
Abstract

Significance Statement
Traumatic Ulcerative Granuloma with Stromal Eosinophilia (TUGSE) is a rare and benign lesion of the oral mucosa. It is a typically self-limiting disease, requiring minimal intervention. Here we describe the case of a 55-year-old patient who underwent surgical excision of an ulcer on the right lateral tongue for suspicion of malignancy with subsequent pathology results of TUGSE. We then provide a review of the literature on this condition.
Pathology Clinic
A 55-year-old woman presented to the clinic with complaints of a tender ulcer on the right lateral tongue and otalgia in the right ear for the past 4 months. Clinical examination demonstrated a circular ulceration on the right lateral tongue, 10 mm × 10 mm in size. Malignancy was suspected, thus prompting surgical excision of the ulcer. Excision was performed with macroscopically clear margins in the operating room. The specimens were sent for pathological investigation, which demonstrated chronic inflammation with predominantly eosinophils and plasma cells within the subepithelium, consistent with a diagnosis of TUGSE (Figure 1). Syphilis was ruled out via negative Treponema immunohistochemical stain.
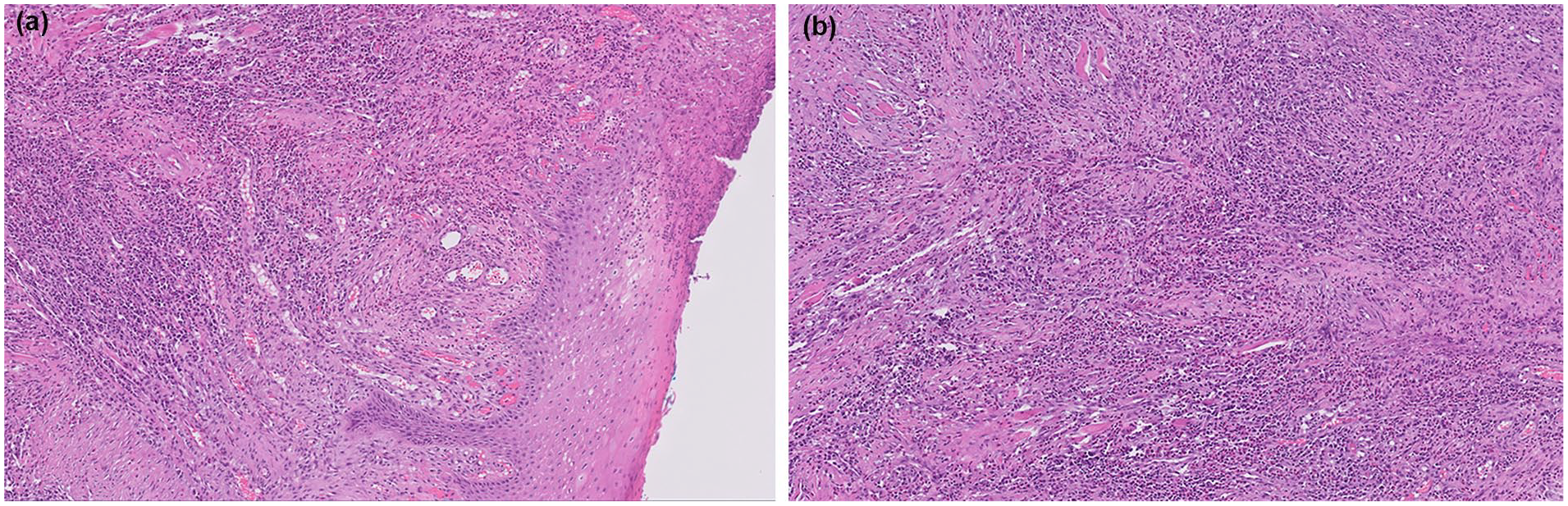
(a) 200× magnification H&E stain: Ulcerated stratified squamous mucosa with a dense lymphoplasmacytic and eosinophilic inflammatory infiltrate. (b) 200× magnification H&E stain: Ulcerated stratified squamous mucosa with a dense lymphoplasmacytic and eosinophilic inflammatory infiltrate.
TUGSE is a rare and benign lesion of the oral mucosa that is characterized by granuloma formation in the submucosa with histiocyte, lymphocyte, and eosinophil infiltration. Gross morphology demonstrates an ulcer with elevated margins and a yellow fibrinous base, typically occurring on the lateral surface of the tongue; however, it can also involve the vestibule, buccal mucosa, and floor of the mouth in other cases. 1
Microscopic characterization of TUGSE demonstrates submucosal invasion with a polymorphic inflammatory infiltrate composed of histiocytes, lymphocytes, large atypical mononuclear cells, plasma cells, and eosinophils 2 (Figure 1). The presence of eosinophils is not completely understood, given that most traumatic oral ulcers are devoid of eosinophils. 1 The current hypothesis is that eosinophils are secondary to mucosal breakdown following trauma. 3 It is also postulated that they have a role in the delayed healing seen in this condition due to the decreased synthesis of transforming growth factor by the eosinophils. 4
The etiology of TUGSE is controversial and not well-understood. As the name suggests, it is believed that trauma is related to the pathogenesis of TUGSE, with factors like sharp tooth margins, dentures, and so on as possible irritants. Some cases have also developed this condition after surgical excision of oral squamous cell carcinomas. 5 Some studies have also shown association with viral agents and bites. 6 Many cases, however, do not demonstrate evidence of trauma, suggesting that there may be other factors contributing to the development of this condition. 7
This condition has a bimodal age of incidence: (1) first 2 years of life and (2) between the 5th and 7th decades. 3 When occurring in infants, TUGSE is classified as Riga-Fede disease and is caused by repetitive trauma from the anterior primary teeth. 8 It has similar histopathological findings as TUGSE in adults.
The lymphocytic infiltrate of TUGSE is primarily composed of B and T lymphocytes. CD3+ and T-cell intracytoplasmic antigen 1+ were noted in most cases. CD68+ cells were also identified, suggesting the presence of macrophages within the infiltrate. Ki-67 can also be identified in 10% to 50% of lymphocytes. 1 CD30+ atypical cells have also been identified in some cases.1,9,10,11 The presence of CD30+ cells warrants inclusion of CD30+ lymphoproliferative disorders within the differential diagnosis.
Diagnosis of TUGSE depends on the biopsy and histopathology results. Differentials for TUGSE include squamous cell carcinoma, infectious causes (primary syphilis, TB, histoplasmosis, etc.), Wegener’s Granulomatosis, sarcoidosis, discoid lupus erythematosus, Langerhans cell histiocytosis, Atypical histiocytic granuloma, CD30+ lymphoproliferative disorders, and malignant lymphoma.1,6 Biopsy of the ulcer was done in this case due to suspected malignancy; thus, cancer is a must-not-miss diagnosis for patients with this condition.
Treatment of TUGSE depends on whether the lesion occurred due to trauma or other causes. In cases of identifiable trauma, the source of irritation should be addressed. After biopsy of the lesion, healing of the ulcer typically ensues, and most cases do not require further treatment. 12 Discomfort experienced by the patient can be managed through corticosteroid or Non-Steroidal Anti-Inflammatory Drug (NSAID) ointments as well as introducing a soft diet. 5 Prognosis for this condition is excellent, and most ulcers resolve on their own.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.