
Abstract
Spontaneous oropharyngeal bleeding is an uncommon but serious medical emergency mainly caused by accidental trauma or post-tonsillectomy. In extremely rare cases, it can be attributed to arterial pseudoaneurysm (PA) of head and neck vessels. The authors present the case of a young female patient presenting with recurring spontaneous oropharyngeal bleeding who was found to have a lingual artery PA on angiography. Due to the active nature of the hemorrhage and extensive blood loss, embolization of the tonsillar branch of the lingual artery was successfully performed. When evaluating patients with spontaneous oropharyngeal bleeding, one should suspect the presence of an arterial PA, especially if the bleeding recurs following initial conventional interventions.
Introduction
Spontaneous oropharyngeal hemorrhage (SOH) is an uncommon but potentially life-threatening medical emergency that often presents a diagnostic challenge for healthcare providers. A wide range of etiological factors can underlie this phenomenon including trauma, coagulopathies, infections, inflammatory conditions, and rarely vascular lesions, such as pseudoaneurysms (PAs).1-4
Arterial PAs in the head and neck region are characterized by anomalous dilations in the wall of the lingual, facial, or other branches of the external carotid arteries, which can lead to spontaneous bleeding into the oropharynx without a history of trauma or evident injury. PAs most commonly arise secondary to disruption of the arterial wall integrity from direct trauma, which can be accidental or post-tonsillectomy.5,6 However, the spontaneous occurrence of oropharyngeal bleeding secondary to a PA, in the absence of trauma or surgery, has been rarely reported.
Through this case report, we seek to enhance the medical community’s awareness of this rare condition considering its potential for severe hemorrhagic events and underscore the significance of an in-depth in-vestigation.
Case Presentation
A 19-year-old female, previously healthy, with a recent history of recurrent acute tonsillitis (5 episodes in the past year), presented to the emergency department for spontaneous episodes of oral cavity bleed of 5 days duration. She describes having multiple episodes of oozing blood from the oral cavity over several days. Prior to presentation, the patient had a self-resolving viral tonsillitis that was not treated with antibiotics. Upon examination, she denied any fever or chills, odynophagia, or decrease in her oral intake. Past medical history is negative for any bleeding disorder, recent trauma, or voice overuse.
On physical examination, the patient had a grade 3+ tonsil on the right with one blood streak overlying the tonsil and a grade 2+ tonsil on the left. There was no erythema or exudates. Moreover, the uvula was midline, with no bulge or palpable fluctuance over the soft palate. The patient had no trismus with a normal range of motion of the neck. Flexible fiberoptic laryngoscopy through both nasal cavities showed minimal blood streaks over the posteromedial surface of the right tonsil. A few hours later, while being observed in the ER, the patient developed an episode of active bleeding, which required imaging for evaluation.
Computed tomography angiogram (CTA) of the neck showed bilateral tonsillitis with a right rim enhancing collection measuring 1.8 × 1.5 × 2.6 cm and fat stranding, reaching the parapharyngeal space suggestive of intra-tonsillar abscess. In addition, a focus of contrast extravasation within the collection on the arterial phase and the absence of a significant blush on the venous phase were identified, suggestive of PA formation (Figure 1a and b). Laboratory tests were normal and did not show leukocytosis. Blood and throat cultures were negative for beta-hemolytic streptococci groups A, C, or G.
