
Abstract

Significant Statement
Axenfeld-Rieger Syndrome (ARS) is a rare genetic condition resulting in a variety of ocular, dental, facial, and abdominal congenital defects. Mutations in transcription factors PITX2 and FOXC1 are responsible for the majority of ARS cases. Despite the constellation of symptoms expressed by both genotypic variants, including difficulty airway, there have been no documented cases relating ARS to tracheal abnormalities. We present the first documented case of tracheal abnormality in a patient with ARS.
Case Presentation
A 68-year-old female former singer with a past medical history significant for Axenfeld-Rieger Syndrome (ARS) was referred to a laryngology clinic to reestablish care, “needing a tracheotomy for a hernia repair.” She reported a long history of difficult intubations that first occurred during a combined septoplasty, inferior turbinate reduction, and uvulopalatopharyngoplasty in 1996 when she required an emergent tracheotomy for intraoperative acute respiratory obstruction. Despite decannulation the following day, the patient reported that her singing voice suffered as a result. In 2016, she presented to laryngology clinic with sleep apnea and an inability to tolerate Continuous Positive Airway Pressure (CPAP). A partially circumferential tracheal web resulting in a 30% to 40% narrowing was found on flexible laryngoscopy (Figure 1). This was presumed iatrogenic, given the proximity to the tracheotomy stoma. A flat widened trachea was also noted, which was consistent with tracheomalacia. A second tracheotomy was performed in 2016 for obstructive sleep apnea. The postoperative course was complicated by persistent tracheitis requiring antibiotics and prolonged hospitalization. She had a persistent cough for months despite maximal medical management. Decision to decannulate resulted in a significant reduction in her cough. An elective hernia repair in 2023 was aborted due to a difficult intubation resulting in intraoperative bradycardia and hypoxia. The patient presented to laryngology clinic requesting a third tracheotomy to proceed with a future ventral hernia repair.
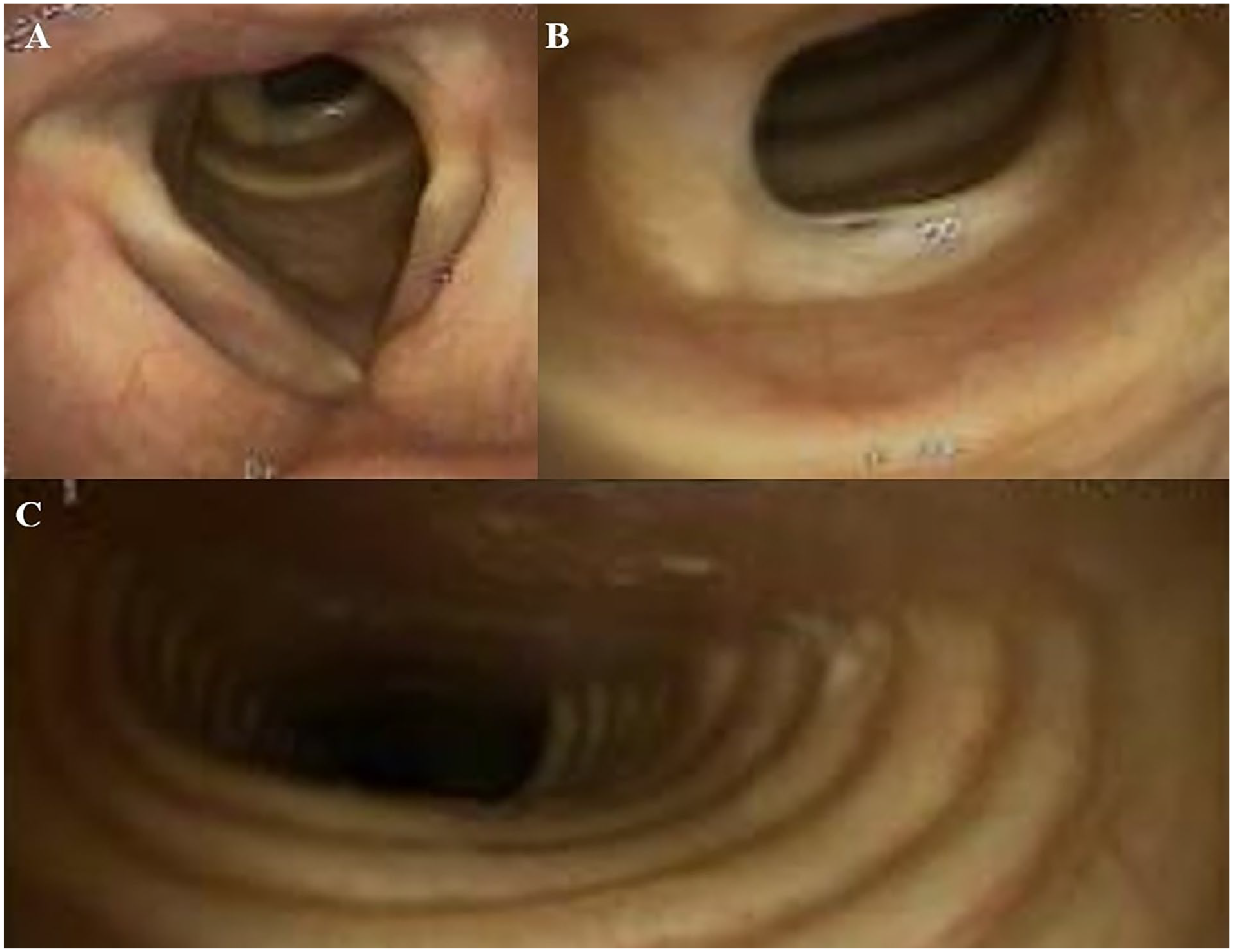
(A and B) A partially circumferential tracheal web with 30% to 40% narrowing is shown on flexible laryngoscopy in 2016. (C) Significant flattening of the tracheal rings is noted during quiet respiration.
