
Abstract
Introduction
Papillary thyroid carcinoma (PTC) is the most common thyroid cancer accounting for 80% to 84% of all thyroid malignancies1,2 and the reported 10-year survival rate is greater than 90%.1,3-5 Central lymph node (CLN) metastasis of PTC occurs in approximately 30% to 64% of cases.6-8 A systematic review identified several clinical features significantly associated with CLN metastasis in PTC, including multifocality, size of primary tumor >2 cm, lymphovascular invasion, and extrathyroidal extension. 5 Total thyroidectomy with prophylactic central neck dissection (CND) significantly decreases the likelihood of locoregional recurrence, but the associated complications include hypoparathyroidism and recurrent laryngeal nerve injury.4,6,9 The indications for CND in PTC have not yet been conclusively established. 8 The American Thyroid Association (ATA) guideline 2015 recommends CND in PTC for T3/T4 tumors or clinically involved lateral neck nodes, or if doing so will positively impact further steps in therapy. 10
The National Comprehensive Cancer Network (NCCN) guideline 2020 recommends CND on the same side as the primary tumor with a modified radical neck dissection performed on clinically involved lateral neck nodes in most cases. 11 The British Thyroid Association 2014 described unclear benefit of CND in high-risk patients, that such decision-making should be personalized, and that bilateral CND was preferred over ipsilateral CND. 12 The European Society of Endocrine Surgeons 2014 recommends CND in patients with high-risk features, such as T3/T4 tumors, extreme age, male gender, bilateral/multifocal tumors, and clinically positive lateral lymph nodes. 13 The ATA guideline 2015 recommends the use of preoperative ultrasound in all patients with PTC. 10 The sensitivity and specificity of ultrasound for detecting CLN metastasis in PTC ranged from 30%-69% to 71%-90%, respectively.11,12 The sensitivity and specificity of ultrasound for detecting lateral lymph node metastasis in PTC ranged from 85%-93% to 65%-80%, respectively.11,12 The positive predictive value (PPV) of ultrasound for detecting CLN metastasis of PTC was 80%, and the PPV of ultrasound for detecting lateral lymph node metastasis of PTC was 85%. 14 To further improve our ability to preoperatively and non-invasively predict the likelihood of CLN metastasis of PTC, the aim of this study was to investigate whether CLN size and characteristics as measured by ultrasound can significantly predict CLN metastasis of PTC.
Material and Methods
This retrospective chart review was conducted at the Department of Otorhinolaryngology of the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. We included patients who were diagnosed PTC and underwent preoperative ultrasound by one experienced otolaryngologist using a LOGIQ S7 Ultrasound Machine with an Expert ML6-15-D Linear Array Transducer (GE Healthcare, Chicago, IL, USA) followed by CND (unilateral or bilateral) during the 2012 to 2019 study period. CLN of any characteristics such as shape (oval or round), internal architecture (presence or loss of fat hilum), cystic change, internal calcification, border (well-defined or irregular), and size detected by ultrasound were included. The size of the central neck node was measured by transverse view of ultrasound. For the round-shaped lymph node, the widest axis was measured and recorded. For the oval-shaped lymph node, the short axis was measured and recorded. An indication for CND in this study was for the central neck node detected by the ultrasound. There was also CND by surgeon’s preference in some patients with size of thyroid mass from preoperative ultrasound equal or greater than 4 cm, positive pathologic lateral lymph nodes by ultrasound, or intraoperative palpable central neck node. Patients who had undergone previous thyroid surgery or radiation were excluded. The Tumor, Node, Metastasis (TNM) staging criteria was used according to 8th edition of the American Joint Committee on Cancer (AJCC) staging manual. We analyzed for correlation between CLN size and characteristics by ultrasound and histopathologic findings among positive CLN patients. The protocol for this study was approved by the Siriraj Institutional Review Board (COA no. Si.634/2018). Written informed consent to participate was not obtained from study subjects due to the retrospective and fully anonymous nature of this study.
Statistical Analysis
Patient characteristics were summarized using descriptive statistics. The results of comparative analyses are given as number and percentage for categorical data, and as mean plus/minus standard deviation for normally distributed continuous data. Chi-square test or Fisher’s exact test was used to compare categorical data, and those results are shown as odds ratio and 95% confidence interval. Student’s t-test was used to compare continuous data. All tests were considered statistically significant at a P-value less than .05. The data were analyzed using SPSS Statistics version 22.0 (SPSS, Inc. Chicago, IL, USA).
Results
There were 165 patients diagnosed with PTC who underwent thyroid surgery. Of those, 15 patients with no preoperative ultrasound and 102 patients with negative central neck node by ultrasound and did not undergo CND were excluded. Among those 102 patients, 8 of them had pathologic lateral lymph nodes. The remaining 48 patients who had preoperative ultrasound and total thyroidectomy with CND were included. Of those, 34 patients had positive identification of the central neck node by ultrasound, and 14 patients had a negative preoperative ultrasound result, but they still underwent CND due to their being determined to be at high risk for CLN metastasis (Figure 1). The reasons for CND in the ultrasound negative group were size of thyroid mass from preoperative ultrasound equal to or greater than 4 cm (1 patient), positive lateral neck node from preoperative ultrasound (7 patients), and intraoperative palpable central neck node (6 patients).