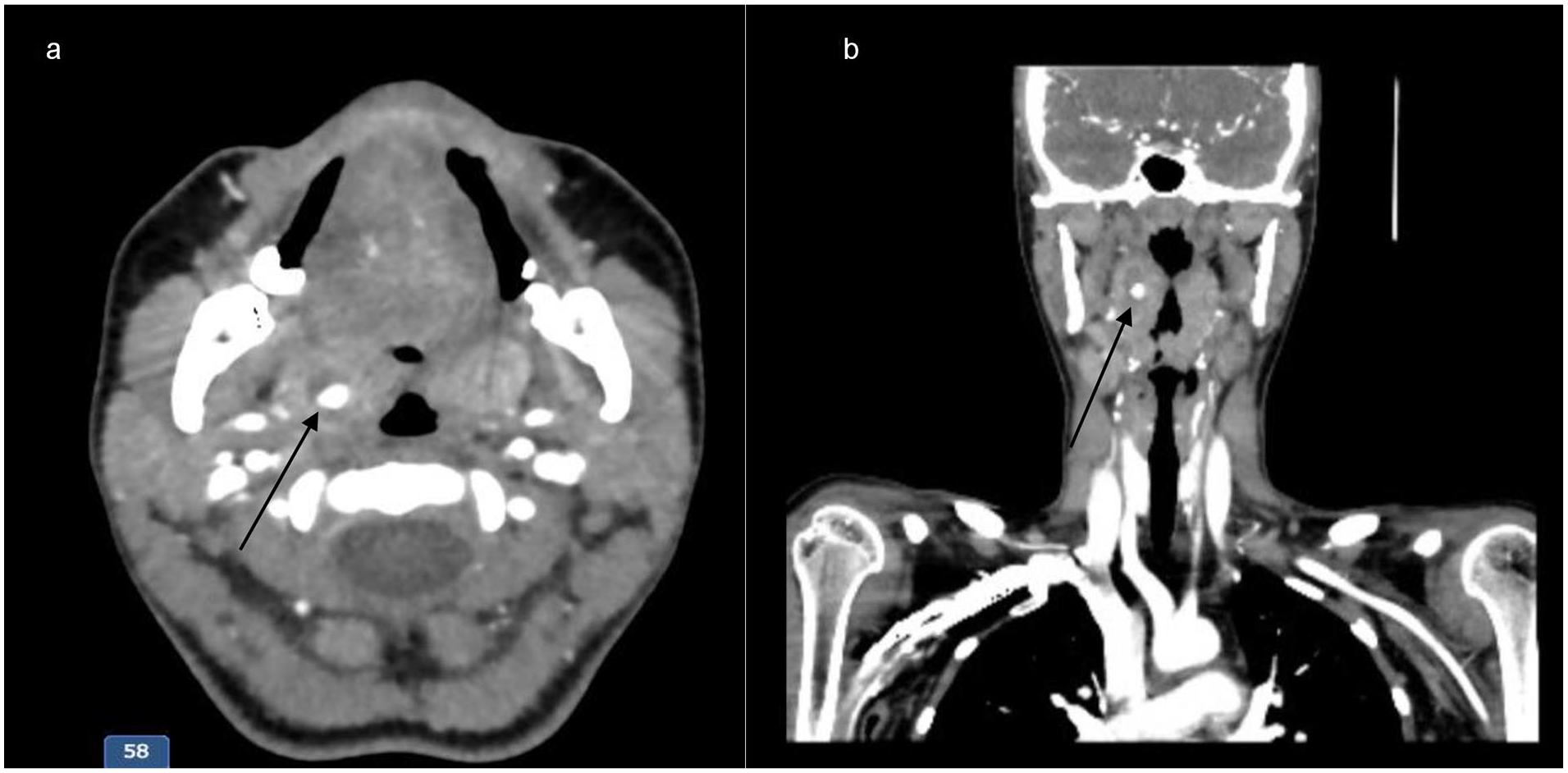
(a) Axial CT scan in the arterial phase shows contrast enhancement in the area of the PA; (b) coronal CT scan in the arterial phase shows contrast enhancement in the area of the pseudoaneurysm. PA, pseudoaneurysms; CT, computed tomography.
The patient was admitted and started on intravenous antibiotics with 900 mg clindamycin q8h and 2 g ceftriaxone q24h. A few hours after admission, the patient had an acute episode of oral cavity bleeding. She was selectively intubated for airway protection and the interventional radiology team was consulted for embolization. However, radiologists did not visualize any active bleeding and could not intervene. The parotid, infra-temporal, submandibular, and carotid spaces were normal. Twenty-four hours later, bleeding recurred, and CTA was repeated after the oral cavity was packed. Imaging revealed an unchanged right tonsillar abscess with a tiny focus of contrast extravasation on the arterial phase and pooling on the venous phase, all suggestive of small active bleeding. The decision was to re-attempt embolization and the interventional radiology team was able to successfully embolize the tonsillar branch of the lingual artery (Figure 2a and b).
