
Abstract

Significance Statement
We present a case where exophytic myringosclerosis resembled a tympanic membrane cholesteatoma. We intend to enhance the literature with photo documentation of differing physical exam characteristics of myringosclerosis to increase the diagnostic accuracy. In cases with similar appearances, biopsy may be beneficial in securing a diagnosis without the temporary morbidity associated with complete mass removal and tympanoplasty.
Case
A 9-year-old male was referred to the otolaryngology clinic for a mass on his left tympanic membrane. The patient has a history of recurrent acute otitis media and bilateral tympanostomy tube placement 3 years prior. He has experienced intermittent otorrhea and tinnitus but denied otalgia, hearing loss, or facial weakness. Otoscopy revealed a patent, well-positioned tympanostomy tube on the left with a pearly white, raised, polypoid mass seen just superior to the tube (Figure 1). The posterior–inferior aspect of the tympanic membrane showed classic myringosclerosis. Outside temporal bone computed tomography scan without contrast was suggestive of left-sided tympanic membrane cholesteatoma. Audiogram showed mild conductive hearing loss bilaterally.

Left tympanic membrane with an exophytic, pearly white mass just superior to the tympanostomy tube and classic myringosclerosis in the posterior portion of the tympanic membrane.
The patient was subsequently taken to the operating room for removal of the left tympanic membrane mass and tympanostomy tube as well as left myringoplasty. The mass was isolated to the tympanic membrane and the middle ear appeared normal with no sign of overt involvement by the mass. The mass was removed from the tympanic membrane with no evidence of keratin material. A left-sided myringoplasty was performed utilizing an autologous fat graft. The final pathology of the mass showed fibroconnective tissue with hyalinization and calcification, consistent with the clinical diagnoses of myringosclerosis (Figure 2). The patient recovered well from surgery and postoperative audiogram at 6 months showed a similar mild conductive hearing loss.
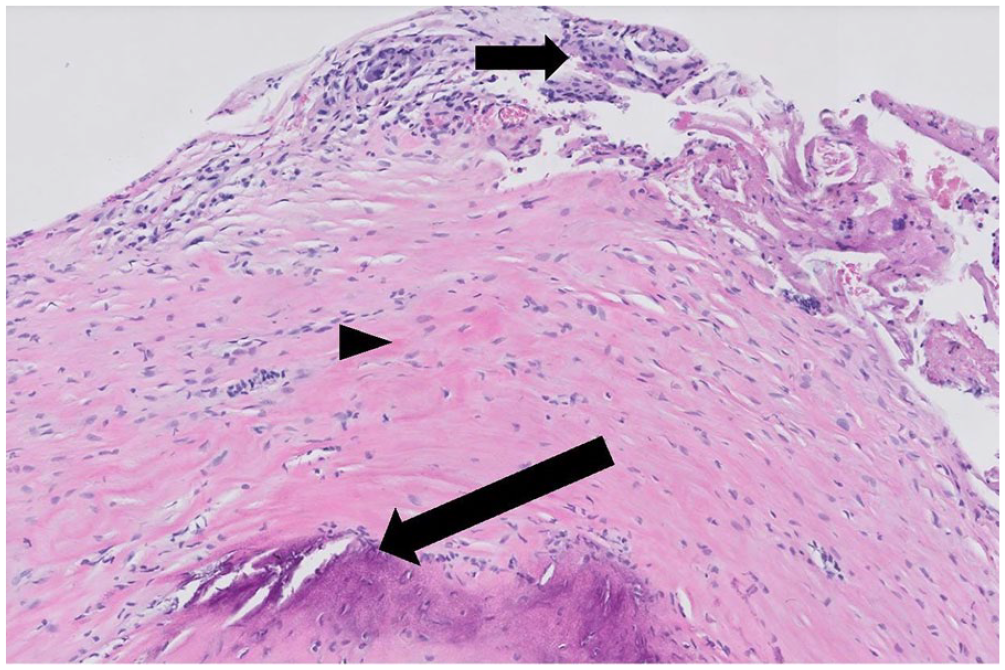
Hyalinized collagen with a lamellar arrangement (arrowhead) and fibrocytes in between collagen fibers with dystrophic calcifications (long arrow), and scant granulation tissue and giant cells at the periphery (short arrow) compatible with the clinical diagnoses of myringosclerosis.
Discussion
Myringosclerosis, a common complication of tympanostomy tube placement, is a type of tympanosclerosis that is isolated to the tympanic membrane without involvement of the middle ear structures. 1 Myringosclerosis occurs due to inflammatory changes within the tympanic membrane secondary to otitis media, tympanostomy tube placement, or other membrane trauma. 2 Specifically, it is characterized by collagen deposition, hyalinization, and calcification beneath the epithelium. 3 Pathogenesis has been theorized to result from inflammatory changes inducing macrophage expression in the tympanic membrane. 4 Classically, these present as flat, white plaques that are contained within the tympanic membrane. 5 Tympanosclerosis includes myringosclerosis that involves the middle ear structures. Therefore, when tympanic membrane lesions arise it is imperative to obtain an accurate diagnosis for appropriate treatment. 6 Topical doxycycline prophylaxis has been shown to have a preventative role in tympanosclerosis formation in animal models; however, this therapy is not utilized in humans. 7
Other common tympanic membrane masses include cholesteatomas. Cholesteatomas can be either congenital or acquired.8,9 Cholesteatomas commonly arise in the middle ear space and can be undetectable on physical exam in as high as 40% of cases. 10 However, some cases can expand to involve the tympanic membrane causing it to bulge out and even rupture. 11 Eventually, if it goes undetected it can lead to recurrent infections, hearing loss, cranial nerve palsies, vertigo, and brain abscess. 12 Tympanosclerosis is a clinical diagnosis and typically does not require surgical intervention unless there is hearing loss noted.13,14 Cholesteatomas on the other hand are typically treated with surgical resection due to its indolent nature and ability to erode the surrounding structures. 15 It is important to note that there is not a strong association between tympanosclerosis and cholesteatoma, and their existence together is uncommon. 16 If the patient has tympanosclerosis and is asymptomatic, surgery should be avoided due to risk of complications. 17
Although clinical suspicion for tympanic cholesteatoma should remain high, this case highlights the alternate appearance of myringosclerosis. There are rare reports of atypical appearing myringosclerosis mimicking tympanic membrane cholesteatoma due to a polypoid, raised appearance; however, this case highlights the varying presentations of myringosclerosis and is unique among the current cases reported in the literature. 18 In this patient, there were 2 discrete appearances of myringosclerosis within the same tympanic membrane: one with a classic flat, white, plaque-like appearance and one with a polypoid, exophytic, pearly white appearance that mimicked a tympanic cholesteatoma. Our aim is to add photo documentation to the current literature on the spectrum of physical exam characteristics of myringosclerosis to assist in increasing diagnostic accuracy. Given the indolent and erosive nature of tympanic cholesteatomas, it is imperative to rule this diagnosis out in any mass with similar appearance. In asymptomatic cases with similar appearances, biopsy may be beneficial in securing a diagnosis without the temporary morbidity associated with complete mass removal and tympanoplasty. 19
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.