
Abstract

Significance Statement
This case report discusses a 56-year-old man, who underwent bilateral balloon Eustachian tuboplasty (BET) as a part of his treatment. Unexpectedly, the procedure led to tympanic membrane perforations in 1 ear, emphasizing the need for caution when performing BET in patients with thin tympanic membranes, even when ventilation tubes are in place.
Case Report
A 56-year-old man presented with right otorrhea. Otoscopy revealed a bilateral adhesive otitis media. The right tympanic membrane showed total adhesion and the left tympanic membrane was thinned and retracted (Figure 1). Nasopharyngoscopy revealed a narrowing of both Eustachian tube (ET) orifices. The Valsalva maneuver was implemented, but no movement of the tympanic membrane was identified. Left ventilation tube insertion was performed during outpatient and the right side is scheduled for tympanomastoidectomy (TM) under general anesthesia with bilateral BET. The preoperative temporal bone computed tomography (CT) confirmed that both mastoids were sclerotic. Furthermore, when the patient performed the Valsalva maneuver, both ETs did not open. Therefore, it was decided to perform BET as there was a high possibility that the tympanic membrane would adhere again even after tympanoplasty with mastoidectomy. The patient wanted to have BET performed during surgery under general anesthesia because of the pain that may occur during BET. Consequently, we scheduled BET and TM simultaneously. At the time of hospitalization for surgery, the left ventilation tube was maintained (Figure 2). Right TM and bilateral BET were performed and the bilateral BET was performed as follows. The balloon was inflated twice to a target pressure of 12 bar for 2 min and 12 bar for 1 min on both sides.1,2 On postoperative day 1, the patient complained of aural fullness in the left ear, which was checked and found to be a medium-sized perforation at the anterior part of the tympanic membrane and a small perforation at the posterior part of the tympanic membrane, and the existing ventilation tube was out of place (Figure 3). The extruding ventilation tube was removed and a paper patch was applied to the tympanic membrane. After the paper patch was applied, the patient’s aural fullness improved.

Otoscopy showed a adhesive otitis media.
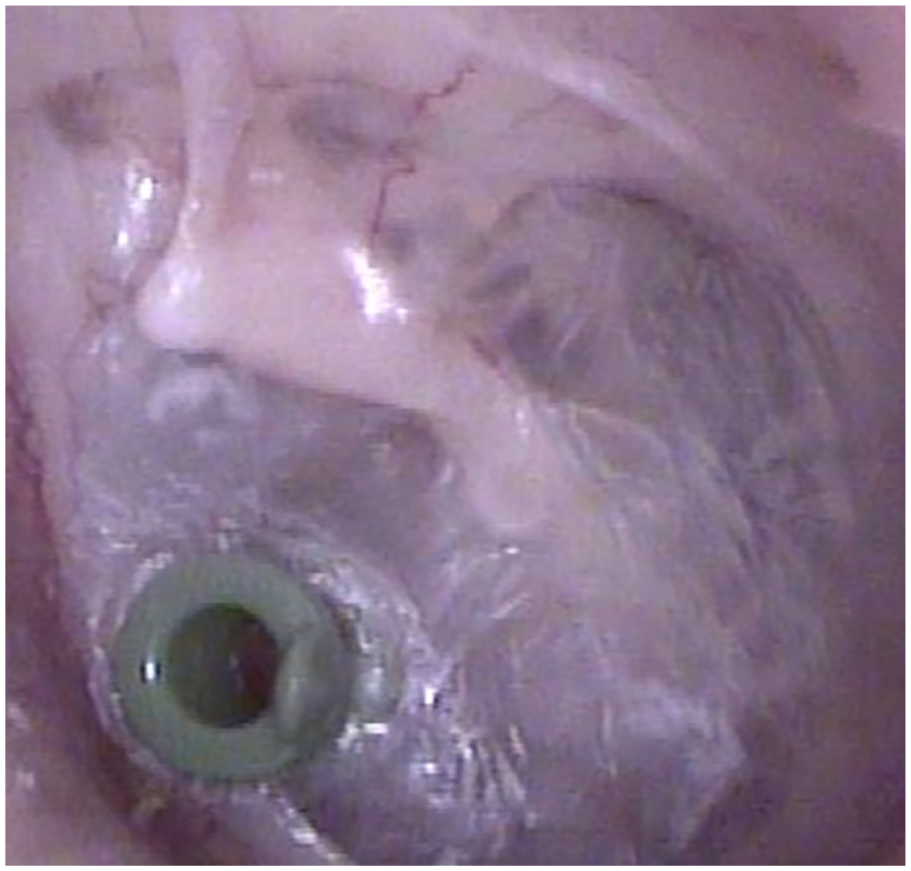
Otoscopy showed a adhesive otitis media after ventilation tube insertion.