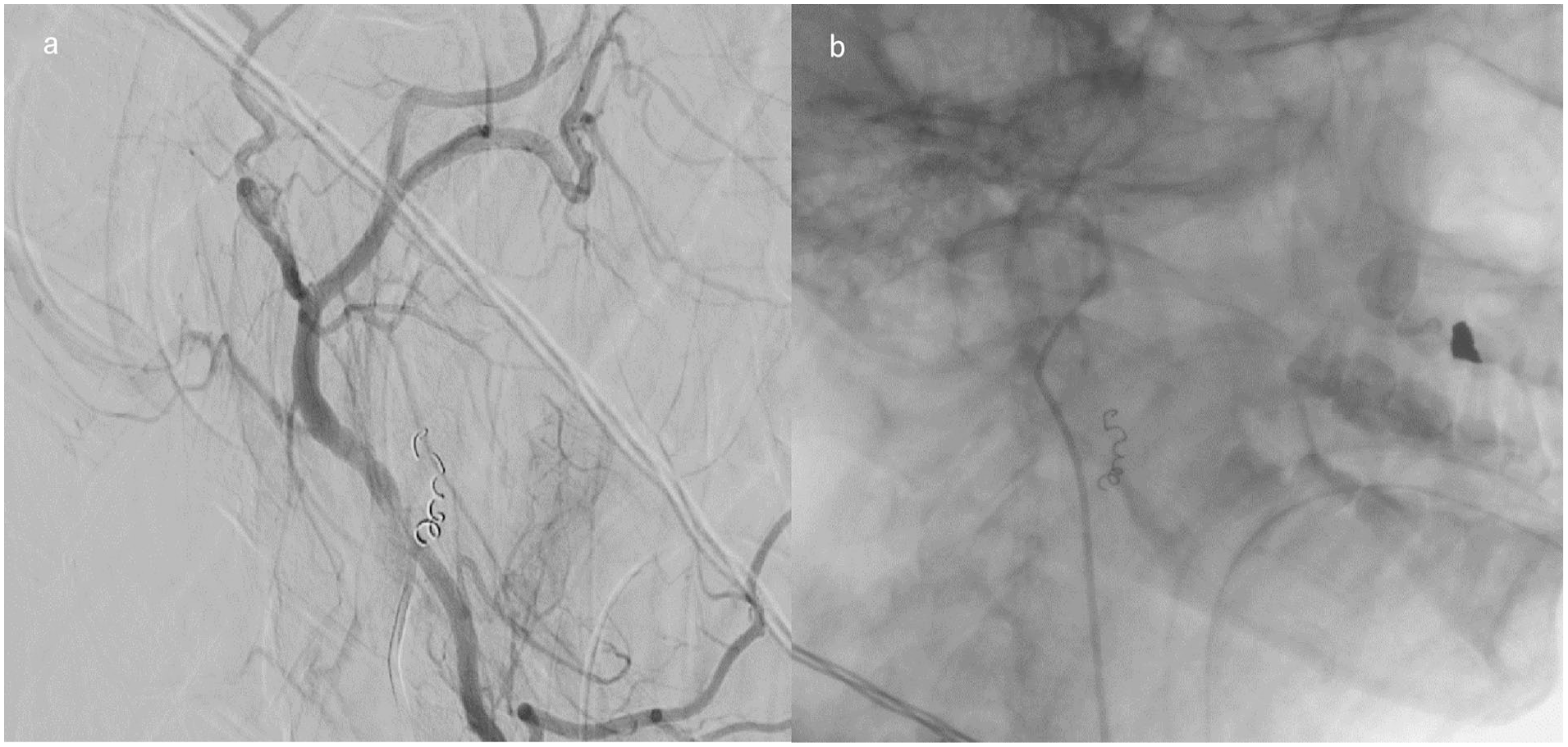
(a) Intraoperative image during embolization shows coil insertion within the tonsillar branch of the lingual artery and (b) postoperative X-ray image shows the final outcome and position of the coil.