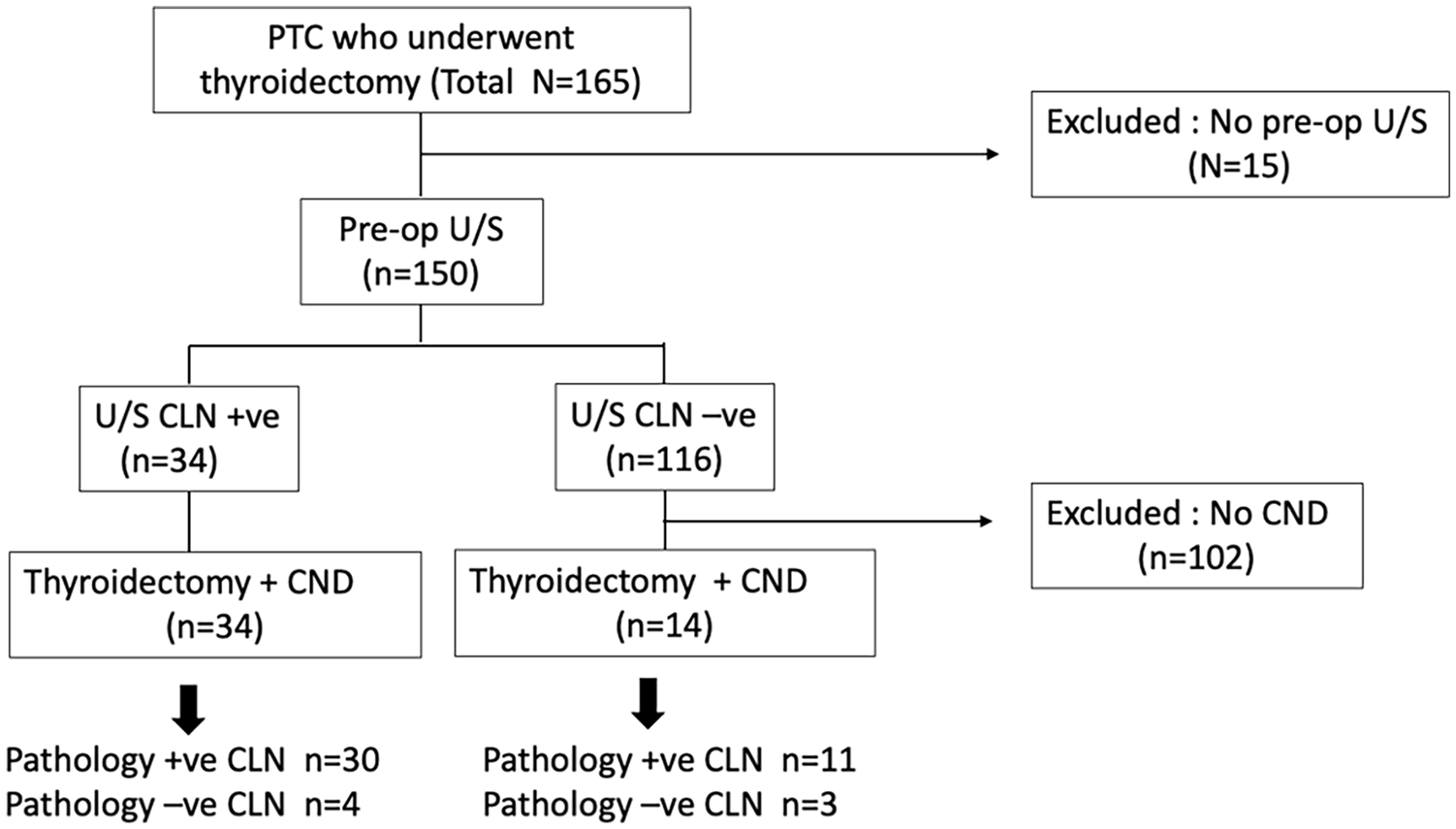
Flow diagram of the patient enrollment protocol.
Patient characteristics consisted of gender, age, number and size of nodules, histology of the lateral neck nodes, and clinical staging (Table 1). The presence of positive lateral nodes was found to be significantly associated with central node metastasis (P = .003).
Demographic and Preoperative Ultrasound Characteristics of Thyroid Nodule, Lateral Neck Node, and Clinical Staging Compared Between the Histology Positive for CLN Group and the Histology Negative for CLN Group (N = 48).
