 histologically distinct entities, although some are exceedingly rare.1,6,7 Current literature estimates that 54% to 79% of salivary gland tumors are benign and 21% to 25% are malignant.2,8-10 Histologically, pleomorphic adenoma is the most common histological type comprising of over 50% of all salivary gland tumors, 1 while parotid gland is the most common site accounting for 80% to 85%.3,4
Most common presentation of salivary gland tumors is a painless mass. Pain, ulceration, dysarthria, and dysphagia may be the initial manifestation in about 30% of cases.1,11 Neurological symptoms such as facial numbness, tingling, weakness, or pain are typically suggestive of malignancy.2,8,12 Varied histopathologic heterogeneity and tumor location in proximity to the facial nerve poses diagnostic and management challenges. 7 Management of a symptomatic or malignant mass typically involves surgical removal, which must weigh sufficient radical removal against facial nerve preservation. 13 Surgical risks include facial nerve injury, with transient paresis in up to 20% of patients in some series.14,15
Primary malignancy of the salivary gland accounts for 0.5% to 1.2% of all malignancies.1,16,17 Malignancy typically presents in the sixth to seventh decade of life and more commonly affects women, with a male to female ratio of 1:1.5. 18 Risk factors include prior ionizing radiation, viral infection, immunosuppression, ultraviolet exposure, and occupational exposures.19,20 Most common histopathologic type of salivary gland cancer is mucoepidermoid carcinoma, which comprises about 10% of all salivary gland neoplasms and approximately 35% of malignant salivary gland neoplasms.1,21,22 Adenocarcinoma and acinic carcinoma, respectively, are the next 2 most prevalent primary malignant tumors. 19 Secondary malignant tumors of the salivary glands constitute approximately 10% of salivary gland malignancy, the majority of which are squamous cell carcinomas.19,23,24
The aforementioned prevalence figures are based predominately on the western world and Caucasian demographic. Most of the published demographic, pathological, and clinical outcome data on salivary gland tumors are based on experiences from tertiary medical centers. We hypothesized that the data obtained from tertiary care centers may be skewed toward malignant pathology and more advanced disease, as tertiary care centers often receive referrals and second opinions from community hospitals. Our study was undertaken to analyze the experience from a community setting to determine whether there are any significant differences in pathological distribution and clinical outcomes compared to the existing literature.
Materials and Methods
A case series with chart review was performed to analyze all major salivary gland tumors that presented to a large community practice, ENT Specialists, Inc, in Southern Massachusetts, with 4 satellite offices, over a 20 year period between January 2002 and December 2021. This practice included 8 board-certified otolaryngologists who operate at 4 different community hospitals, all with their own tumor review board, and all with an academic affiliation with Tufts Medical Center. This investigation received institutional review board approval from the Tufts Medical Center Review Board. Retrospective chart analysis was performed for demographic, clinical presentation, imaging, cytology, histopathology, and clinical outcome data in 806 patients. To ensure inclusivity of the data set, International Classification of Diseases, Tenth Revision (ICD-10) codes were used for parotid mass, submandibular mass, neck mass, and salivary gland malignancy. In addition, we used the Current Procedural Terminology (CPT) code for fine needle aspiration of a salivary gland mass. All fine needle aspirations were performed under ultrasound guidance in a dedicated ultrasound clinic by one operator, the senior author of this article.
Demographic information on patients with salivary gland neoplasm including gender assigned at birth and date of birth was collected. Cytology and histopathology data, when available, were analyzed. Clinical surgical outcomes included transient short-term and long-term facial nerve or sensory nerve weakness, Frey’s syndrome (postoperative gustatory sweating), seroma, salivary fistula, postoperative infection, sialocele, and recurrence. Tumor pathology was divided into benign or malignant, and further subcategorized based on pathology report. Comparisons in group proportions were performed using chi square and Fisher’s exact tests.
