
Abstract
This clinical record revisits the classical and pathognomonic features of craniocervical tetanus in a 65-year-old farmer who presented with acute-onset trismus, multiple cranial nerve pareses (III, IX, and X), risus sardonicus, and spasm of the head–neck musculature. This paper explores the relevant literature and presents a brief pictorial analysis of the global epidemiologic data. With most countries successfully adopting the maternal and neonatal tetanus elimination (MNTE) program, the incidence and mortality of tetanus across age groups have sharply reduced in high-income and most middle-income nations. In adults, tetanus is now encountered in specialized situations like waning immunity and incomplete vaccination, in the resource-poor and low-income nations, in countries achieving MNTE recently, and as cluster cases in the aftermath of natural disasters involving human settlements. Therefore, present-day practicing otolaryngologists and residents who have limited exposure to the tell-tale clinical features of craniocervical tetanus should consider it during work-up of acute-onset trismus in adults in susceptible situations and with a conducive background. The clinical spectrum of craniocervical tetanus as depicted in this report, including the demonstration of the pathognomonic positive spatula test, provides valuable learning points for otolaryngologists in this regard.
Keywords
Introduction
Tetanus is a potentially fatal, non-transmissible, neurotoxin-mediated infectious disease that is increasingly becoming uncommon in today’s clinical practice due to strengthened implementation of maternal and neonatal tetanus elimination (MNTE) program across nations. 1 The disease in its different forms has characteristic clinical features and is essentially a clinical diagnosis. The occasional, sporadic events in elderly persons with poor immunity might present with acute-onset trismus as the chief complaint. 2 Considering craniocervical tetanus as a probable differential diagnosis in such situations might be challenging for the present generation otolaryngologists and residents. This is because unfamiliarity with the classical features and the rarity of the disease in contemporary times have increased the threshold of suspicion and put such a diagnosis at a low priority. However, tetanus continues to be a public health problem in many low-income nations and may emerge through cluster cases during the aftermath of natural disasters affecting human habitat.1,3,4 Also, it cannot be eradicated due to the ubiquitous, highly resistant spores. 3 Therefore, it is imperative that the young otolaryngology practitioners and residents be aware of the head–neck presentations of tetanus and consider it as a differential in suitable clinical scenarios. The present illustration re-visits the compelling diagnostic features of craniocervical tetanus that intend to serve as a clinical set-piece experience for them.
Case Report
A 65-year-old farmer from the interior of an Indian village was referred to the Otolaryngology and Head–Neck Surgery department from the peripheral healthcare service for evaluation of inability to fully open his mouth for 3 days. The man appeared emaciated, had poor oro-dental hygiene, with history of tobacco-chewing and smoking since decades. The acute-onset trismus was not preceded by fever or any systemic illness. He was not known to have any comorbidity and had been otherwise active prior to his present illness. He also complained of inability to swallow food, more to liquids, since the same duration he developed the trismus. A non-contrast computed tomogram study of the head–neck region performed at the primary healthcare service prior to the referral did not reveal any mass lesion in the pharynx, oral cavity, and the retromolar trigone areas. The patient denied history of dog-bite, and inadvertent or deliberate ingestion of insecticide or rodenticide.
On careful examination, the patient was noted to have stiffness in his neck resulting in restricted head movements. The diffuse spasm in the neck muscles was evident. He also had the risus sardonicus expression on his face. Within 4 days of the onset of trismus, the patient developed bilateral ptosis. The clinical features are depicted in Figure 1 and Supplemental Video 1. An effort to evaluate the oral cavity and oropharynx with a steel tongue depressor revealed lack of gag reflex and resulted in sudden, painful clenching of the jaws due to spasm of the masseters, suggesting positive spatula test [Supplemental Video 2].

The clinical features of craniocervical tetanus consist of involuntary spasms of the facial and neck muscles, along with cranial nerve pareses. This patient presented with acute-onset trismus (A). There was risus sardonicus expression over his face, and prominent, stiff neck muscles (B and C). He developed bilateral ptosis within 4 days of the onset of trismus (B and C). Note the voluntary contraction of the frontalis (frontal belly of occipitofrontalis muscle), apparent as forehead wrinkling, in an effort to counter the drooping eyelids.
The diagnosis of cervical tetanus progressing to the generalized form was made. At this stage, the patient did not develop respiratory distress, abdominal rigidity, weakness or spasm in the extremities, or other features of generalized tetanus extending below the neck. He could not recollect any recent major trauma. During clinical examination, apart from a dry central perforation in his left ear, no specific wound in the head–neck region could be identified that could be a potential port for contamination by the bacterial spores. However, he had been carrying out his farming activities bare-footed, and his immunization for tetanus was unknown.
