
Abstract
Introduction
Paragangliomas, including glomus tympanicum, glomus jugulare, glomus vagale, and carotid body tumors, account for 0.6% of all head-and-neck tumors. Glomus tympanicum tumors arising from the paraganglions are the most common primary neoplasms of the middle ear, 1 but they are generally benign, thus exhibiting local invasion of the middle ear and mastoid without involvement of the jugular bulb. 2 The risk of surgical morbidity is high given the extensive capillary networks and the proximity of the Jacobson nerve (the tympanic branch of nerve IX) and the Arnold nerve (the auricular branch of nerve X). Tumor removal is technically challenging. Such tumors grow slowly but adhere to surrounding structures. Most patients are middle-aged women who are often diagnosed late when they complain of pulsatile tinnitus, hearing loss, and earache (depending on the size of the tumor). Some present with bleeding from the ear. Fewer than 5% of patients have multifocal tumors, and even fewer evidence secretions or metastasis. 3
High-resolution computed tomography (HRCT) of the temporal bone is our preferred modality when locating and diagnosing a tumor. 4 Tympanic tumors are characterized by air or bone between the tumor and the jugular bulb. Continued tumor growth can be problematic given the proximity of the tumor to the cochlea, the facial nerve, the jugular vein, the cranial nerves, the ossicular chain, and the carotid artery; follow-up alone is inadequate. The optimal treatments for advanced glomus tympanicum tumors (Glasscock–Jackson Grades III and IV) are controversial. These tumors lie in critical anatomical locations and have abundant blood supplies, rendering surgical resection complex, associated with a serious risk of complications. Intensity-modulated or fractionated stereotactic radiotherapy is an alternative. In contrast, if patients with early-stage tumors lack any contraindication for general anesthesia, surgery is preferred; this allows total or near-total tumor removal. The tumor’s size and extent dictate the surgical procedure; most surgeries feature a postauricular or a transcanal approach.5-7
With the introduction of endoscopy in the field of ear surgery, more and more procedures are being performed with endoscopes because it can reduce the operative time, afford wider visualization of the surgical field and higher amplification without a loss of resolution, and is associated with fewer incisions and soft tissue dissections and less postoperative morbidity. 8 If the naked eye perceives gross total resection, relapse seems unlikely. However, grinding of bone underwater to remove blood from the operative area is more difficult during endoscopic than conventional surgery.
Of patients with early-stage glomus tympanicum tumors, studies have confirmed the safety and effectiveness of the transcanal endoscopic approach.9-23 Additional high-quality comparative studies are required to explore whether endoscopic ear surgery (EES) is inferior to microscopic ear surgery (MES). Here, we retrospectively compared the operative times, outcomes, relapse rates, and postoperative symptoms of 25 patients with glomus tympanicum tumors treated either endoscopically or microscopically.
Methods
Patient Selection
We retrospectively analyzed patients with glomus tympanicum tumors treated from June 2003 to November 2021 at the Eye and ENT Hospital of Fudan University, Shanghai, China. This study was approved by the Ethics Committee of the Eye and ENT Hospital, Fudan University (approval number: 2019076). Patients were divided into MES and EES groups. In MES group, patients suspected of possible mastoid invasion underwent canal-wall-up tympanomastoidectomy (CWUT) or canal-wall-down tympanomastoidectomy (CWDT) and others underwent MES via the trans-tympanic bone. Seven patients underwent trans-tympanic bone and nine CWUT or CWDT in the MES group; the EES group contained seven patients. All patients underwent imaging and general examinations before surgery. The inclusion criteria were Glasscock-Jackson Grade I or II glomus tympanicum tumors evident on CT, intraoperative findings and a confirmatory pathological report on the operative specimen. All patients were operated upon under general anesthesia. Surgical success was defined as complete tumor excision. We collected demographic and clinical characteristics, the type of surgery, the surgical approach, perioperative findings, postoperative complications, and outcomes.
Radiological Evaluation
Tumors were detected via HRCT of the temporal bone using a 128-channel multidetector SOMATOM Definition Edge CT Scanner (Siemens Inc., Munich, Germany). A glomus tympanicum tumor was defined as a single, round solid tumor confined to the mesotympanum, with clear boundaries (Figure 1A). Some patients also underwent magnetic resonance imaging (MRI); the tumors evidenced intermediate or hypointense T1 signals (Figure 1B) and hyperintense T2 signals. The “salt-and-pepper” pattern reflecting prominent intra-tumoral flow voids was apparent on T2 sequences and evidenced significant contrast enhancement (Figure 1C and D).