Past medical history is significant for cataracts, glaucoma (right eye), right-sided hearing loss (status-post stapedectomy), gastroesophageal reflux disease (GERD), chronic obstructive pulmonary disease (COPD), sleep apnea with CPAP intolerance, obesity hypoventilation syndrome, and morbid obesity. Family history is notable for a daughter born with tracheomalacia who passed away in infancy and an older brother who passed away shortly after birth from an unknown cause.
On physical examination, she was noted to have a tracheocutaneous fistula. Transnasal tracheoscopy was performed, which confirmed the presence of the partially circumferential tracheal web resulting in 50% tracheal stenosis (Figure 2) adjacent to the prior stomal site and tracheomalacia. Options regarding airway management were discussed. Given that her pressing need was tied to a possible hernia surgery, she opted to defer management while waiting for a second opinion for revision ventral hernia surgery.
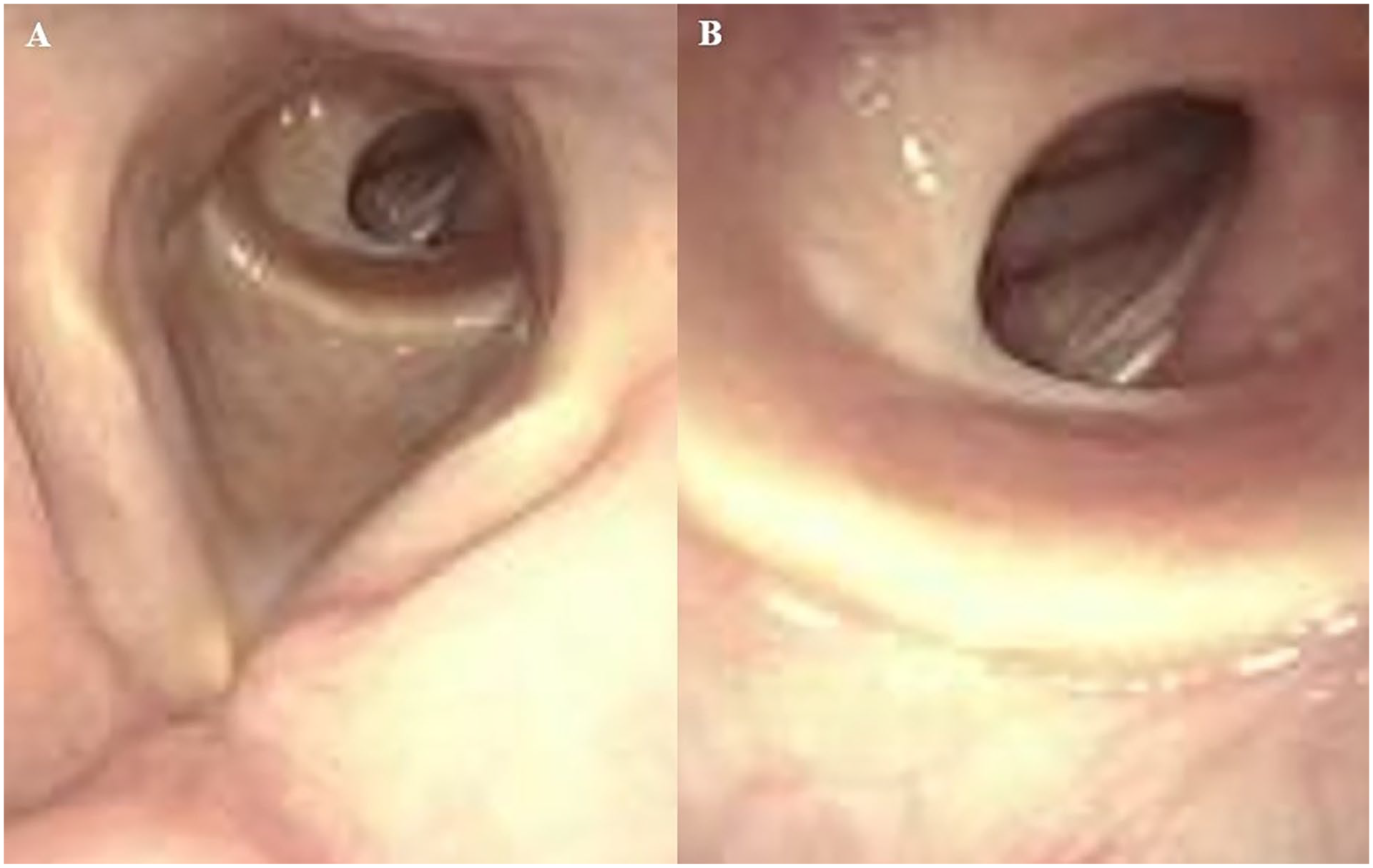
(A and B) A partially circumferential tracheal web with 50% narrowing is shown on flexible laryngoscopy in 2023.
Discussion
ARS is a rare genetic condition believed to be the result of abnormal neural crest migration resulting in a variety of ocular, dental, facial, and abdominal congenital defects. 1 ARS has been linked to genetic mutations in several chromosomes affecting transcription factors such as PITX2 and FOXC1. 1 ARS is classically divided based on the subsequent clinical malformations expressed. 1 Axenfeld anomaly is an anteriorly displaced, prominent Schwalbe line delineating the outer corneal endothelium (“posterior embryotoxon”) resulting in an adherent iris and increased risk for glaucoma. 1 The Rieger anomaly refers to central iris defects (ie, pseudopolycoria, ectropia uveae). 1 Rieger syndrome describes patients with the Rieger anomaly and systemic features such as facial dysmorphisms, dental dysplasia, maxillary hypoplasia, hearing loss, and cardiac anomalies. 1