In apprehension of the worst, the patient was admitted to the intensive care unit for monitoring and further management. He was administered human tetanus immunoglobulin (500 IU; intramuscular; Tetglob™, Bharat Serums & Vaccines Ltd., Mumbai, India) and tetanus toxoid (0.5 ml; intramuscular; Tetvac™, Serum Institute of India Ltd., Pune, India), apart from antibiotics (intravenous co-amoxyclav and metronidazole) and other supportive measures, including continuous midazolam infusion for muscle relaxation and sedation. A watchful observation was maintained with provision for endotracheal intubation or tracheostomy for a possible respiratory failure. Fortunately, the muscle spasms progressed no further. The patient recuperated over the next 3 weeks without any residual spasm and nerve paresis.
Discussion
Tetanus is a non-contagious, neurotoxin-mediated, vaccine-preventable infectious disease caused by the anerobic gram-positive bacillus Clostridium tetani and is characterized by muscle spasm, multiple cranial nerve pareses, and autonomic disorders.2,3,5 The highly resistant bacterial spores are ubiquitous in the soil, feces, rusted metals, and skin. 5 They enter the human body through surface wounds of varying severity, although a visible tissue breach might not be evident in about 20% of the affected individuals.1,6 The toxins (tetanospasmin, and the poorly understood histolytic—tetanolysin) ascend to the central nervous system from the neuromuscular junction close to the wound through retrograde axonal transport, and reduce the secretion of the inhibitory neurotransmitters (γ-aminobutyric acid, glycine) and block the excitatory synapses.2,3 This results in the characteristic muscle spasms. The reasons for cranial nerve paresis are not fully understood. The four clinical types of tetanus depend upon the predominant presenting features: localized (restricted to injury site), cephalic (cranial nerve pareses following trauma in the head–neck region), generalized (most common type; spasms of the muscles of head–neck, extremities, thorax, and abdomen), and neonatal.2,3,5 The less common cephalic type often progresses to the generalized form, as seen in this patient.
Tetanus is potentially fatal, with a mortality rate of 15%-30% in the cephalic and 10%-70% in the generalized and neonatal types, reaching up to 100% without treatment, and 15%-20% even in the intensive care set-up. 5 Since natural antibody production is negligible due to the minute amount of toxin released, definitive preventive and curative options rest on timely administration of toxoid (inactivated toxins producing active immunity) and immunoglobulin (antibodies producing passive immunity), determined by the previous vaccination status and the nature and severity of injury. Essentially, tetanus is a disease of the resource-poor-, low- and middle-income nations. The efficacy of the dedicated government initiatives to implement vaccination as part of the MNTE program as a long-term strategy to counter adult tetanus and confer lifetime immunity is threatened by poor hygiene and awareness, a large population to cater, insufficient resources, and non-adherence to the periodic booster doses. However, even complete immunization (including the three booster doses within 15 years of age) might not provide lifelong protection due to the unpredictable waning of antitoxin titer with time.3,4 Also, with no herd immunity, a person recovering from tetanus might again contract the disease due to inadequate concentration of natural antitoxins in the body.1,4 Nevertheless, with a 90% global reduction of neonatal death within the period of 1990–2015, and with an 81% reduction of non-neonatal mortality during the same period, tetanus is now rarely encountered in the adult population.1,7,8 Appropriate perinatal care, strict immunization regimen, and advanced healthcare have eliminated this disease from the resource-rich, industrialized nations. The occasional, sporadic events are associated with waning immunity in the elderly and incomplete vaccination. Tetanus, however, continues to be a public health problem in the sub-Saharan Africa and south Asia (which contribute to 82% of new cases) [Figure 2(A)-(C)].7,8 Countries in these regions that achieved MNTE only recently (like India in 2015) 9 might still have sporadic adult cases which go largely unreported. Also, some recent research has highlighted a surge of the disease as cluster cases among the survivors of natural catastrophes like earthquakes and tsunamis that cause mass destruction of human settlements.3,4 For these reasons, today’s clinicians need to keep themselves abreast of the disease and its typical presenting features.