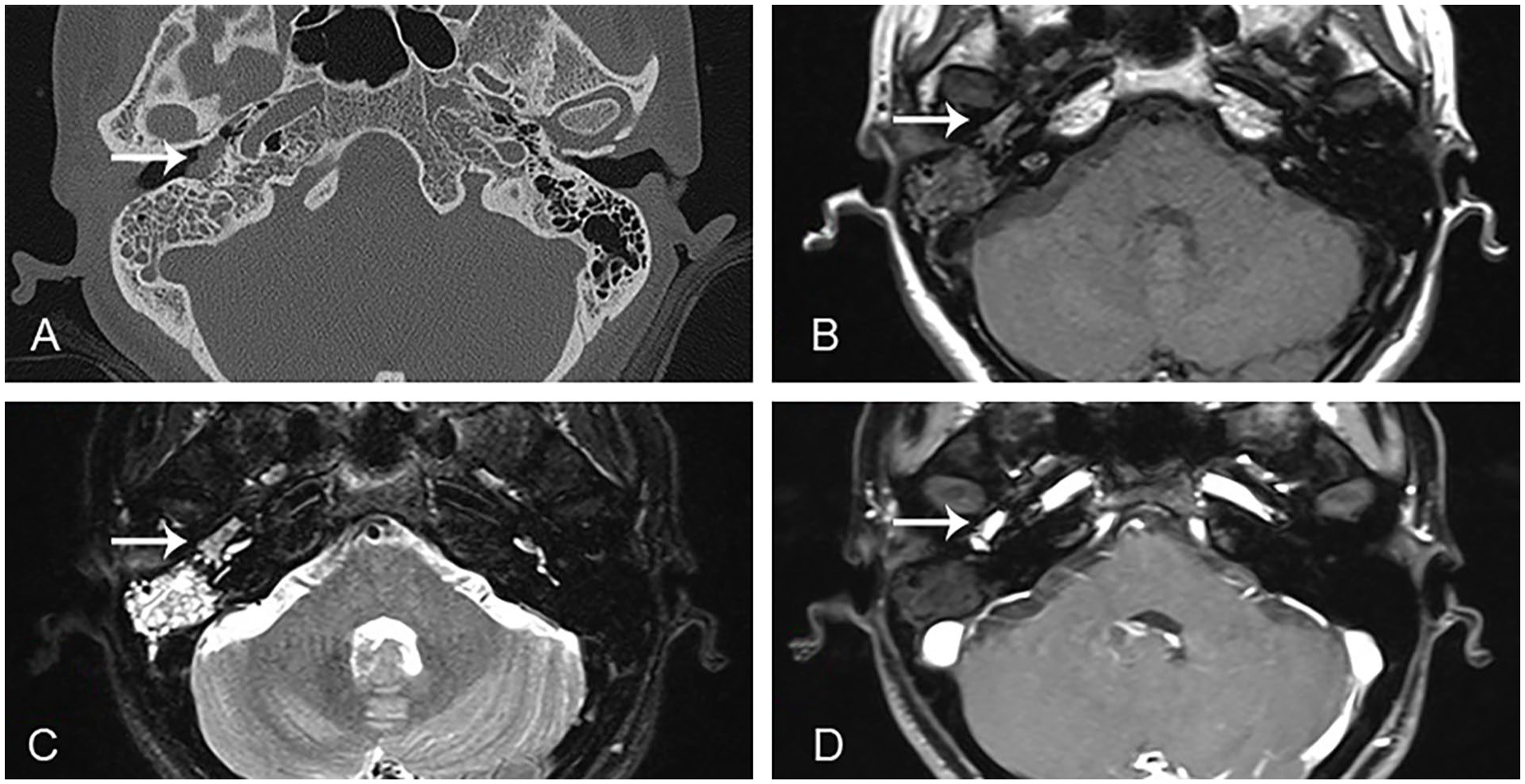
(A) Typical appearance of a glomus tympanicum tumor (white arrow) on HRCT; the tumor presents as a soft tissue mass of uniform density at the surface of the cochlear promontory. Axial T1 (B), T2 (C), and contrast-enhanced T1-weighted (D) MRI scans showing the glomus tympanicum tumor confined to the mesotympanum. HRCT, high-resolution computed tomography; MRI, magnetic resonance imaging.
Surgical Procedures
All surgeries were performed by a single experienced otologist. In the MES group via trans-tympanic bone, an ear canal flap was created to expose the tympanic membrane and surrounding bone. The bony ear canal was enlarged and the inferior tympanum exposed from the enlarged region of the tympanum. The tympanic membrane was lifted and a red mass found in the middle and inferior tympanum. The broad base was located in the promontory tympanum and was connected to the promontory nerve. The mass was completely removed via electrocoagulation at the pedicle. The tympanic membrane was repaired using temporalis muscle fascia and the ear canal flap was restored. As an alternative, traditional CWUT or CWDT was sometimes performed.