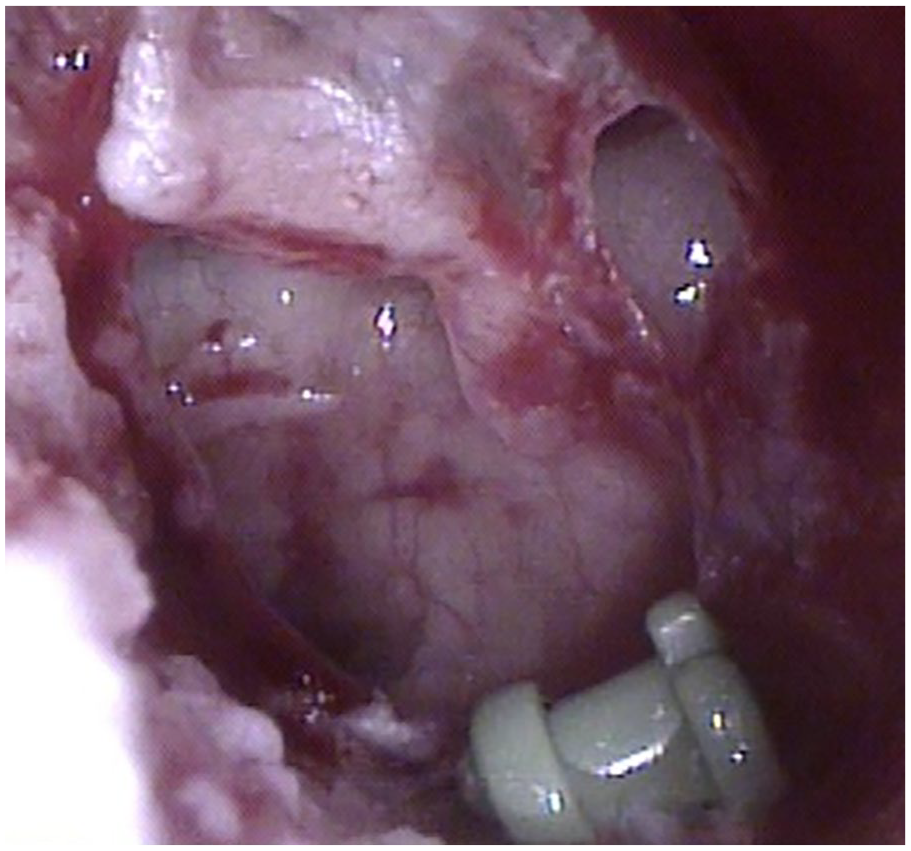
Otoscopy showed a perforation of left tympanic membrane and dislocated ventilation tube after balloon Eustachian tuboplasty.
Complication of BET included minor bleeding, emphysema in the parotid region, hemotympanum, and temporary increase of tinnitus.3,4 The adverse event rate was 3% and these were mostly minor, self-resolving complications.4,5 When ballooning, pressure is transferred through the ET to the middle ear, which can cause damage to the tympanic membrane. The tympanic membrane perforation occurred even though the pressure inside the middle ear was regulated with the outside due to the presence of a ventilation tube. This case report highlights the need for increased caution when performing BET in patients with thin tympanic membranes, as tympanic membrane perforation is possible, even with a ventilation tube in place. Therefore, when performing BET, we must perform it slowly and gently to reduce the risk of tympanic membrane perforation, and we must be more careful in cases where the tympanic membrane is thin.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.