
Abstract
Adult-onset lymphatic malformations arising at the postcricoid, a subsite of the hypopharynx, are sporadic. Only one case has been previously reported. In this study, we presented a 36-year-old female presented with globus sensation, dysphagia, and upper airway obstruction, requiring a tracheostomy. A computed tomography scan identified a 5 cm × 4.5 cm × 3 cm multilocular hypodense lesion in the postcricoid. Due to its considerable size, complete resection with function preservation was crucial, and a standard microscopic direct laryngoscopy approach may result in inadequate exposure, while an open transcervical approach may affect functional outcomes and increase surgical complications. We successfully performed an en bloc resection with a transoral endoscopic approach, using laryngeal suspension and a laparoscopic ultrasonic scalpel to preserve aerodigestive functions, ensure rapid recovery, and avoid neck scarring. The patient was decannulated within 2 weeks and remained disease-free after 1 year. The reported cases of adult-onset lymphatic malformations at the postcricoid and hypopharynx were reviewed and summarized for educational purposes.
Introduction
Lymphatic malformations are rare, congenital, aberrant growths of lymphatic vessels, approximately 90% being diagnosed in children within the first 2 years of life.1,2 Although the terms cystic hygroma or lymphangioma have been used, the term lymphatic malformation emphasizes the congenital aspect of the lesion with no suggestion of neoplasm.3,4 Areas of the body rich in lymphatics are most frequently affected, with 75% occurring in the head and neck.1,3,5 They are often asymptomatic unless they involve or originate in the airway or pharynx, resulting in stridor or dysphagia. 4 Lymphatic malformations in the upper aerodigestive tract in all age groups have been reported as having an incidence of 19.7% in the head and neck. 6
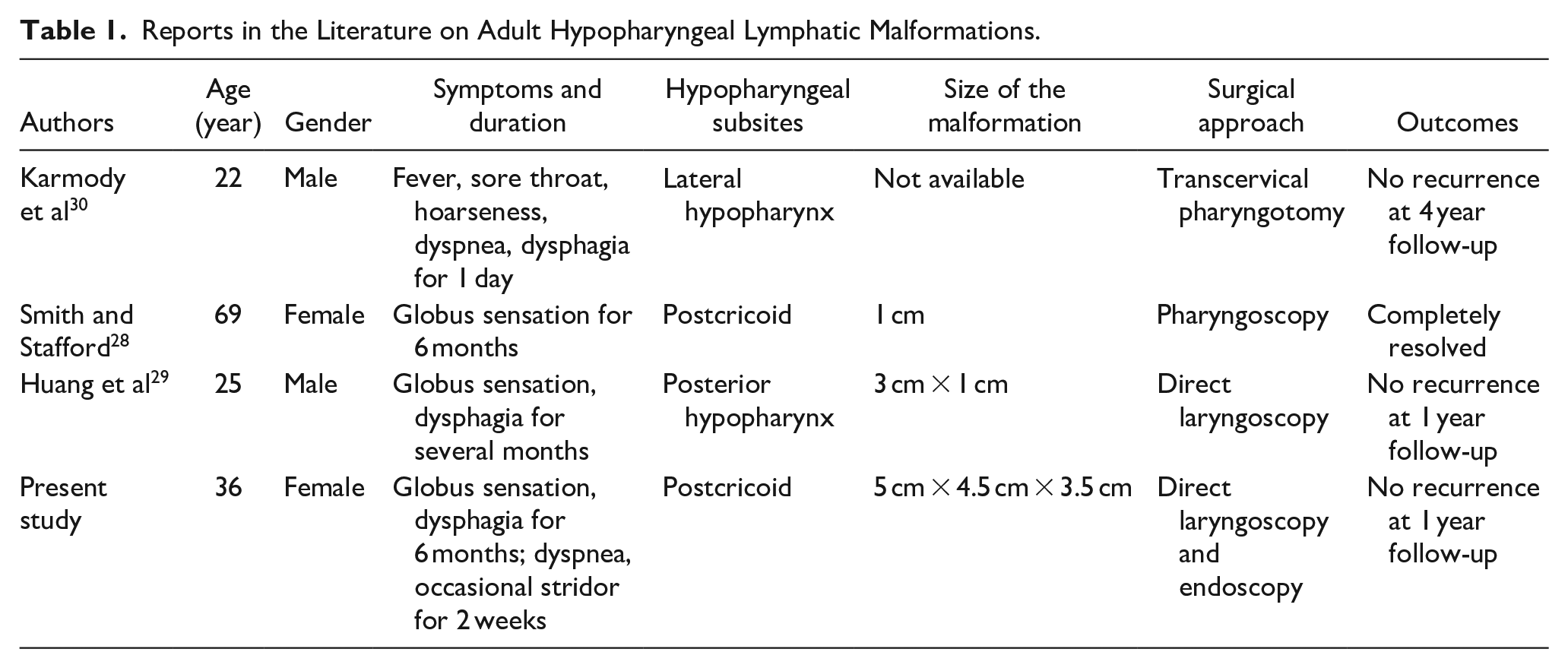