In the endoscopic group, an ear canal flap was created to expose the tympanic membrane and surrounding bone. Using an electric drill to grind the bone underwater to enlarge the osseous ear canal, the inferior tympanum was exposed from the enlarged region of the drum bone. An epinephrine-soaked cotton ball was placed to stop bleeding if necessary. The tympanic membrane was lifted and a red mass found in the middle and inferior tympanum. The tumor body was fully exposed, followed by the blood vessels at the root, and an epinephrine tampon employed to pack the blood vessels on the surface of the promontory before blunt dissection of the tumor. The tympanic membrane was repaired using tragus cartilage and the ear canal flap was restored (Figure 2).
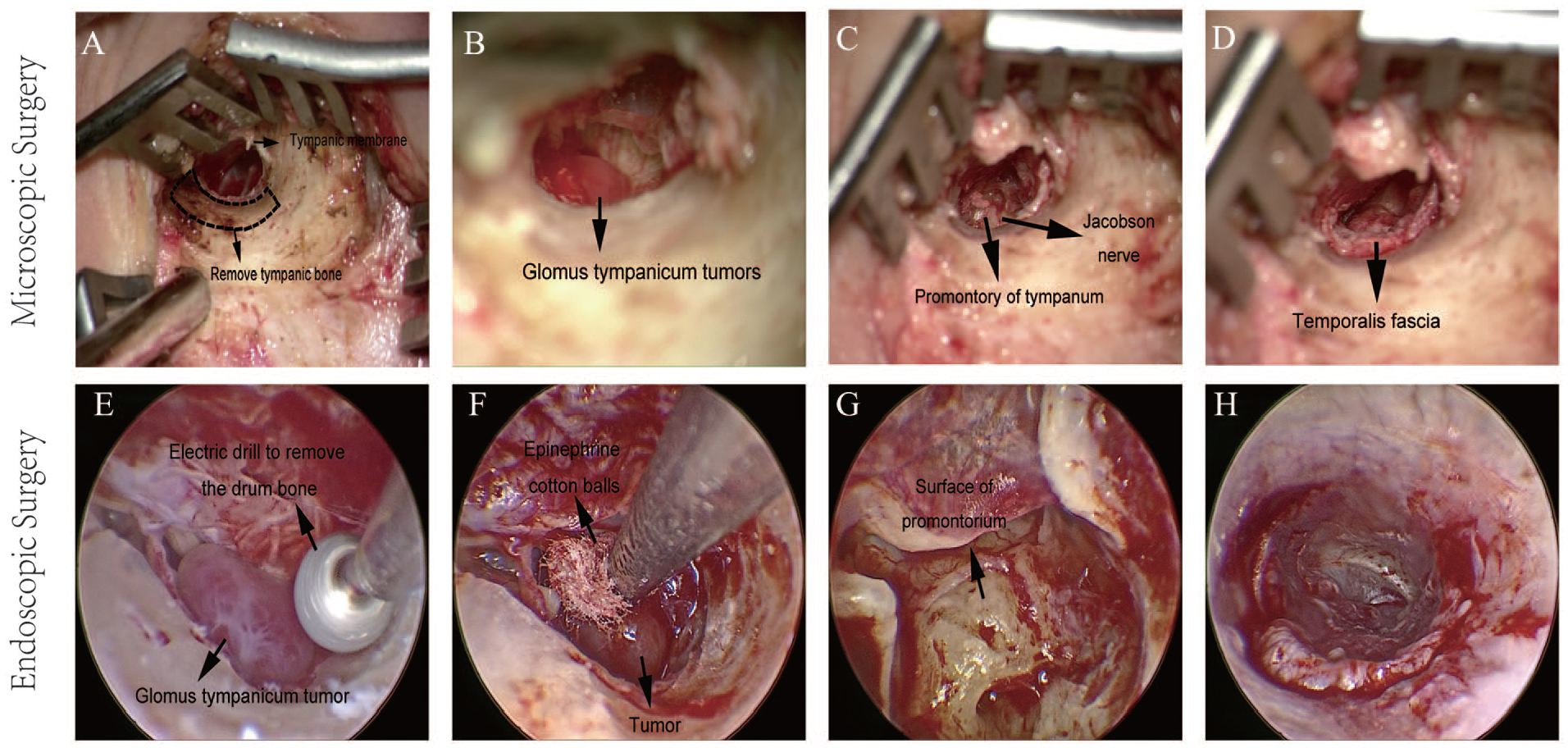
(A) Removal of tympanic bone. (B) The glomus tympanicum tumor. (C) The promontory tympanum. (D) The temporalis fascia. (E) Removal of the drum bone by an electric drill operating underwater. (F) Placement of an epinephrine cotton ball at the root of the vessel prior to blunt dissection of the tumor. (G) The surface of the promontorium after tumor dissection. (H) Repair of the tympanic membrane. MES (A-D), EES (E-H). EES, endoscopic ear surgery; MES, microscopic ear surgery.