The figure sub-parts provide an overview of the comparative records related to tetanus in the last three decades (1990–2019) in terms of overall mortality (A), age-dependent mortality (B), and new case rate (C) across countries in different economic groups. There has been a drastic reduction in overall mortality throughout the world and especially in lower–middle-income nations (A). This can be attributed to the intensive implementation of the MNTE program and scheduled vaccinations in these countries. Mortality in high-income nations is primarily among the elderly population, who develop waning immunity, are inadequately immunized, or are drug addicts (B; a,b). For example, in the United States, proportional mortality in the last three decades has been consistently the highest in the 70+ year category (B; a), whereas the only death registered in the United Kingdom during this period was also in the 70+ year category (B; b). In contrast, bulk of the deaths is in the under-5 year category in lower–middle-income nations (India, Kenya), although the death rate in this age category has considerably decreased in India compared to that in Kenya (B; c, d). The new case rate (new infection per 100,000) is negligible or absent in high-income nations (C; a). India is fast approaching that target; however, tetanus still continues to be a significant public health concern in sub-Saharan Africa (C; b). The illustrations provide the impression that new cases of tetanus in the adult population are becoming increasingly uncommon, especially in high-income nations and also in those middle-income countries that have strictly adopted the MNTE program and scheduled vaccinations. MNTE, maternal and neonatal tetanus elimination; Kenya and Somalia have been chosen as the representatives of sub-Saharan Africa because Kenya is the latest of the priority countries to achieve MNTE validation in 2018, and Somalia is presently the only country in the world having a new case rate of >10/100,000 population; Data sources: references 7 (open access), and 8; https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups, accessed: March 12, 2023.
For the otolaryngologists, work-up of the common presentations like trismus, spasm of the head–neck musculature, multiple cranial nerve pareses, and a difficult airway under spasm necessitating emergency tracheostomy can be challenging in some given clinical situations, when craniocervical tetanus may need to be considered. It is difficult to maintain a high index of suspicion because the condition is least expected. However, the diagnosis is through development of a characteristic clinical pattern; identifying them in time is both life-saving for the patient and rewarding for the clinician-otolaryngologist.
Acute-onset trismus is often the first presentation of craniocervical tetanus, although the patient under discussion also had dysphagia of simultaneous onset.2,5 His clinical features unleashed in close succession in less than a week before the final diagnosis was made. The incubation period for tetanus (range: 3-21 days; median: 7 days)1,2 could not be established here as there was no definite history of trauma. Also, barring the inactive central perforation, no tissue breach could be detected in the head–neck region facilitating entry of the bacterial spores. The dysphagia in this patient suggested pareses of the IX and X cranial nerves, and bilateral ptosis indicated oculomotor paresis. There was diffuse, visible, sustained spasm of the facial musculature (risus sardonicus), muscles of mastication (trismus), and neck muscles (stiff neck, restricted movements). The positive spatula test as documented here was highly characteristic. Considered 94% sensitive and 100% specific, it is a simple bedside clinical test to diagnose tetanus, although it may be difficult to elicit when trismus is severe.2,10,11 It can be documented as a standalone neurophysiologic test for loss of masseter inhibitory reflex. 11 Associated absence of gag reflex further suggested IX and X cranial nerve involvement. The facial nerve—the most common cranial nerve involved2,3—was unaffected in this patient.
Work-up of acute-onset trismus in an elderly patient with long-standing addiction to tobacco could prompt unsuspecting otolaryngologists to exclude oropharyngeal malignancy. Temporomandibular joint pathology, the acute dystonia spectrum, rabies, strychnine poisoning (rodenticide ingestion), and neuromuscular disorders with descending paralysis (reverse Guillain Barré syndrome, Miller Fisher syndrome, myasthenia gravis, etc.) constitute the range of differential diagnoses. The clinical evidence in this patient, however, strongly pointed to craniocervical tetanus—a combination of the cephalic and generalized form, not extending beyond the cervical area. It is one of the uncommon variants of tetanus (about 3% of all cases). 12 The craniocervical features here corroborated to the case definition of non-neonatal tetanus propounded by the World Health Organization and was of grade 2 (moderate) severity following the Ablett classification [Table 1].1,5,13
The Spectrum of the Clinical Features of Tetanus is Enumerated Through the World Health Organization Case Definition of Non-neonatal Tetanus and the Ablett Classification of Severity of the Symptoms.