In the adult population, lymphatic malformations are sporadic. Approximately 150 cases have been reported in the head and neck area.1,2,4,7,8 They mainly occur in the neck, and those that arise in the upper aerodigestive tract are rare. The most frequently reported sites are the oral tongue (approximately 30 cases),9-13 followed by the tonsil (27 cases),14-18 then the supraglottic larynx (19 cases).19-27 Adult hypopharyngeal lymphatic malformations have been previously reported in 3 cases,28-30 with only one case occurring at the postcricoid 28 (Table 1).
Reports in the Literature on Adult Hypopharyngeal Lymphatic Malformations.
This study aims to report on a hypopharyngeal lymphatic malformation originating at the postcricoid in an adult patient and review similar articles regarding clinical features, investigation, and management.
Case Presentation
A 36-year-old female presented with a globus sensation and dysphagia for 6 months. She developed progressive dyspnea and occasional stridor for 2 weeks. She denied recent infection or trauma of the upper aerodigestive tract. The patient had no known drug or food allergy and no history of smoking, alcohol, or drug abuse. She had no family history of cancer or genetic disorders and had never undergone surgery. At the emergency department of a local hospital, her vital signs were within normal limits, with the respiratory rate at 20 breaths/minute. She had a mild degree of inspiratory stridor. The neck examination was unremarkable. A fiberoptic laryngoscopy revealed a large, smooth surface cystic mass in the hypopharyngeal area that obstructed the laryngeal inlet. The routine blood investigation tests were within normal limits. A contrast-enhanced computed tomography (CT) scan of the head and neck revealed a multilocular hypodense lesion, size 5 cm × 4.5 cm × 3 cm, originating from the postcricoid region which occupied the supraglottic area, causing airway narrowing (Figure 1). The patient was transferred to the operating room for a tracheostomy. A direct laryngoscopy and biopsy were performed, and the pathological results were consistent with lymphatic malformation. The patient was referred to our hospital, a tertiary-level care center, for definitive treatment.