Statistical Analysis
Wilcoxon rank-sum tests was used to compared the operation duration, length of hospitalization, cost of hospitalization between the two groups. The Kruskal–Wallis test was used in the comparison of the three groups. We used the Nemenyi test for pairwise comparison. Statistical significance was designated as P < .05 (2-sided) and analyses were conducted in StataMP version 17.0.
Results
Clinical Features
A total of 23 patients were enrolled (16 in the microscopic group and 7 in the endoscopic group); 25 cases are described, including 2 relapses during follow-up. The common symptoms were hearing impairment (64%), pulsatile tinnitus (96%), and ear fullness (52%). We collected postoperative imaging (CT or MRI) data, audiometric data, and clinical signs and symptoms. CT or MRI was re-performed if recurrence was suspected. Medical histories were obtained from patient files and during interviews with the patients (Table 1). The patients ranged in age from 29 to 59 years (mean 43.78 ± 7.0 years in the MES group and 46.9 ± 12.8 years in the EES group). No significant between-group difference in age was apparent (P = .57). The follow-up time was 145.1 ± 48.7 months in the MES group and 20.0 ± 4.4 months in the EES group. There were 3 males and 13 females in the MES group and 7 females in the EES group. In the MES group, 13 patients (72.2%) had Grade I tympanic paragangliomas and 5 (27.8%) had Grade II tympanic paragangliomas; in the EES group, 5 patients (71.4%) had Grade I tympanic paragangliomas and 2 (28.6%) had Grade II tympanic paragangliomas. The grade of tumors showed no difference in three groups (P = .434). In EES group, the maximal linear dimension of the tumor ranged from 3.04 millimeters (mm) to 16.46 mm (mean 9.096 ± 5.334 mm). The dates of surgery ranged from 2019 to 2021 in the EES group; no patient had relapsed by the end of 2022. In the MES group, 12 tumors were on the right and 6 on the left; in the EES group, 2 tumors were on the right and 5 on the left. Neither side was preferred in either the MES or EES group (P = .45 and .45, respectively). In the MES group, 8 cases underwent surgery via the trans-tympanic bone and 10 CWUT or CWDT. Of the 25 cases, 24 presented with pulsatile tinnitus, which was the most common complaint. This was followed by hearing impairment in 12 cases in the MES group and 4 in the EES group. Ear fullness was reported by nine cases in the MES group and four in the EES group. Otorrhea was noted in one EES case and dizziness in one MES case. Earache was present in four MES cases and three EES cases (Table 1).