Results
Our study assessed major salivary gland mass characteristics and outcomes for 806 patients, 426 (52.9%) were female and 380 (47.1%) were male. The average age was 57 years.
The parotid gland was the most common site of pathology in 683 patients (84.7%), followed by submandibular in 78 (9.7%) and sublingual in 45 (5.6%). A total of 203 patients did not have a definitive histopathology as they were managed conservatively with observation alone or lost to follow-up. A total of 495 patients underwent surgical intervention within the community practice. Twenty-six patients underwent surgical excision at an outside hospital. Eighty-two patients were determined to have a benign diagnosis based on fine needle aspiration or excisional biopsy alone. Ultrasound-guided fine needle aspiration biopsy was used for 638 patients (79.2%; Figure 1). Final histopathology was benign in 508 cases (83.8%), while 98 tumors (16.2%) received a diagnosis of primary or secondary malignancy (Table 1).

Patient outcomes: flow chart demonstrating patient outcomes.
Salivary Gland Tumor Pathologies for 603 Cases.

For the parotid gland, pleomorphic adenoma (155), Warthin’s tumor (155), and cyst (55) were the most common benign diagnoses, while mucoepidermoid carcinoma (13), adenocarcinoma (8), and acinic cell carcinoma (8) were the most common primary malignancies (Tables 2 and 3).
Benign Salivary Gland Tumor Pathology for 505 Cases.

Malignant Salivary Gland Tumor Pathology for 98 Cases.

The most common benign diagnoses for the submandibular gland were pleomorphic adenoma (14), sialadenitis (10), and reactive lymph node (8; Table 2). Adenocarcinoma and myoepithelial cell carcinoma were the only 2 primary malignancies. Among all glands, there were 26 cases of lymphoma and 24 cases of metastatic squamous cell carcinoma (Table 3).
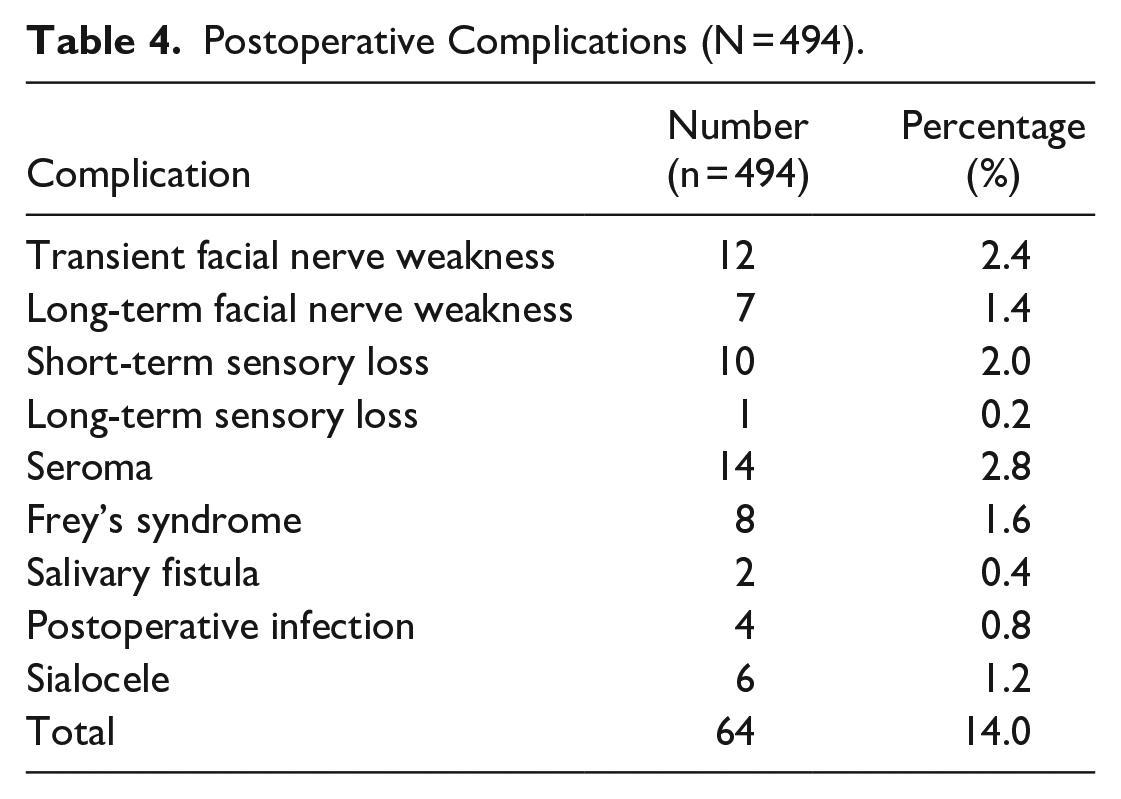
Among 494 patients who underwent surgical intervention, 64 (13.0%) reported postoperative complications. These complications include transient facial nerve weakness in 12 patients (2.4%), long-term facial nerve weakness in 7 patients (1.4%), transient sensory loss in 10 patients (2.0%), long-term sensory loss in 1 patient (0.2%), seroma in 14 patients (2.8%), Frey’s syndrome in 8 patients (1.6%), salivary fistula in 2 patients (0.4%), postoperative infection in 4 patients (0.8%), and sialocele in 6 patients (1.2%; Table 4). There were no patients with records of recurrence within the 20 year period being analyzed.
Postoperative Complications (N = 494).
Discussion
