
Abstract

Significant Statement
Benign fibrous histiocytoma (BFH) is a soft tissue tumor that may present as a fibrous mass anywhere in the body. BFH is rare in head and neck region, and very few cases with nasal involvement have been reported in literature till date. This tumor is originated from undifferentiated mesenchymal stem cells and has fibrous and histiocytic elements. We hereby report an interesting and a rare case of BFH at nasal tip in a 9-year-old girl along with its management and follow-up.
Case Report
A 9-year-old girl presented to the pediatric otolaryngology department of our institute with the complaints of painless mass over the nasal dorsum. The mass started as a small nodule over nasal tip and had been growing slowly for 3 years. There was no history of trauma, previous surgery, or similar lesions on the body. There were no complaints of nasal obstruction or discharge from the swelling. On examination, a localized, firm, non-tender, oval swelling of about 1.5 cm × 1.5 cm was noticed over right side of nasal tip (Figure 1a). The overlying skin was tense and adhered to the swelling. Clinically, the findings were suggestive of soft tissue neoplasm. No significant cervical lymphadenopathy was noticed. No abnormality was evident on nasal endoscopy. Keeping differentials of dermoid, fibroma, and nasal cyst/glioma, a magnetic resonance imaging (MRI) was done. MRI findings were suggestive of well-localized nasal mass with no intracranial or intranasal extension.
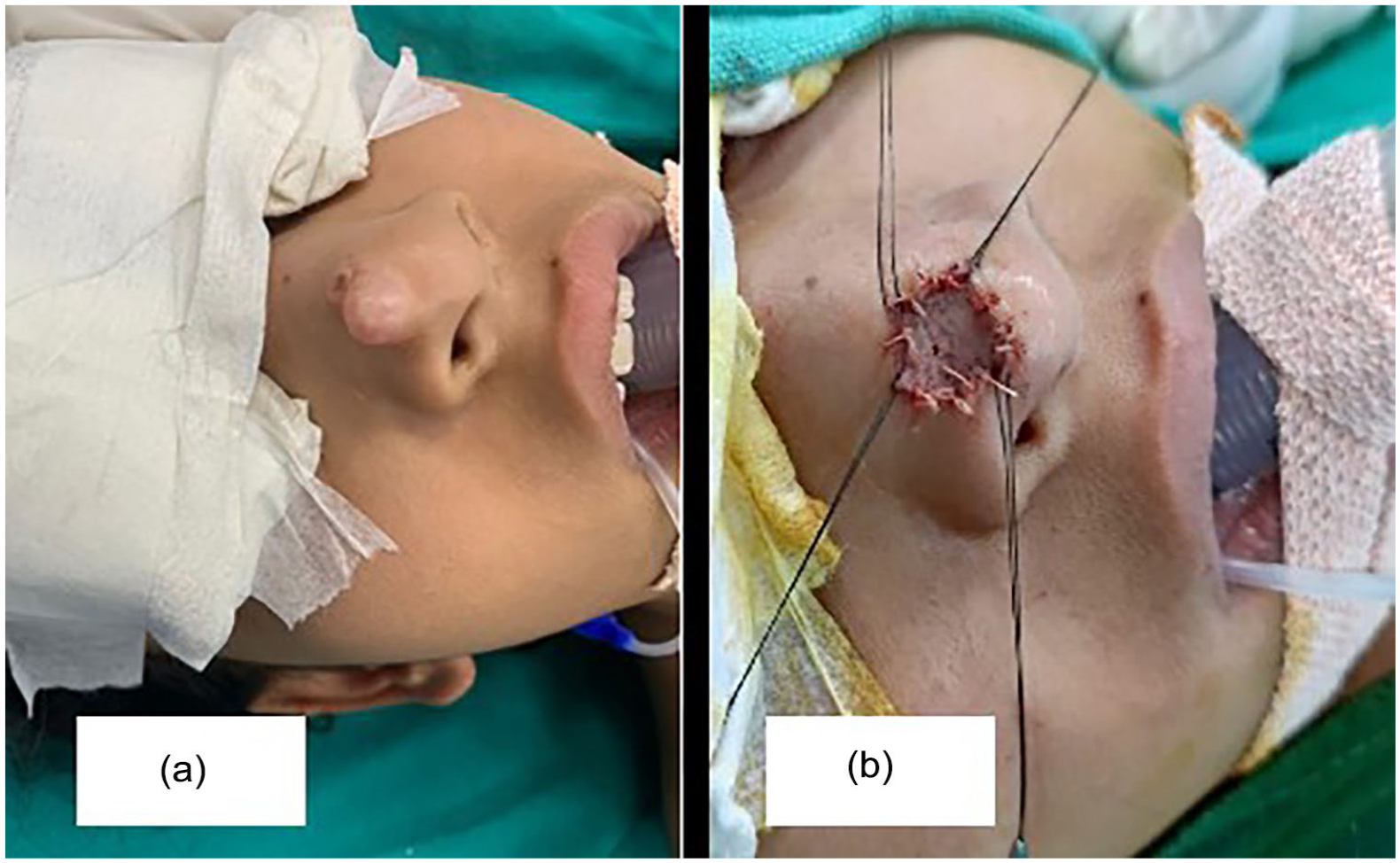
Intraoperative images. (a) Swelling over right-side tip of nose. (b) Swelling excised and defect is covered using full-thickness skin graft harvested from postauricular region.