Characteristics of the Patients in Both Groups.
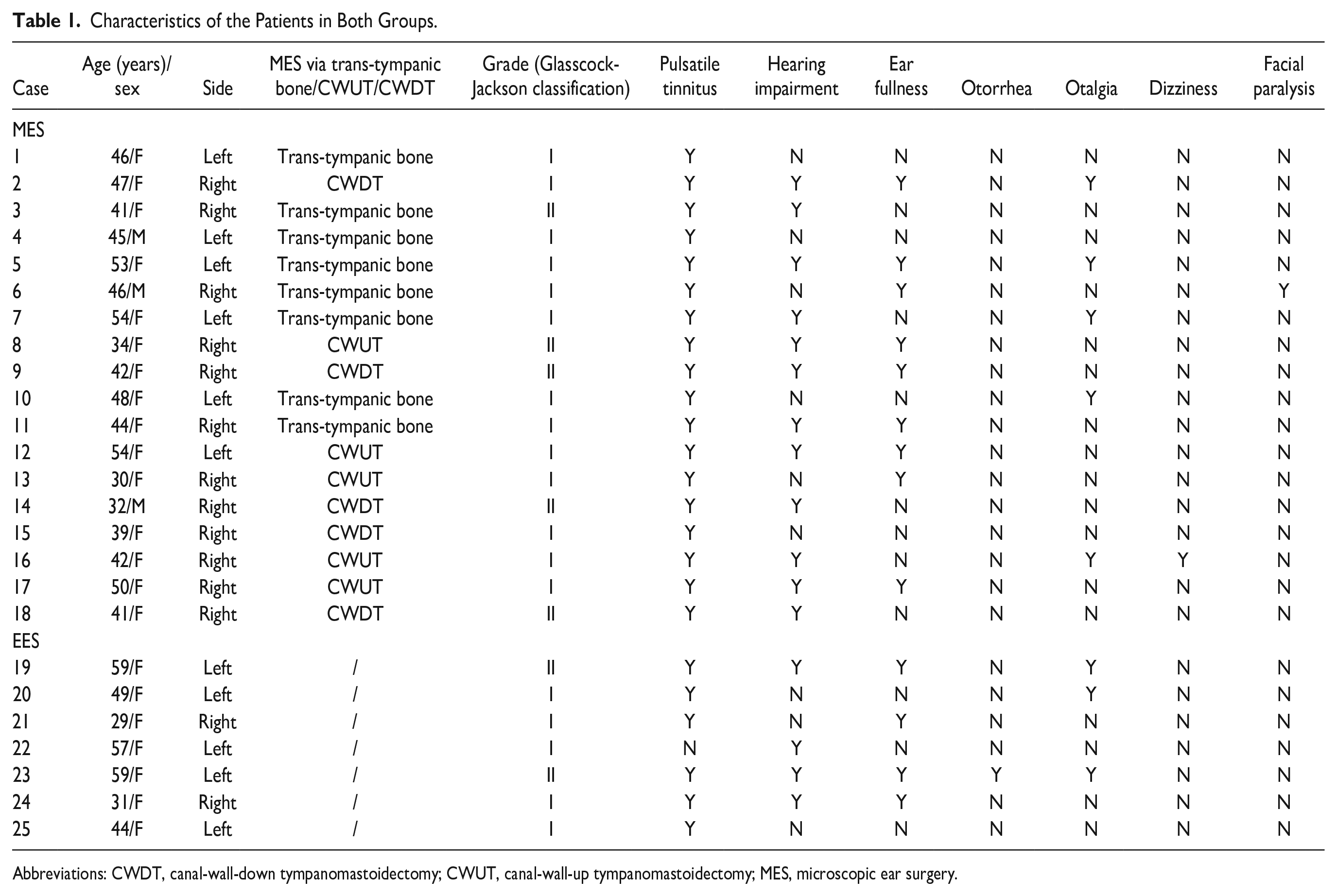
Abbreviations: CWDT, canal-wall-down tympanomastoidectomy; CWUT, canal-wall-up tympanomastoidectomy; MES, microscopic ear surgery.
Surgical Outcomes
The operative time was 109.7 ± 86.3 min (range 40-219 min) in the MES group and 102.1 ± 59.8 min (range 30-172 min) in the EES group (P = .94). In the MES group, the operative time of surgery via the trans-tympanic bone was 65.3 ± 19.9 min and that of CWUT or CWDT 149.2 ± 104.1 min. No statistically significant difference was found among the three groups (P = .07). It worth noting that the duration of EES was getting shorter as the surgeon became more skilled in endoscopy. One patient who underwent CWDT evidenced blood oozing from the dressing during hospitalization; the others lacked postoperative bleeding. The mean length of hospitalization was 5.61 ± 6.01 days in the MES group and 4.1 ± 3.2 days in the EES group (P = .92). When we compared the three groups, it showed a significant difference (P = .01) with 2 ± 0 days after trans-tympanic bone surgery, 8.5 ± 6.9 days after CWUT or CWDT and 4.1 ± 3.2 days in the EES group. The length of hospitalization of MES via trans-tympanic bone surgery is shorter than the group of CWUT or CWDT (P = .006) The costs of hospitalization did not differ between the MES and EES groups and among the three groups (P = .19, P = .35 respectively), being Renminbi (RMB) 12,481.4 ± 4752.9 in the MES group, RMB17,284.2 ± 7002.4 in the EES group, RMB10770.3 ± 1409.1 in MES via the trans-tympanic bone, RMB13392.6 ± 6613.3 in CWDT or CWUT group. Preoperative pure tone average air conduction (PTA AC) of EES group was 36.5 ± 2.1 dB, and pure tone average bone conduction (PTA BC) of EES group was 21.5 ± 9.2 dB. Postoperative PTA AC was 37.5 ± 13.44 dB and PTA BC was 20.0 ± 7.071 dB in EES group. No statistically significant differences were found between preoperative and postoperative PTA AC (P > .9999), PTA BC (P > .9999). It showed a significant difference (P < .0001) of the blood loss among the three groups, with 15.1 ± 2.9 ml, 38.7 ± 4.4 ml, 5.3 ± 1.8 ml of MES via the trans-tympanic bone, CWDT or CWU and EES group, respectively. (Tables 2 and 3)
Outcomes of the MES and EES Groups.