According to the American Cancer Society, 53,583 people were diagnosed with salivary gland cancer worldwide in 2020. Although, the incidence in the United States is rather uncommon as it is estimated to be 1 adult in 100,000, making salivary gland cancer less than 1% of all cancers diagnosed in the United States annually. 25 Current literature estimates that approximately 3 quarters of salivary tumors are benign, while 1 quarter are malignant.1,26 Our results on salivary gland tumor pathology derived from a community setting show a greater proportion of benign pathology compared to existing literature gathered from academic tertiary-level care centers.
We reviewed other studies assessing salivary tumor pathology performed in the last 20 years to directly compare to our study.
We compared our findings to other studies examining entire populations of people. The Arctic Inuit population became a population of special interest for salivary gland tumors in the 1920s when Johannes Fibiger reported a particularly high incidence of salivary tumors in Greenland. It was thought that malignant tumors constituted 60% of all salivary gland tumors in the Inuit population. 27 However, a study by Haugaard et al 27 analyzed data on all Greenlandic Inuit with an epithelial-derived salivary gland tumor from 1990 to 2019 and found that of 203 patients, 155 (76%) patients had benign tumors and 48 patients (24%) had malignant tumors. 27 These data are consistent with the findings in our study and suggests that the proportion of malignant salivary gland tumors in the Greenlandic Inuit population is similar to other nonendemic populations.
A study by Deschler and colleagues 28 reviewed a single surgeon’s experience with parotid masses at a tertiary-level academic center in Boston, MA, from January 2004 to December 2018. This study analyzed 924 patients who presented to a single surgeon over a 15 year period and found 70.9% of pathology to be benign and 29.1% to be malignant. 28 The similarities in sample size, timeframe, and geography make this an ideal study comparison. Our study found that at our secondary care center, 435 (83.7%) of parotid tumors were benign and 85 (16.3%) tumors of the parotid were malignant, which is significantly lower than the percentage of malignancies reported by Deschler (χ2 = 29.3, P < .001).
The subcategories of benign pathology were consistent among all studies with pleomorphic adenoma and Warthin’s tumor being the most common benign pathologies. The makeup of primary malignant pathologies also remained consistent among studies with mucoepidermoid carcinoma being identified as the most common primary salivary gland malignancy. However, our study found lymphoma to be the most common malignant pathology, while Deschler et al 28 identified metastatic squamous cell carcinoma as the most common overall malignant pathology. This may be due to the referral pattern in a tertiary care center.