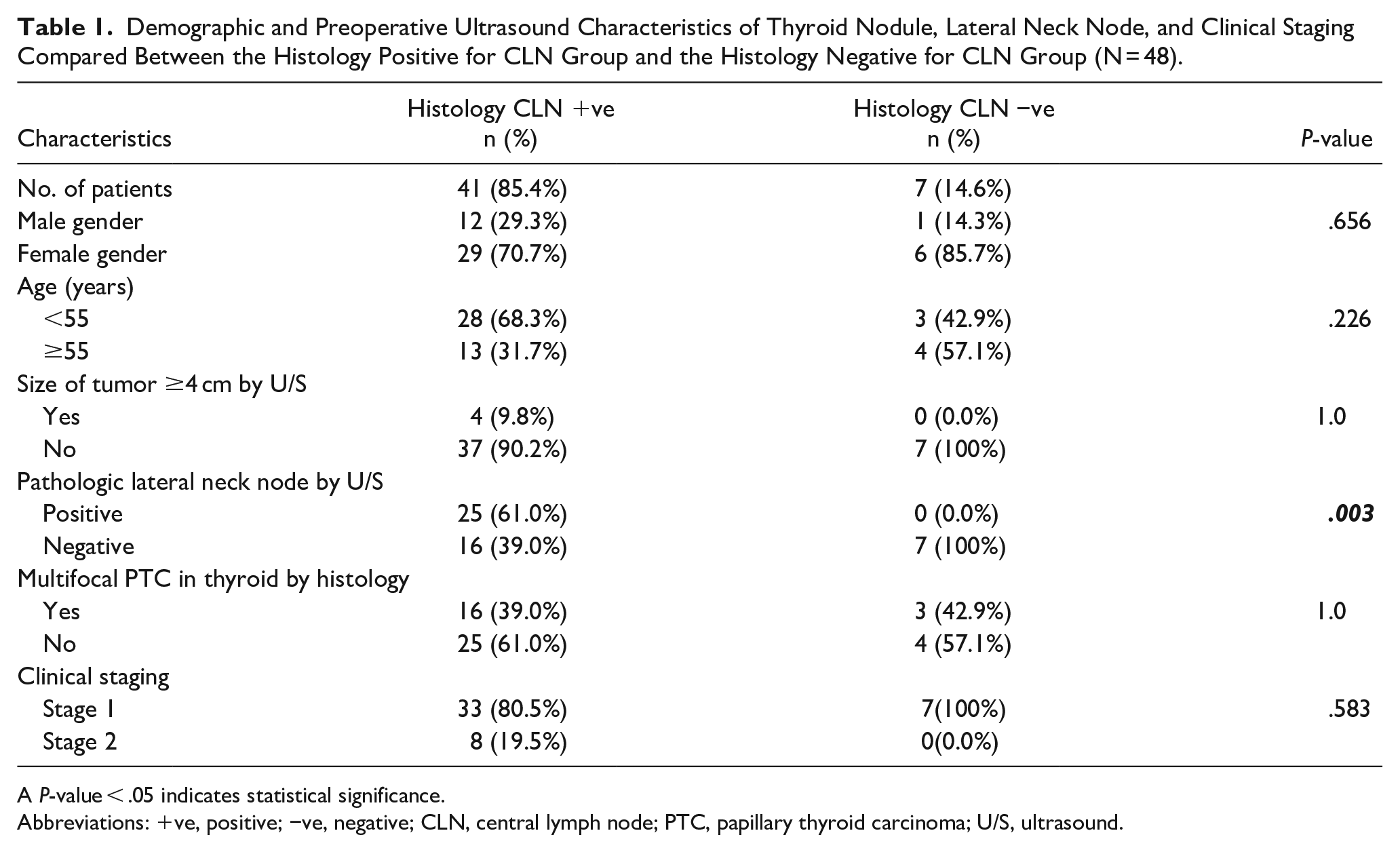
A P-value < .05 indicates statistical significance.
Abbreviations: +ve, positive; −ve, negative; CLN, central lymph node; PTC, papillary thyroid carcinoma; U/S, ultrasound.
Thirty-four patients had positive CLN from ultrasound. The size of CLNs varied from 2 to 44 mm, and the mean size was 8.1 ± 7.2 mm. In 32 cases (94%), the lymph nodes had a well-defined hypoechoic round shape without fat hilum (Figure 2A). One case (3%) had a well-defined hypoechoic oval shape with fat hilum, and histopathology showed no metastasis (Figure 2B). Another case (3%) had a hypoechoic round shape with irregular border and microcalcification, and histopathologic analysis revealed the presence of metastasis. The number of positive cases with more than 1 node was 13/34 (38%). Patients associated with chronic lymphocytic thyroiditis from thyroid histopathology were 9/34 (26%). Histopathologic findings of CLN metastasis relative to ultrasound findings of CLN metastasis is shown in Table 2. Among the 34 patients who had positive CLN from preoperative ultrasound, 30 patients were found to be positive for CLN metastasis by histopathology. The PPV, negative predictive value (NPV), sensitivity, and specificity of ultrasound for detecting CLN metastasis of PTC were 88.2%, 21.4%, 73.2%, and 42.9%, respectively. Of the 30 patients who were positive for CLN metastasis by histology, 29 patients had equal or more number of histological positive nodes as detected by ultrasound, and all of CLN detected by ultrasound were histologically positive. Seven patients had the exact number of histologically positive lymph node as detected by ultrasound, and 22 patients had more histologically positive nodes than those detected by ultrasound. Only 1 patient had less number of nodes positive by histology than an ultrasound. That patient had 1 positive paratracheal lymph node out of 3 lymph nodes detected by ultrasound, of which 2 right paratracheal lymph nodes were histologically negative, whereas only the left paratracheal lymph node was histologically positive. The 3 out of 4 patients with negative CLN metastasis by histology and the 1 patient with less number of positive nodes by histology than by ultrasound were associated with chronic lymphocytic thyroiditis.