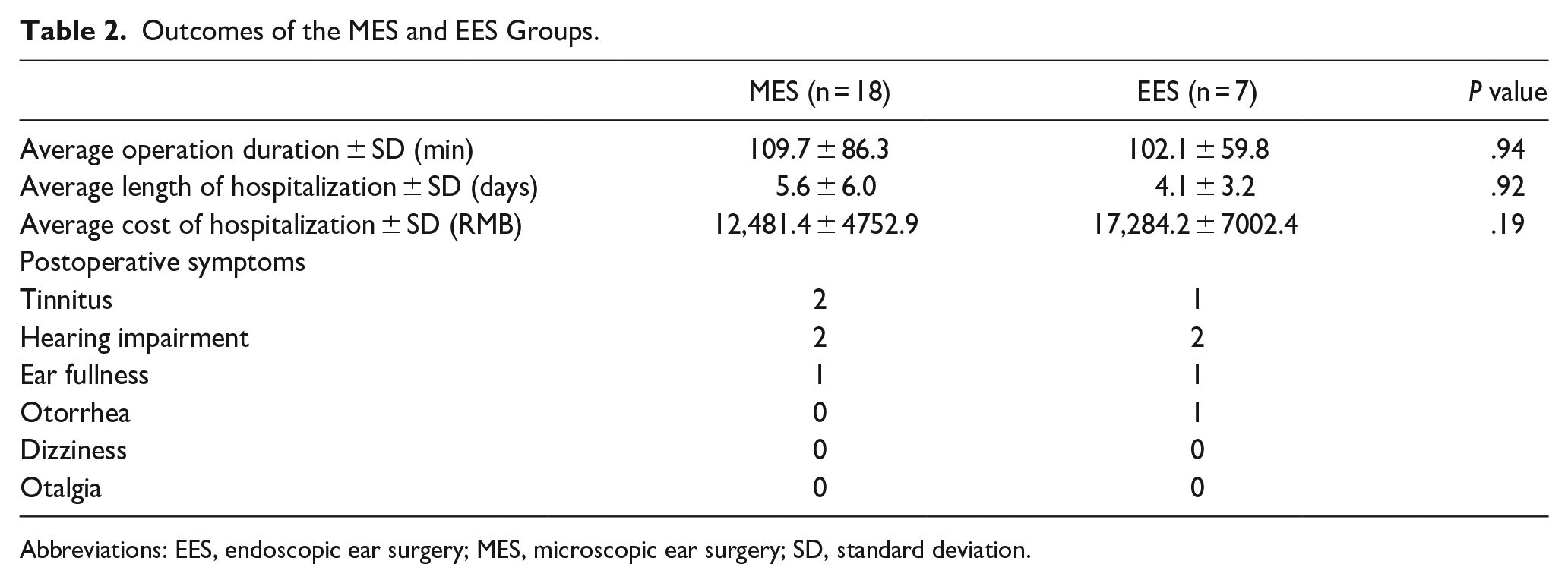
Abbreviations: EES, endoscopic ear surgery; MES, microscopic ear surgery; SD, standard deviation.
Outcomes of the MES Via the Trans-Tympanic Bone, CWDT or CWUT, and EES groups.
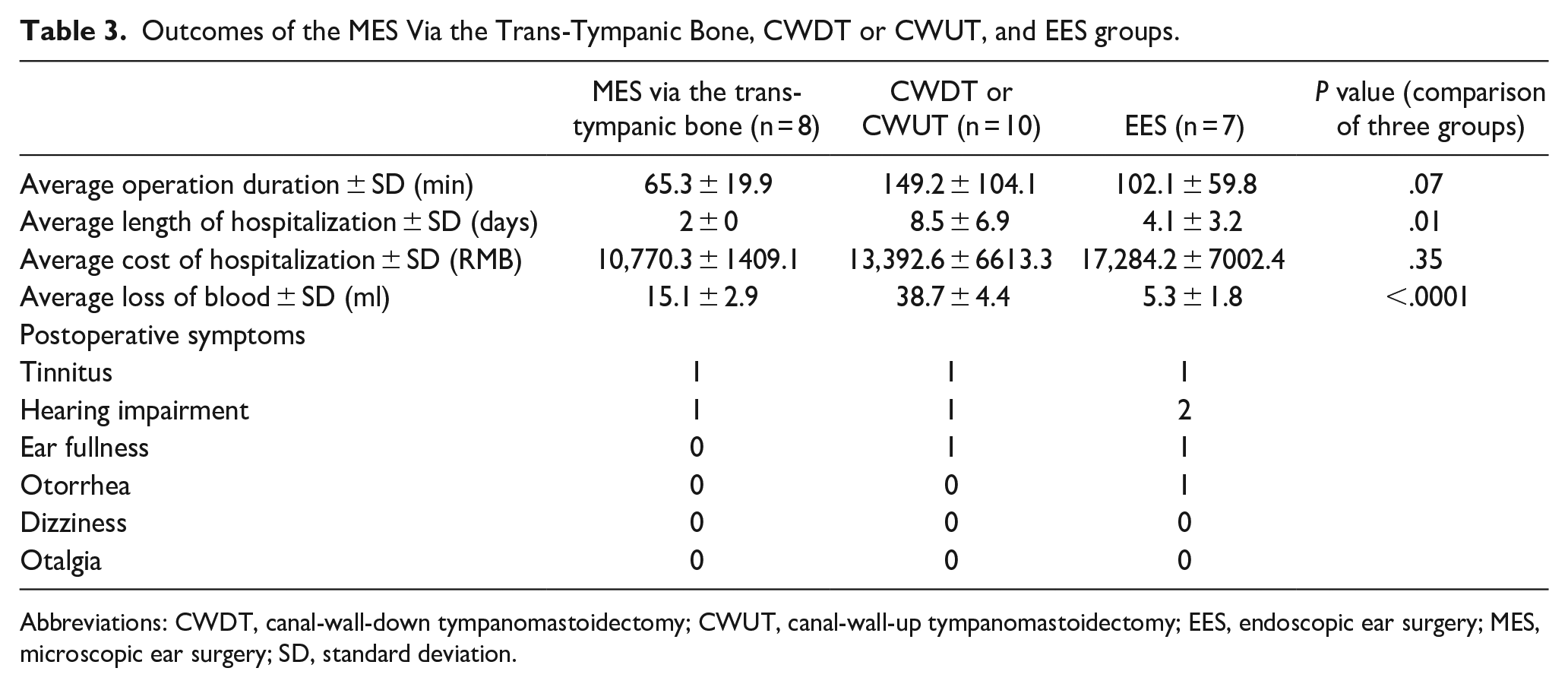
Abbreviations: CWDT, canal-wall-down tympanomastoidectomy; CWUT, canal-wall-up tympanomastoidectomy; EES, endoscopic ear surgery; MES, microscopic ear surgery; SD, standard deviation.
Complications
The pulsatile tinnitus improved in all patients. Two patients in the MES group and three in the EES group still complained about tinnitus in quiet circumstances. In 10 of 12 (83.3%) cases in the MES group and 2 of 4 (50%) cases in the EES group, preoperative hearing was maintained or subjectively improved. Dizziness and otalgia were noted in two cases in the EES group and otorrhea in one case in the EES group. One MES patient who underwent CWDT and one who underwent CWUT relapsed after 8 years (Table 2).
Discussion
Surgical resection is the ideal option for glomus tympanicum tumors which is dictated by the Glasscock-Jackson tumor grade. 24 Grade I tumors are generally removed via transcanal excisions, and most Grade II and Grade III tumors are treated via tympanomastoidectomy with either facial recession or (more recently) hypotympanotomy. CWDT or ear canal overclosure is used to treat Grade IV tumors with large canal defects. 10
In this study, we compared patients with Grade I and Grade II glomus tympanicum tumors. Retroauricular incision via a transcanal tympanotomy approach with or without atticotomy, open cavity mastoidectomy, or hypotympanotomy with tympanomastoidectomy are recognized as appropriate surgical treatments.25,26 Besides, current studies showed the safety and effectiveness of EES.9-23 We chose microscopic surgery in some cases because EES had not been introduced at that time. For the alternative of different procedures of microscopy, CWDT or CWUT underwent in some cases because we expected a larger field of view for surgery before. We retrospectively found that the three surgical ways can be performed in these cases with no involvement of the mastoid, which tied well with previous studies.11,12