When compared to the study by Deschler et al, 28 our study had significantly fewer overall complications for all patients who underwent operative management (P < .001). However, Deschler et al 28 assessed a greater amount of malignant salivary gland tumors. His study showed that selective nerve branch sacrifice was required in 114 total cases (12.3%) and 91 cases of malignant tumors (33.8%). 28 Our study’s complication rate (13.0%) is very comparable to the complication rate for benign tumor surgical intervention assessed by Deschler et al 28 (12.2%). Clinical outcomes data from our study show a low proportion of short-term adverse outcomes such as facial nerve paralysis or Frey’s syndrome and an even lower proportion of long-term adverse outcomes including long-term facial nerve paralysis or recurrence. These findings support the idea that identification and management of salivary gland pathology can be safely performed within a community care center. However, while the outcome data on surgical treatment of benign tumors are comparable to the existing literature, the same conclusion cannot be drawn for malignant tumors, given relatively small numbers in our series and likely disparity in the complexity of the surgical cases in tertiary care centers.
A study by Parikh and colleagues 29 identified 200 patients through the Massachusetts Eye and Ear Infirmary institutional cancer registry treated for malignancies of the parotid gland alone over a 10 year period (January 2005-December 2014). Our study which reviewed data over a 20 year period identified only 101 tumors of primary or secondary malignancy among all 3 salivary glands. Parikh et al 29 identified nearly twice as many patients with salivary gland malignancies in half of the time. This difference in incidence of malignancy may be a result of the difference in volume of patients seen by a tertiary-level care center receives versus community centers. However, this study did not assess the proportion of benign and malignant pathology among all salivary tumors.
Knopf and colleagues 30 assessed 1211 patients presenting to a tertiary-level care center with parotid pathology over a 20 year period from January 1993 to July 2013. Their study identified 946 (78%) benign and 265 (22%) malignant tumors of the parotid gland. 30 Our study of 806 tumors over a 20 year period identified a greater proportion of benign pathologies, with 435 (83.7%) benign and 85 (16.3%) malignant, which is significantly lower than the percentage of malignancies reported by Knopf (χ2 = 6.92, P < .01).
Compared to the existing literature, derived from tertiary care centers, our data derived from a community health center showed a smaller percentage of malignant salivary gland tumors. Although these results are statistically significant, our study is limited by its design as a retrospective study as well as its narrow geographic distribution. However, same conclusions can be drawn by comparing data drawn from similar geographic distribution in studies by Deschler et al 28 and Parikh et al. 29 This also holds truth while comparing with other studies such as Knopf et al 30 performed over similar time period.
Conclusion
Our study found a greater proportion of benign pathology compared to the existing data. The existing literature may be skewed toward malignant burden among salivary gland tumors due to referral pattern to tertiary care centers, more advanced patient presentations, and complex pathologies at tertiary care centers.
Our data on clinical outcomes show that successful identification and management of benign tumors can safely be undertaken in a community setting, with results being comparable to those achieved in the academic tertiary care setting. However, given small amount of identified malignancies and likely higher complexity of the surgical cases in tertiary care centers, more information is needed regarding outcome of malignant salivary tumor.
Footnotes
Authors’ Note
This work was presented as a podium presentation at the American Academy of Otolaryngology—Head and Neck Surgery Foundation 2022 Annual Meeting and OTO Experience, Philadelphia, PA, September 10 to 14, 2022.
Author Contributions
ES: primary author, data collection and analysis. CZ: data collection and analysis, review and editing. JKD: senior author, concept, supervision, review, and editing.
Data Availability
The data that support the findings of this study are available on request from the corresponding author, JKD. The data are not publicly available due to information that could compromise the privacy of research participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the institutional review board of Tufts Medical Center.