A provisional diagnosis of benign nasal mass was made, and child was taken up for surgical excision (Figure 1b) under general anesthesia. The mass was excised completely in toto and defect was covered with postauricular full-thickness skin graft. Histopathological examination (H & E) confirmed the diagnosis of a BFH (Figure 2). After a year, postoperative follow-up showed good cosmetic outcome with no recurrence (Figure 3).
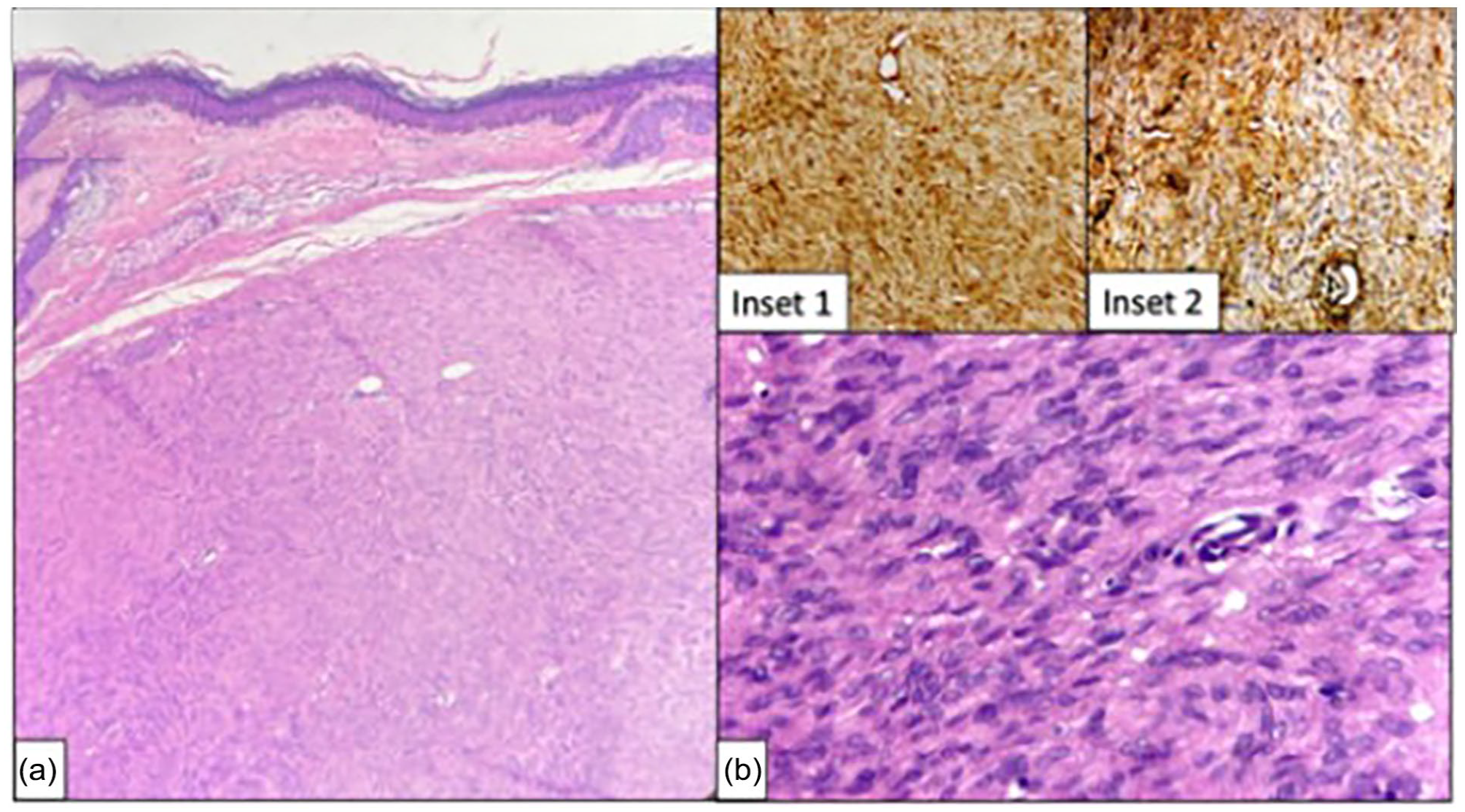
Histopathological findings. (a) The dermis showing a well-circumscribed and nonencapsulated spindle cell lesion with largely unremarkable epidermis Histopathological examination (H&E, 20×). (b) The spindle cells are arranged in storiform pattern along with few histiocytic cells (H&E, 40×). Inset 1: The spindle cells showing diffuse expression of vimentin Diaminobenzidine (DAB chromogen, 20×). Inset 2: The spindle cells showing focal expression of CD34 (DAB chromogen, 20×).

Result after 12 months follow-up.
Discussion
Benign fibrous histiocytomas (BFH) are common mesenchymal tumors found in skin and in deep soft tissues. This tumor is originated from undifferentiated mesenchymal stem cells and has fibrous and histiocytic elements. 1 BFH is rare in head and neck region.2,3 The etiology of BFH is not known exactly, mostly it is found in the sun-exposed sites, areas of trauma, chronic irritation, and recurrent infections. 3 Fibrous histiocytoma can present as malignant fibrous histiocytoma or BFH. 4