Although it is believed that MES affords a good surgical field, bimanual handling, and stereoscopic vision, and it can be mastered by most surgeons, it is difficult to discern the middle ear depth because of poor light; this may prolong the operative time and increase bleeding. 27 As for the two MES procedures in this study, MES via trans-tympanic bone has the advantages of lower trauma and less possibility of cosmetic complications of the incisions because it is not needed postauricular incision. We found a shorter length of hospitalization of the group of MES via trans-tympanic bone, but most of the patients we mentioned were hospitalized for 2 days in the three groups. The mean hospitalization of endoscopic surgery was 4 days, since one patient requested an extended hospitalization to 10 days and one patient’s hospitalization includes holidays resulting in an extension. For CWDT or CWUT group, there were 1 patient with recurrent tympanic body tumor and another patient with secondary surgery after surgery in other hospital. The length of hospital stay was 21 and 14 days, respectively, leading to the extension of hospitalization. It is assumed that endoscopic approach has the advantages of low trauma, a wide surgical field (thus good illumination), shorter focal lengths of observed objects, larger observation angles, good exploration of the area that is “blind” under the microscope including the sinus tympani, facial recess, hypotympanum, and protympanum, and high resolution. 24 We found no significant difference between any of the 2 groups including the duration of the operation, which can be explained for the learning curve as we finished the surgery within 30 min in the subsequent cases. Besides, according to the mean and standard deviation values, the possible longer operation duration of CWUT and CWDT can be explained for the time of tympanomastoidectomy. Comparisons of operation duration may not be a true reflection of reality because of the small number of cases in our study. Compared to other studies,28,29 our duration of endoscopic surgery was longer because we are still on the learning curve; with more experience, the duration of surgery will fall.