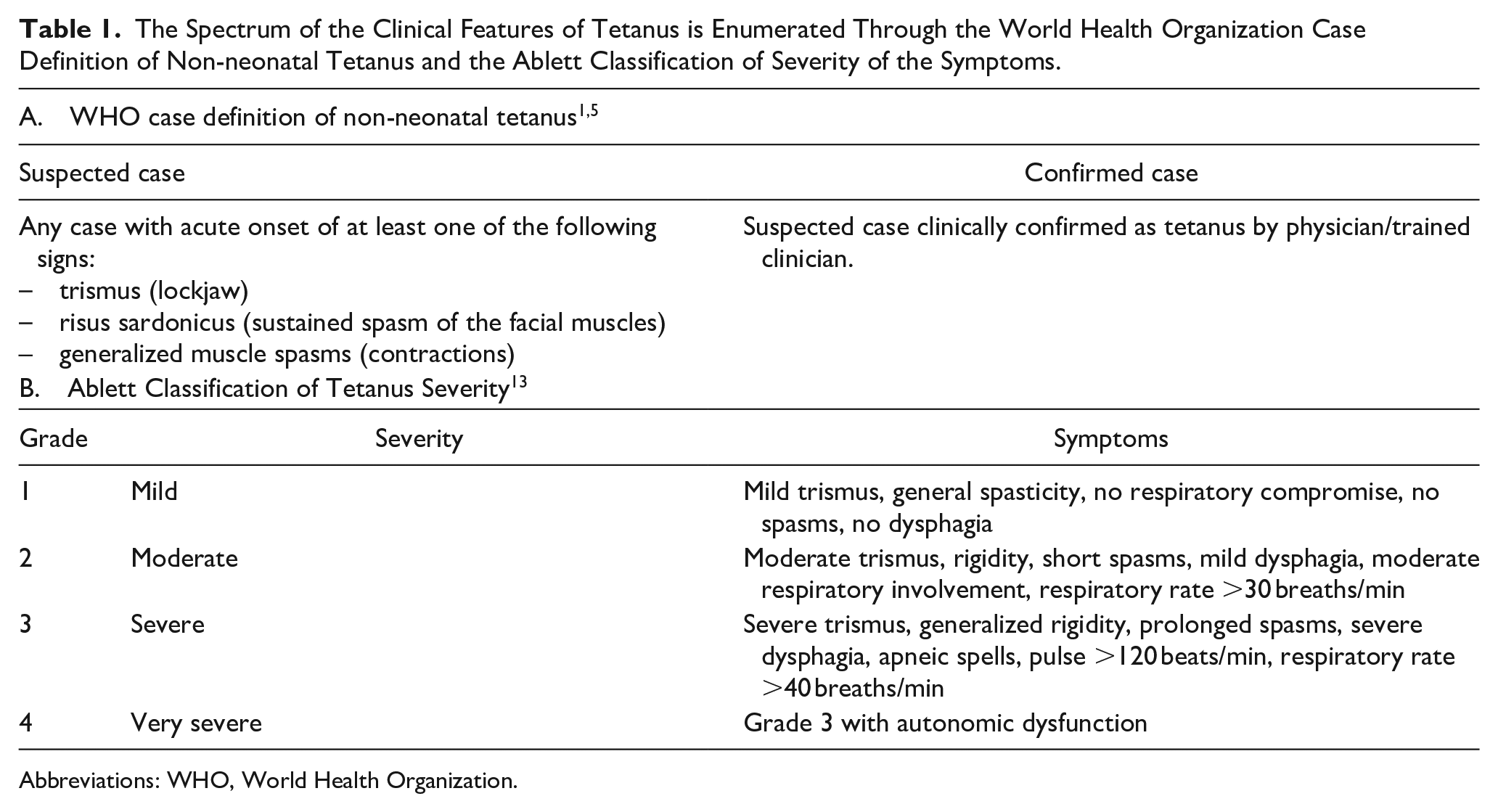
Abbreviations: WHO, World Health Organization.
Conclusion
Craniocervical tetanus is becoming an increasingly uncommon clinical event in the era of immunization, especially in the high- and middle-income group nations. However, its classic clinical manifestations are pathognomonic and diagnostic. These should be identified at the earliest for prompt administration of toxoid and/or immunoglobulin as part of the life-saving treatment protocol. This clinical piece revisits this unusual disease of the 21st century with florid clinical presentations in an elderly man. This will help the residents get familiar with the clinical features, and, in the future course of their career, save lives, if they decide to participate in philanthropic rescue activities during cluster break-outs following natural disasters.
Footnotes
Authors’ Note
Mainak Dutta is now affiliated to Department of Otorhinolaryngology and Head-Neck Surgery, All India Institute of Medical Sciences, Kalyani, West Bengal, India..
Data Availability Statement
All the relevant clinical data are available to us and can be reproduced on request. Please note that the manuscript contains two clinical videos that have been uploaded as ![]() (for online publication only). We request that the videos be made available to the reviewers. The high-resolution version of the videos can be reproduced on demand.
(for online publication only). We request that the videos be made available to the reviewers. The high-resolution version of the videos can be reproduced on demand.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The clinical principles adopted for his management complied with the ethical standards of the relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2013, at Fortaleza, Brazil.
Informed Consent
Written informed consent has been obtained from the patient for the publication of this report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.