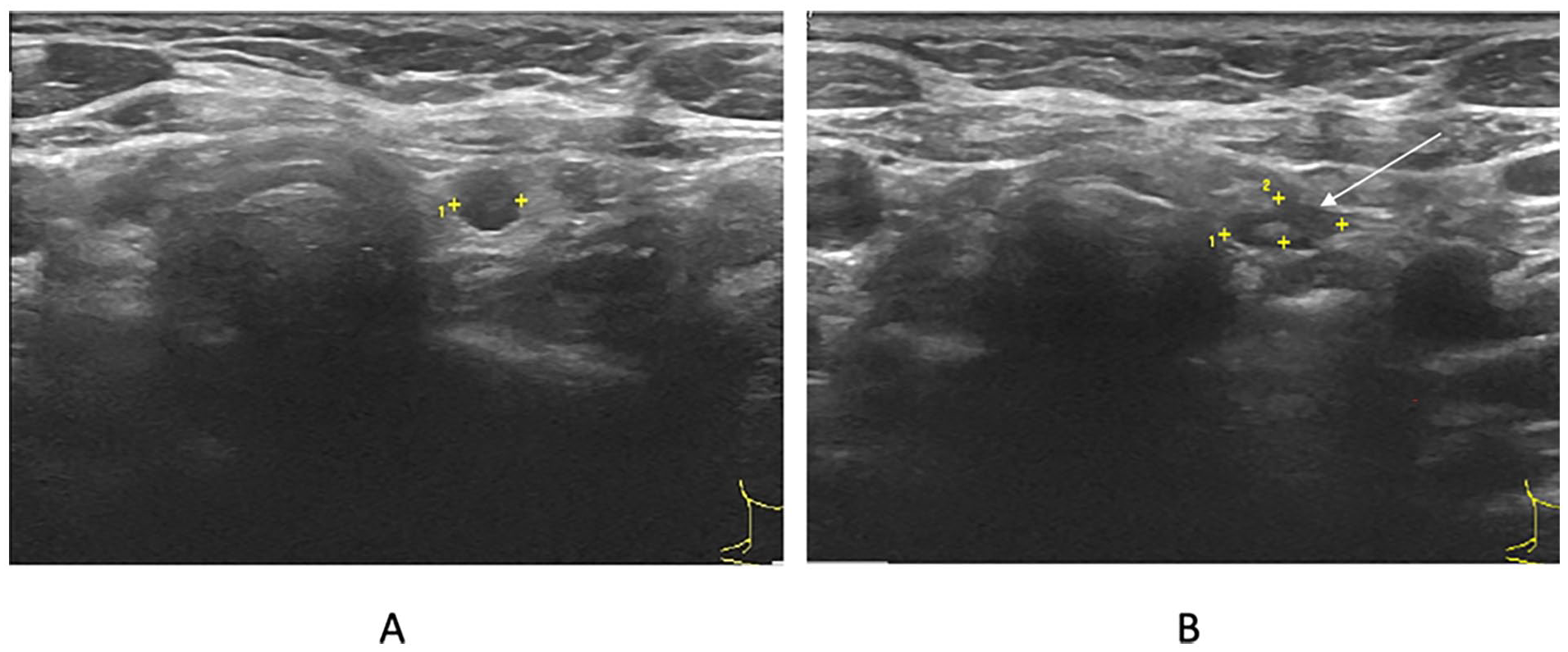
Paratracheal lymph node identified from ultrasound. (A) Round shape without fat hilum. (B) Oval shape with fat hilum (arrow).
Histopathologic Findings of CLN Metastasis Relative to Ultrasound Findings of CLN Metastasis.
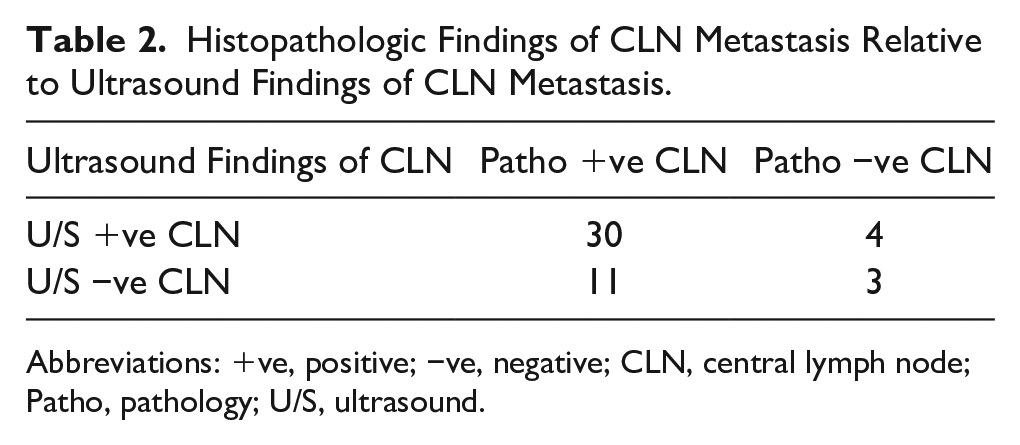
Abbreviations: +ve, positive; −ve, negative; CLN, central lymph node; Patho, pathology; U/S, ultrasound.