Following embolization, the patient did not report any bleeding episodes and was successfully extubated 24 hours later. She then completed courses of intravenous antibiotics for a total of 14 days and was discharged home.
Discussion
SOH is a relatively uncommon medical emergency that demands prompt evaluation and intervention. It is characterized by bleeding originating from the oropharynx, which includes the tonsils, soft palate, and posterior pharyngeal wall, in the absence of apparent injury or trauma. This condition can be life-threatening if not recognized and managed promptly.
Coagulopathies and hematological disorders are among the few etiological factors responsible for SOH. Patients with underlying pathologies such as von Willebrand’s disease, hemophilia, or thrombocytopenia can present with tonsillar bleeding even without evidence of tonsillitis or peri-tonsillar abscess. 1 Inflammatory and infectious causes can lead to mucosal erosion, compromise vascular integrity, and eventually result in bleeding. Infectious mononucleosis and SARS-COV-2 have been reported to induce spontaneous tonsillar hemorrhage by increasing blood flow to the inflamed tonsils. Subsequent erosion from infection-related ulceration of the engorged tonsils triggers blood extravasation and bleeding.2,3 Rare tumor-like malformations of the tonsils, termed “tonsilla partim pendulans” may predispose to intratonsillar hemorrhage with acute dysphagia due to intraparenchymal inflammation and mechanical stress. 7 In the absence of identifiable infective, traumatic, or intrinsic causes of bleeding, SOH can be labeled as idiopathic. 8
Vascular abnormalities such as arteriovenous malformations, telangiectasias, and PAs may be present within the oropharyngeal mucosa. PAs of the lingual, facial, or tonsillar arteries causing oropharyngeal hemorrhage invariably occur following tonsillectomy. Literature reports only one case of PA causing spontaneous tonsillar bleeding. In 2022, Shafqat et al described the case of a 21-year-old male who presented with acute, large-volume oropharyngeal bleeding, localized to the left palatine tonsil and without any sign or symptom of infection. CTA of the neck revealed a 5-mm focal enhancement in the left palatine tonsil and cerebral angiogram identified a PA of the tonsillar branch of the left facial artery. The bleeding was successfully treated with embolization of the tonsillar and ascending palatine branches of the left facial arteries. 4
PAs of the head and neck region can arise from many etiological factors. Post-surgical alteration in the vascular wall integrity of the oropharyngeal vessels favors the formation of PAs, especially following tonsillectomy. 5 Trauma secondary to high-velocity gunshot wounds, blast injuries, or blunt neck trauma may develop delayed PAs of the lingual, facial, or other branches of the external carotid artery, predisposing to massive bleeding episodes that can be life-threatening. 6 Mycotic PA of the lingual artery has been reported secondary to a complicated parapharyngeal infection with reactive lymphadenitis and abscess formation, highlighting the potential role of infections in the pathophysiology of these vascular abnormalities. 9 The combination of radiotherapy and intra-arterial chemotherapy for advanced tongue or head and neck cancer cooperatively forms PA by the mechanism of vascular microinjury to the arterial wall. 10
This case adds to the literature by describing the second case of spontaneous oropharyngeal bleeding secondary to a PA successfully managed by the embolization of distal branches of the lingual artery.
Footnotes
Authorship Contribution Statement
All authors contributed to the study’s conception and design. Material preparation and data collection were performed by Anne-Marie Daou. The first draft of the manuscript was written by Anne-Marie Daou and Jad Hosri, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The American University of Beirut Institutional Review Board has determined that this is not “Human Subject Research” and hence no ethical approval is required. Therefore, this article does not contain any studies with human participants performed by any of the authors.
Informed Consent
For this type of study, informed consent is not required.
Consent for Publication
Consent for publication was obtained for every individual person’s data included in the study.