Previous studies support the use of trans-tympanic bone approach with microscope2,30,31 and EES9-23 in the early-stage glomus tympanicum tumors. Medina et al 31 showed excellent hearing outcomes and a complete tumor removal among 34 patients using the transcanal approach with microscopy. Kaul et al 15 reported that none of 12 patients reported postoperative vertigo, tinnitus, sensorineural hearing loss, or facial or chordatympani nerve injury after endoscopic resection of a glomus tympanicum tumor. The present series are consistent with these studies. Therefore, we believe that EES and trans-tympanic bone surgery afford surgical outcomes as good as those of conventional MES.
Glomus tympanicum tumors are highly vascular so it is important to control the bleeding. When performed EES, the tumor is fully exposed to find the blood vessels supplying the root before excision. We use small epinephrine-soaked cotton balls to bluntly separate the tumor from the blood vessels at the root; we thus stop bleeding during complete tumor removal. The blood lost is less than 10 ml. For MES, if bleeding occurs, it will be easier to stop the bleeding because of the two-handed operation. However, if the endoscopic surgery is well-mastered, stopping the bleeding will not be a problem.
With respect to limitations of this study, we acknowledge the retrospective study, small simple size and the limited follow-up duration in EES group as we report that the recurrence occurred after up to 8 years. Due to the short time since endoscopy was introduced into ear surgery, the current follow-up data are relatively short. Despite the low probability of tumor recurrence, a prolonged period of monitoring is necessary. Furthermore, there is a dearth of postoperative hearing information. Glomus tympanicum tumors are a relatively rare disease, and the cases we reviewed, particularly MES, have been operated a dozen years ago, and a significant number of patients did not report experiencing any hearing loss following the operation, and consequently, did not undergo a postoperative audiogram. The limitations lead us to stress the importance of the postoperative data of PTA and studies recruited more patients are needed. More experience is needed to determine whether endoscopy can be used for advanced glomus tympanicum tumors. More data are needed to weigh the learning curve and technical limitations of endoscopy and the less clear microscopic field of view in the choice of MES via the trans-tympanic bone.
Conclusions
Early-stage (Grade I or II) glomus tympanicum tumors can be removed via MES via the trans-tympanic bone, or EES via the ear canal; these surgeries afford complete resection, a low recurrence rate, minimal patient trauma, and are nearly equal in cost.
Footnotes
Acknowledgements
The authors thank the anesthetists and the nursing team for their cooperation during the surgical procedures. They also thank the audiologist and the radiologists for assistance with the preoperative and postoperative assessments.
Author Contributions
Conceptualization: Xiao Fu, Jingfang Wu, and Wuqing Wang; Data curation: Xiao Fu; Formal analysis: Xiao Fu and Jingfang Wu; Funding acquisition: Fanglu Chi, Yasheng Yuan, and Dongdong Ren; Investigation: Jihan Lyu and Binjun Chen; Methodology: Xiao Fu, Jingfang Wu, Jihan Lyu, and Binjun Chen; Project administration: Dongdong Ren; Resources: Wuqing Wang; Supervision: Dongdong Ren; Visualization: Fanglu Chi and Dongdong Ren; Writing—original draft: Xiao Fu; Writing—review and editing: Yasheng Yuan and Dongdong Ren.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to the privacy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (NSFC; Grant Nos. 82271166, 81970880 to DR, 81970889 to FC); Natural Science Foundation of Shanghai (Grant No. 22ZR1410100 to DR); Shanghai 2020 “Science and Technology Innovation Action Plan”—“One Belt One Road” International Cooperation Project (Grant No. 20410740600 to YY) and Clinical Research Plan of SHDC (Grant No. SHDC2020CR1049B to YY).
Institutional Review Board
This study was approved by the Ethics Committee of the Eye and ENT Hospital, Fudan University (approval number: 2019076) on November 14, 2019.
Informed Consent
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this article.