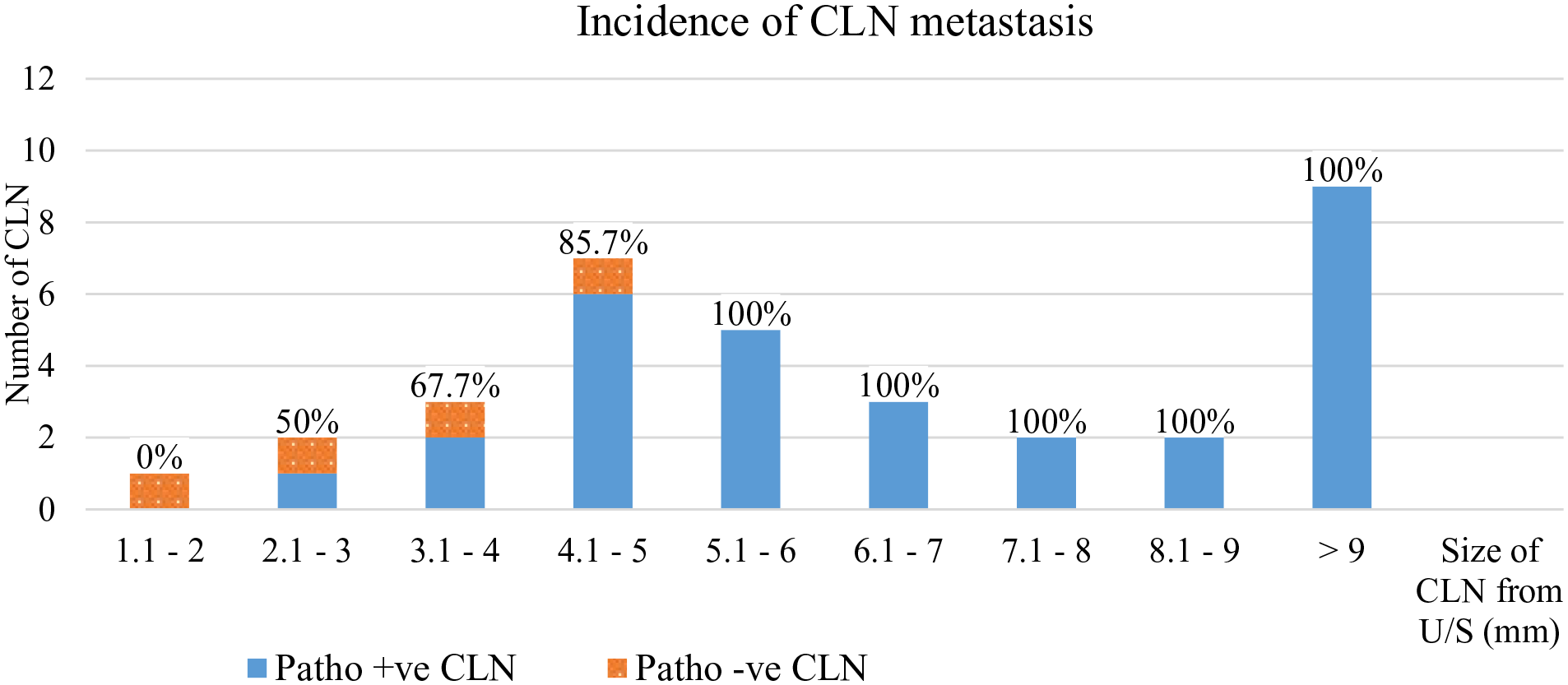
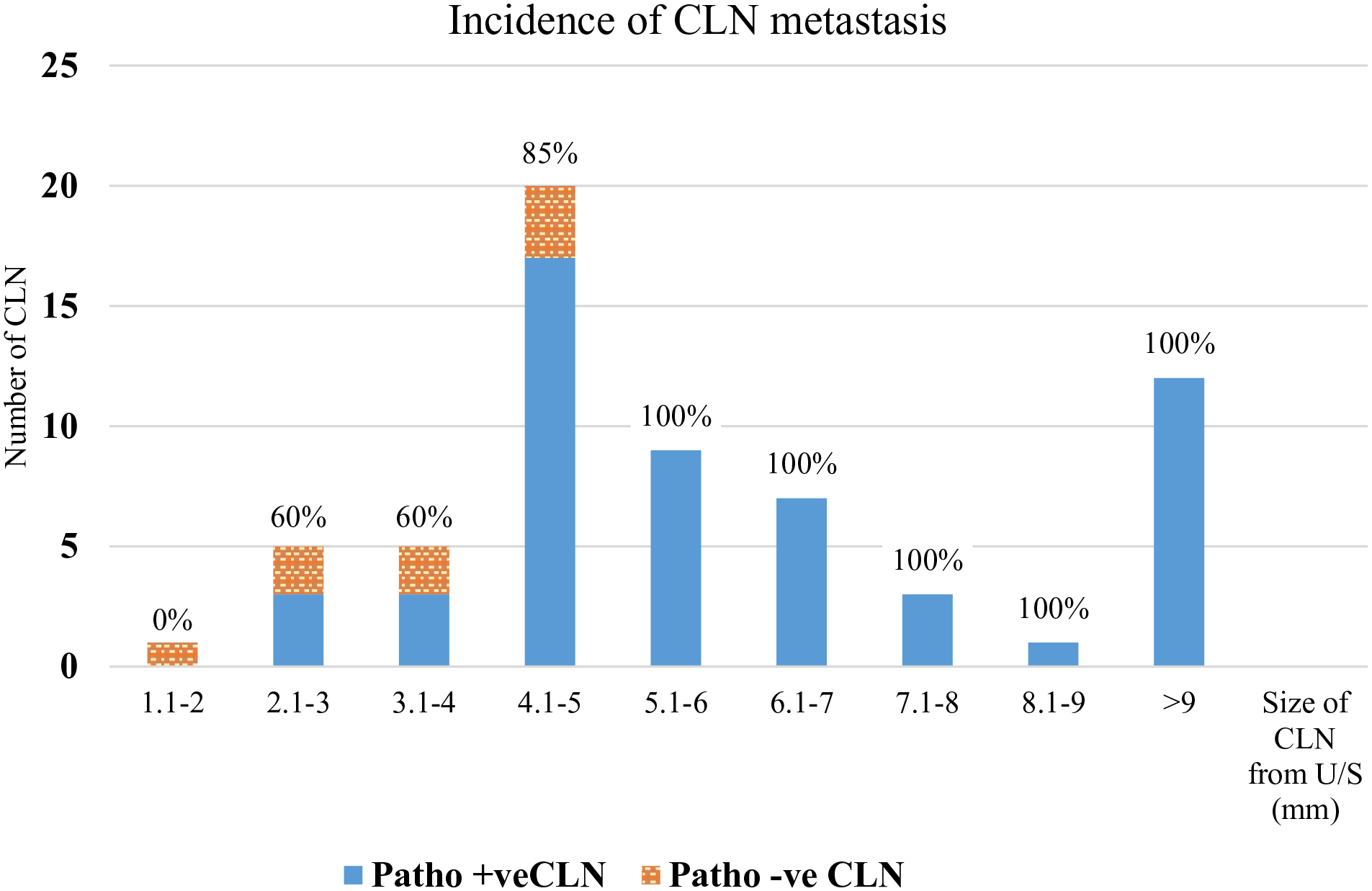
After reviewing the preoperative information of the patients who had positive ultrasound identification of CLN, almost all of the lymph nodes in the central neck of these patients had similar characteristics of hypoechoic round shape without fat hilum.The only difference among this group of lymph nodes was size. Analysis for the cutoff sizes of CLN as measured by ultrasound that may predict CLN metastasis of PTC is shown in Table 3 and Figure 3. The size of the CLN is the largest lymph node in each patient, as measured by ultrasound in 34 patients.The size of CLN that was most commonly found was 5 