Presently, ARS is characterized into ARS type I (heterozygous variants of PITX2), ARS type II (no specific gene variant), and ARS type III (heterozygous variants of FOXC1). 2 More recently, it has been proposed that ARS should be subcategorized based on mutations in the 2 distinct transcription factors PITX2 and FOXC1, responsible for 71% of ARS cases. 2 Both variants are associated with ocular malformations, congenital heart disease, feeding difficulties, hypotonia/early delay without cognitive impairment, and joint/skeletal anomalies. 2 Microdontia/hypodontia, umbilical anomalies, and Meckel diverticulum were highly specific for PITX2 variants. 2 Widely spaced eyes, enamel hypoplasia/frequent dental caries, dental crowding, hearing loss, and hip anomalies were specific to FOXC1. 2
Despite the focus on the ophthalmological complications of ARS, the consequential-associated systemic malformations highlight the importance of a multidisciplinary approach. To the otolaryngologist, ARS can present as hearing loss (sensorineural, conductive, mixed) 3 and complications from craniofacial dysmorphisms. 4 While this patient’s ARS diagnosis was made phenotypically based on ocular characteristics, incorporating genetic information into the clinical management can provide invaluable information when managing systemic ARS complications. Recently, the incorporation of routine audiologic evaluations in FOXC1-variants has been advocated. 2
While ARS craniofacial and dental anomalies can result in difficulty in securing an airway, 5 to our knowledge, tracheal abnormalities such a tracheomalacia have not been described. It is possible that the tracheomalacia led to poor toleration of the tracheotomy tube secondary to coughing. Furthermore, it is unclear if this genetic syndrome would result in more frequent occurrence of iatrogenic subglottic stenosis. While the FOXC1 transcription factor has not been previously documented to be associated with tracheal defects, disruption of the closely related transcription factor FOXF1 6 —an essential transcription factor for tracheal development 7 —has been shown to be intrinsically related to the development of tracheomalacia. 8 Despite the unclear association between these distinct yet phylogenetically-related genes as it pertains to ARS, this patient’s history of difficult intubations, tracheomalacia, and a tracheal web along with a family history of tracheomalacia requires further investigations into a possible underlying association between ARS and acquired or congenital tracheal abnormalities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.