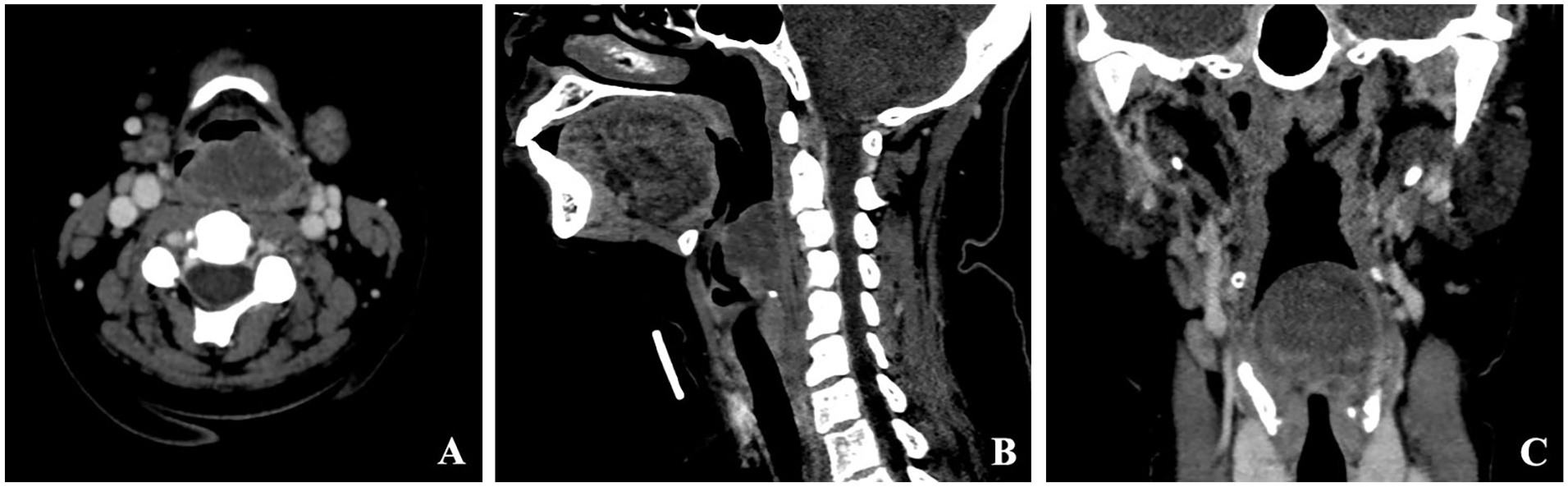
Computed tomography scan of the head and neck revealed a multilocular hypodense lesion originating from the postcricoid region, extending upward posterior to the epiglottis (A = axial view, B = sagittal view and C = coronal view).
The surgical option of a transoral approach was introduced to the patient with the possibility of a transcervical pharyngotomy in case of unsuccessful transoral resection. The suspension Lindholm laryngoscope was employed to assess the mass extension, revealing primary involvement at the postcricoid, with an upward extension to the posterior surface of the arytenoids (Figure 2).
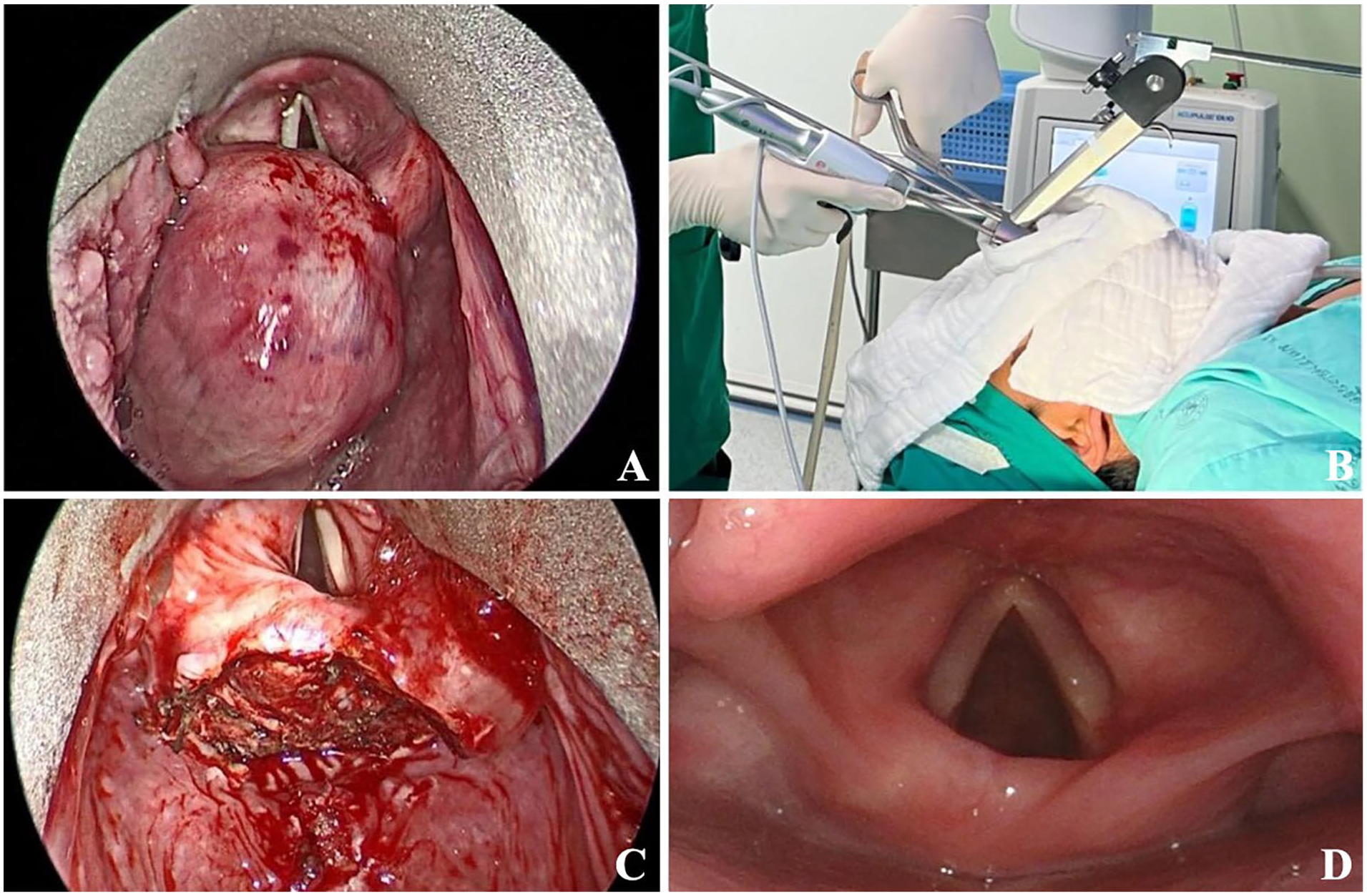
Intraoperative photographs showing (A) the postcricoid lymphatic malformation during the transoral direct laryngoscopy (B) with endoscopic-assisted approach, (C) the postcricoid area after complete resection, and (D) the laryngoscopic examination at 1 year follow-up.
A microscopic direct laryngoscopy with CO2 laser excision failed initially because the large size of the mass prevented total exposure. A 5 mm, zero-degree rigid endoscope with a high-definition camera was applied, allowing total mass exposure. The assistant controlled the endoscope, allowing the surgeon to use instruments with both hands. We used laryngeal forceps and a laparoscopic ultrasonic scalpel to completely resect the mass from its attachments allowing preservation of the arytenoids and posterior cricoid lamina (Figure 2).
The specimen was a 5 cm × 4.5 cm × 3.5 cm tan-red mass with smooth mucosa (Figure 3A). The histological examination revealed benign squamous epithelium with the stroma underneath containing varying sizes of thin-walled lymphatic channels and lymphoid follicles (Figure 3B and C). The final pathologic report was consistent with lymphatic malformation with complete excision.