mm, and the smallest size of CLN that was found to be positive by histopathology was 3 mm. The incidence of CLN metastasis increased as the size of the CLN increased, and all the central lymph nodes that were larger than 5 mm in size were histopathologically confirmed to be CLN metastasis. All of CLN detected by ultrasound from 34 patients were 63 nodes. The incidence of pathologic involvement of lymph nodes of various sizes is shown in Figure 4.
Analysis for the Cutoff Sizes of Central Lymph Node as Measured by Ultrasound That May Predict Central Lymph Node Metastasis of Papillary Thyroid Carcinoma.
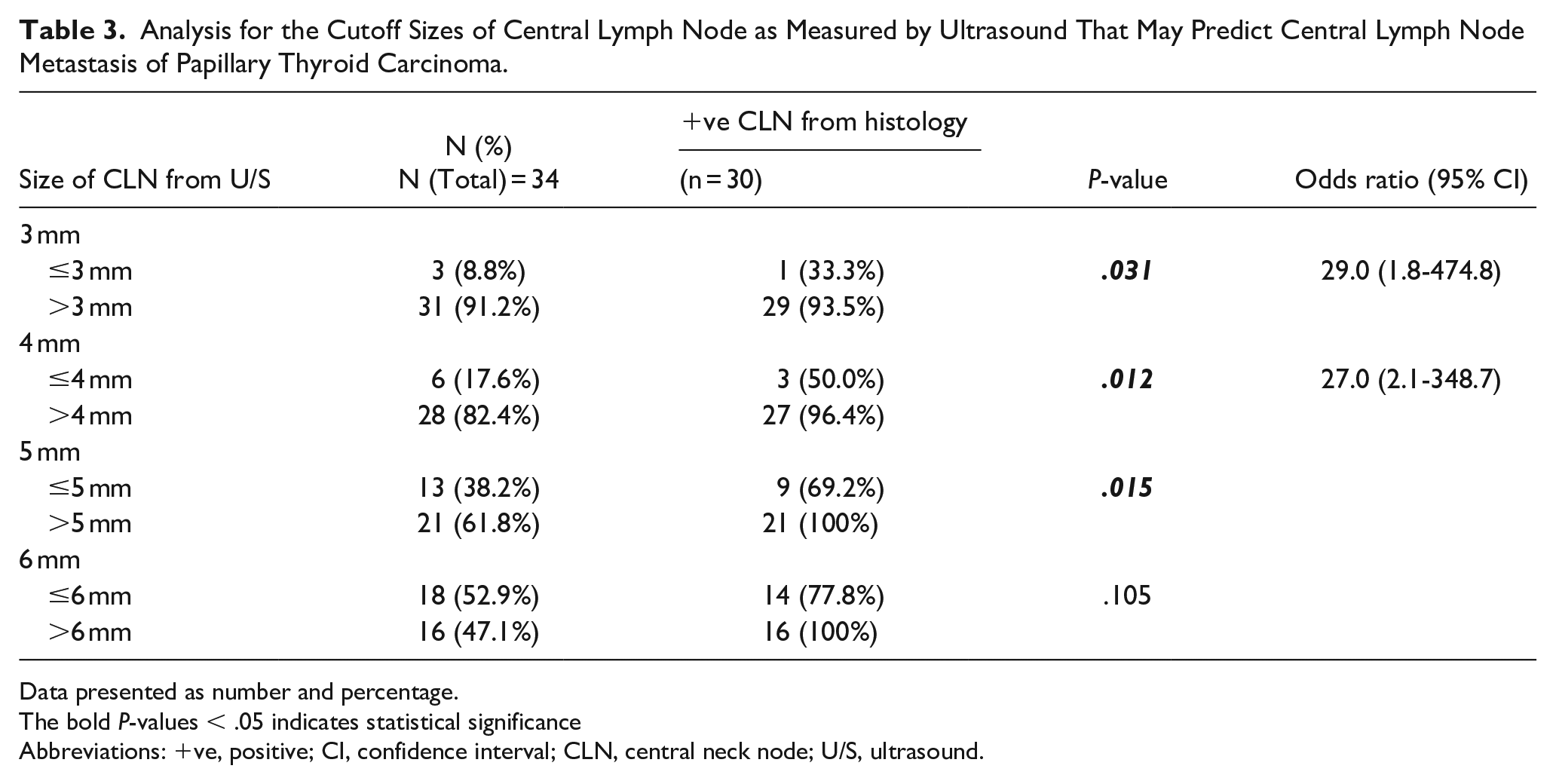
Data presented as number and percentage.