Very few cases of BFH with nasal involvement have been reported in pediatric age group. BFH is usually present as a slow-growing painless mass with symptoms related to invasion of anatomy around it. 5 Similarly, in our case, a small swelling was started 3 years ago, which grew slowly to involve overlying skin. Clinically, it looks like a soft tissue neoplasm, therefore, the child was planned for surgical excision and skin grafting to achieve cosmesis.
Imaging tools like computed tomography and MRI are used to find out extent and nature of the lesion but for such cases, biopsy is required for definitive diagnosis. The BFH has a controversial diagnosis because of its uncertain histology. 2 Pathological diagnosis of such lesions is challenging in most of the cases and based on light microscopy and immunohistochemistry. 4 On histopathological examination, we found spindle cells arranged in the storiform pattern along with few histiocytic cells.
The treatment of choice for BFH is en bloc surgical excision. 1 Generally, prognosis of typical BFH is excellent but they can recur if not excised completely. 1 Although no metastasis has been reported, close follow-up is recommended. 1
Conclusion
BFH is rare but should be considered in cases of slow-growing head and neck masses. Clinically they mimic soft tissue neoplasm and biopsy is required for definitive diagnosis. Therefore, such cases need to be addressed on priority and wide local excision is treatment of choice.
Key Points
Very few cases of nasal benign fibrous histiocytoma are reported in pediatric cases.
These are challenging cases to achieve cosmesis.
Definite diagnosis is made only with histology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written consent to publish was obtained from patient and her parents.