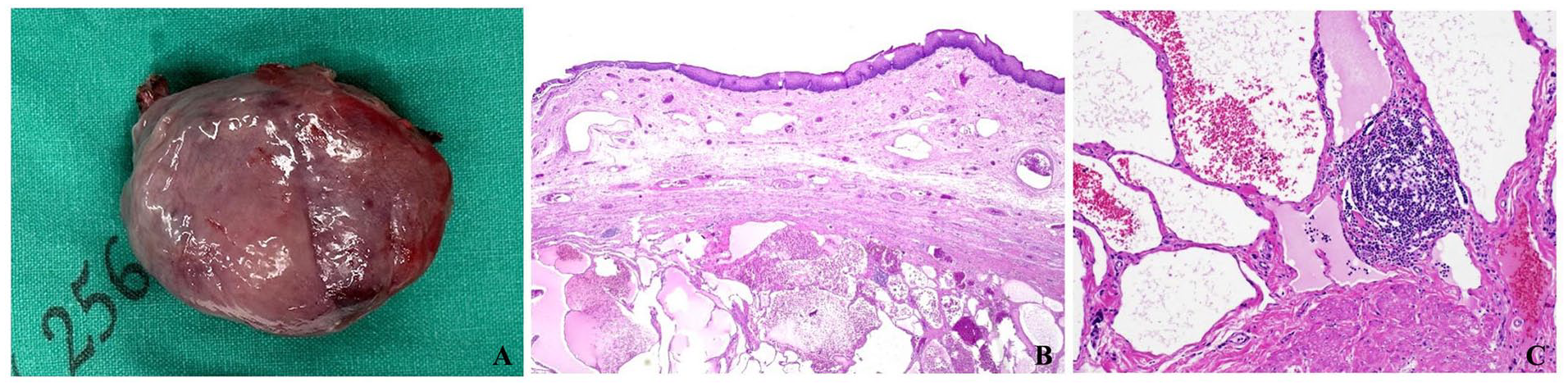
(A) Photograph of a tan-red mass, measuring 5 cm × 4.5 cm × 3.5 cm, with a smooth mucosal covering. (B) Photomicrographs of the lymphatic malformation showing benign squamous epithelium with the underneath stroma containing an area of lymphatic channels varying in size filled with pink proteinaceous fluid and blood. (C) The mass comprised numerous lymphatic channels with lymphoid follicles and fibrous tissue in between (hematoxylin-eosin stain, 100× magnification).
The wound was left for secondary healing. The patient’s recovery proceeded without complications. Voice and swallowing abilities showed marked improvement within 1 week. Successful tracheostomy tube decannulation was performed 2 weeks postoperatively. After 12 months of surveillance, there was no evidence of recurrence.
Discussion
Benign neoplasms of the hypopharynx are uncommon compared to their malignant counterparts; the most common are fibrolipoma and leiomyoma. 31 In addition, benign hypopharyngeal cysts are extremely rare, with the differential diagnosis including retention cysts, bronchogenic cysts, lymphoepithelial cysts, and vascular malformations. 32
Vascular malformations are one of the subtypes of vascular anomalies besides vascular tumors and can be categorized from their constituent malformed vessel type(s) into capillary, lymphatic, venous, and arteriovenous.3,5
There are 3 theories regarding the etiology of lymphatic malformations, including an arrest of the normal growth of primitive lymph channels, lymph channels not reaching the venous system, and lymph channels lying in the wrong areas.8,33 These theories are derived from the abnormal development of the lymphatic system. First, during the embryonic period, the primary lymphatic plexus is established and matures into a hierarchical network with the formation of lymphatic and lymphovenous valves that ensure unidirectional lymph flow to the venous circulation. Second, after birth, lymphatic capillary junctions connecting the lymphatic and venous circulation are developed. In addition, genetic mutation encoding the RAS-MAPK (Mitogen-activated protein kinase) pathway may lead to the formation of ectopic lymphatic vessels with abnormal development of lymphatic valves. 34 However, the etiology of adult lymphatic malformations is controversial. It is thought to occur due to the delayed proliferation of cells rests from acquired processes such as infection, inflammation, trauma, or lymphatic obstruction.1,2,4,7
Due to the indolent nature of the disorders, patients may be asymptomatic or have nonspecific symptoms. Clinical presentation depends on the location, size, and rate of growth. Lymphatic malformations of the upper aerodigestive tract may have significant local effects on deglutition, phonation, and airway patency. From the literature review, the common presenting symptoms of hypopharyngeal lymphatic malformations were globus sensation and dysphagia, which occurred for several months.28,29 In the present case, the mass originated from the postcricoid and extended to the laryngeal inlet, initially causing dysphagia and subsequently leading to upper airway obstruction, necessitating a tracheostomy. Although there was no history of infection, trauma from deglutition may have caused the recent enlarging of the mass. Airway obstruction was also observed in a previous report, and the precipitating cause was local infection. 30
The disorders are known to be associated with abnormal chromosomes, such as Down syndrome, Turner syndrome, and Noonan syndrome. 8 The present patient has no evidence of these abnormalities.