The bold P-values < .05 indicates statistical significance
Abbreviations: +ve, positive; CI, confidence interval; CLN, central neck node; U/S, ultrasound.
Incidence of central lymph node (CLN) metastasis for the largest lymph node size for each patient as measured by ultrasound.
Incidence of central lymph node (CLN) metastasis for a total of 63 CLN for each lymph node size as measured by ultrasound from 34 patients.
Probable risk factors for CLN metastasis were reviewed in patients who underwent CND (Table 4). Twenty-four of the 48 cases had preoperative positive lateral lymph node, and all 24 (100%) of those cases were found to be positive for CLN metastasis from histopathologic analysis. Among the 24 patients with preoperative negative lateral lymph node, 17 (70.8%) patients were confirmed as having positive CLN metastasis. The differences were statistically significant (P = .009). Four of the 48 (8.3%) patients had a thyroid tumor of size ≥4 cm, and all 4 (100%) of those patients were positive for CLN metastasis. Among the patients with a thyroid tumor of size <4 cm, there were 37/44 (84.1%) cases positive for CLN metastasis (P = 1.00).
Analysis for Probable Risk Factors for Central Lymph Node Metastasis of Papillary Thyroid Carcinoma.
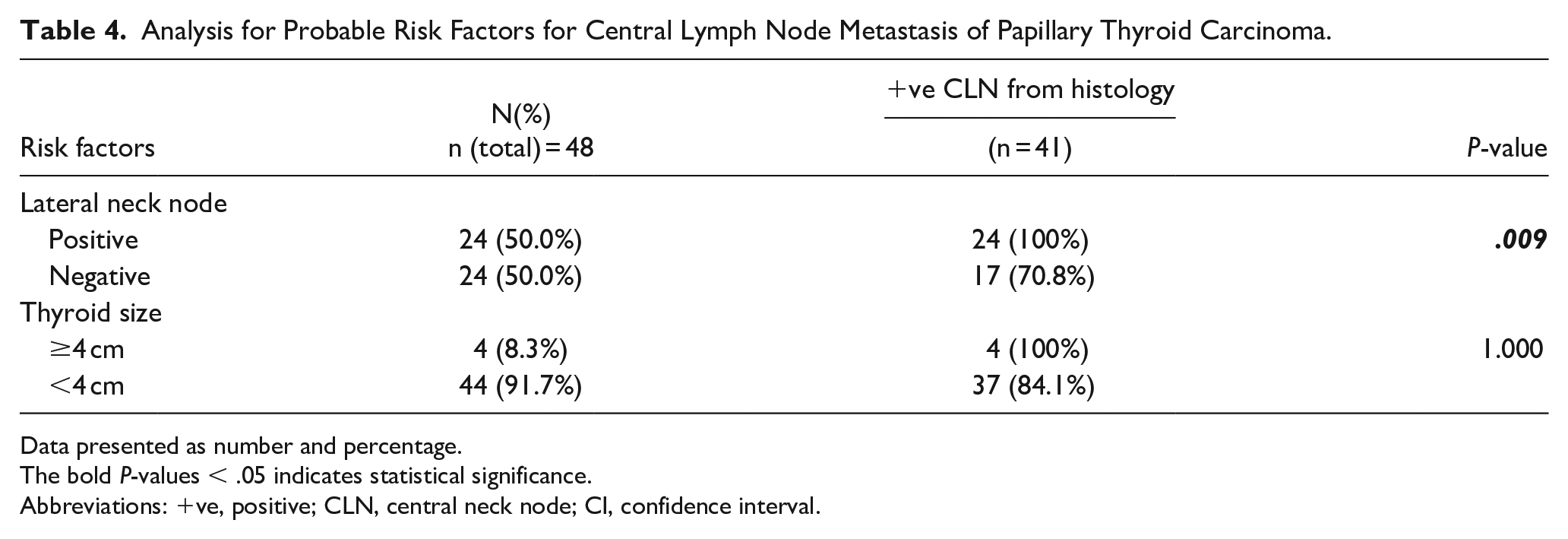
Data presented as number and percentage.
The bold P-values < .05 indicates statistical significance.
Abbreviations: +ve, positive; CLN, central neck node; CI, confidence interval.
Discussion
The prevalence of CLN metastasis of PTC was reported to range from 30% to 68%,6-8,16 however, the definite indications for CND are still being debated. 8 The decision to resect these lymph nodes at the time of thyroidectomy often depends on preoperative suspicion of nodal metastasis. In routine clinical practice at our center, we perform CND in patients with large thyroid nodule(s) (≥4 cm), clinically positive lateral neck node, intraoperative palpable CLN, or positive CLN by ultrasound. The sensitivity, specificity, PPV, NPV, and accuracy of ultrasound for detecting CLN metastasis of PTC were reported to be 30%-69%, 71%-90%, 76%-84%, 51%-63%, and 66%, respectively.14-17 In the present study, we found the PPV, NPV, and accuracy to be 88.0%, 21.0%, and 68.7%, respectively. The 3 out of 4 patients with positive nodes by ultrasound but negative CLN metastasis by histology were associated with chronic lymphocytic thyroiditis. Preoperative ultrasound for patients with chronic lymphocytic thyroiditis had a higher number of total cervical lymph nodes than the euthyroid patients with goiter. 18 Compared with PTC patients without chronic lymphocytic thyroiditis, the preoperative ultrasound for CLN displays a higher false-positive rate (27.9% vs 12.2%, P < 0.001) and a lower specificity (72.1% vs 87.8%, P < .001) in PTC patients with chronic lymphocytic thyroiditis. 19 In our study, 3/9 cases (33.3%) had chronic lympocytic thyroiditis,while only 1/25 case (4%) without chronic lymphocytic thyroiditis had false-positive preoperative ultrasound for CLN. There were 14 patients who had a negative preoperative ultrasound result, but they still underwent CND due to their being determined to be at high risk for CLN metastasis. CLN metastasis was found in 11 patients in this group. The NPV of ultrasound at the central neck area is not very high, perhaps because lymph nodes in this area are more difficult to see by ultrasound when compared to the lateral neck due to their proximity to the thyroid gland and trachea. Combination ultrasound and computed tomography yielded significantly higher sensitivity for macroscopic lymph node detection in both the lateral and central neck. 7 The risk factor for CLN metastasis that we identified in this study was positive lateral lymph node by preoperative ultrasound (P = .003). The patients who had positive lateral lymph node had positive CLN metastasis in all cases. In previous studies, skipped metastasis to the lateral compartment lymph nodes occurred in 7.4%-9.7% of patients.20,21 In our study, size of thyroid tumor ≥4 cm from ultrasound was not found to be a significant risk factor for CLN metastasis (P = 1.00). All of our patients with a thyroid tumor ≥4 cm had histologically proven CLN metastasis, but 83% of thyroid tumors <4 cm also had histologically proven CLN metastasis. This suggested that a tumor size ≥4 cm was highly predictive of CLN metastasis, but the rate of CLN metastasis remained high in tumor sizes <4 cm. This result may be due to the inclusion of only high risk of CLN metastasis or positive CLN by ultrasound in this study. Some studies reported that the risk of CLN metastasis increased when the size of the PTC was >1 to 2 cm.5,22 The ATA 2015 and the European Society of Endocrine Surgeons 2014 recommend CND in PTC for T3/T4 tumors (size >4 cm or extrathyroidal extension).10,13 Preoperatively, patients should undergo clinical neck examination in combination with neck ultrasound to detect any lymph nodes of concern. High-resolution cervical ultrasound was reported to be the most sensitive method for detecting metastatic lymph nodes as small as 2 to 3 mm. 7 In our study, the smallest CLN detected by ultrasound was 2 mm. There was a high PPV in detecting CLN metastasis by ultrasound. The precision of the ultrasound increased as the size of CLN increased. Ultrasound was found to be an effective preoperative evaluation, especially for CLN ≥ 5 mm. In case of high risk of CLN metastasis group, CND should also be considered even if CLN was negative by ultrasound because NPV of ultrasound was not very high. The previous study described the ultrasound characteristics of cervical lymph nodes that had a high risk for metastasis in papillary thyroid cancer, including cystic change, hyperechogenicity, loss of fat hilum, internal calcifications, size >5 mm, and round shape. 23 Using a CLN size of greater than 5 mm as an indicator of metastasis, preoperative ultrasound had 58.3% sensitivity and 71.4% specificity for detecting CLN metastasis. 24 In our study, almost all CLN had a round shape without fat hilum and no hyperechogenicity. Moreover, we found the smallest size of metastatic CLN from preoperative ultrasound to be 0.3 mm. The risk of CLN metastasis of PTC was 67.7% and 85.7% for lymph node size 3.1 to 4 mm and 4.1 to 5 mm respectively, and the risk increased to 100% when the size was >5 mm. The result was similar when we included all of the 63 lymph nodes detected by ultrasound from 34 patients. Therefore, CND should be considered when CLN size is ≥3 mm, and is highly recommended in nodes ≥5 mm in size.
Limitations
This study has some mentionable limitations consistent with the data-related vulnerability of the retrospective study design; data specific to a negative CLN from ultrasound that underwent CND was not completely recorded. We did not perform CND in all patients, but we did perform CND in all patients who had positive identification from ultrasound, which was the main indication of CND in this study. As such, the incidence of central node metastasis in cases with lateral node positivity or tumors ≥4 cm might be higher than usual.
Conclusions
Ultrasound was found to be an effective preoperative evaluation in patients with PTC to determine the likelihood of CLN metastasis and whether CND is indicated, especially in the ultrasound-positive central lymph node. A high risk of metastasis was found in CLN size ≥3 mm by ultrasound, and the risk dramatically increased in CLN size ≥5 mm. We also found positive lateral neck node from preoperative ultrasound to be a significant risk factor for CLN metastasis.
Footnotes
Acknowledgements
The authors gratefully acknowledge Clinical Professor Cheerasook Chongkolwatana, MD and Associate Professor Kitirat Ungkanont, MD for their advice and other helpful contributions to this study and Miss Jeerapa Kerdnoppakhun for her assistance with article preparation.
Availability of Data and Materials
The original data are available in the form of SPSS. If the editor and reviewer need the author’s description of any parts of the article, I could answer and attach the file later.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.