Magnetic resonance imaging (MRI) and contrast-enhanced CT scans have been used to investigate lymphatic malformations for diagnostic evaluation, determine the lesion extent, and guide treatment decisions.4,7,29 The MRI may demonstrate the characteristic findings of a cystic lesion as hypointense on T1-weighted images and hyperintense on T2-weighted images. 29 However, the CT scan may show a water-density mass with a mild peripheral rim enhancement. 4 In the present case, the CT scan proved adequate for radiologic diagnosis and demonstrating the origin of the lesion.
Treatment modalities for lymphatic malformations include observation, steroids, cauterization, sclerotherapy, and surgical resection, of which surgical excision and sclerotherapy produce better responses.2,8
Although the efficacy of sclerotherapy is comparable to that of surgical excision with a volume shrinkage of ≥60% in macrocystic lesions, 2 evidence supporting the use of sclerotherapy in adult patients is still lacking, and a 60% shrinkage of the aerodigestive lesion is unacceptable. 2 In addition, sclerotherapy-induced fibrosis may produce organ dysfunction and difficulty in surgical resection in recurrent lesions. 23
Regarding the treatment of adult hypopharyngeal lymphatic malformations from the literature review, there are 2 reports of small lesions being removed transorally, in which Smith and Stafford 28 described the “polyp-like” 1 cm mass was avulsed from the postcricoid area under pharyngoscopy, while Huang et al 29 reported that the mass, approximately 3 cm × 1 cm in size, was completely excised via direct laryngoscopy. However, Karmody et al 30 detailed the mass (not mentioning the size) at the lateral hypopharyngeal wall causing airway obstruction was incompletely excised via transcervical lateral pharyngotomy approach, and there was profuse drainage of serous fluid from the neck wound for 2 weeks after the operation 30 (Table 1).
In the era of minimally invasive surgery, approaches toward the larynx and hypopharynx have evolved, shifting from open transcervical surgery to transoral procedures. 35 The advantages of transoral surgery include faster functional recovery, reduced hospital stay, and the absence of neck scarring. In the present case, the transoral approach posed technical challenges due to the large size and location of the mass. An initial attempt to utilize a microscopic direct laryngoscopy proved inadequate for proper exposure. As a result, we opted for endoscope-assisted surgery through the suspension laryngoscope. This approach conferred several benefits: it permitted navigation around the mass, unrestricted by the line-of-sight constraints of microscopic CO2 laser surgery; it allowed for the use of various instruments, such as ultrasonic scalpel or monopolar cautery, enhancing complete resection of the mass. It also significantly reduced operation costs compared to a transoral robotic approach while achieving similar outcomes.
Despite their rarity and benign nature, lymphatic malformations may affect the adult hypopharynx, impairing upper aerodigestive function. Physicians must recognize this malformation as a potential diagnosis in cases presenting similar symptoms. Employing a transoral direct laryngoscopy with an endoscopic-assisted approach allows complete excision of the malformation while preserving function.
Footnotes
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval has been exempted by the Research Ethics Committee of our institution (exemption number 0358/2023).
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.